
Abstract
Purpose:
Diabetes mellitus is a global epidemic and one of the leading causes of morbidity and mortality. Additional medications that are novel, affordable, and efficacious are needed to treat this rampant disease. This meta-analysis was performed to ascertain the effectiveness of oral aloe vera consumption on the reduction of fasting blood glucose (FBG) and hemoglobin A1c (HbA1c).
Methods:
PubMed, CINAHL, Natural Medicines Comprehensive Database, and Natural Standard databases were searched. Studies of aloe vera's effect on FBG, HbA1c, homeostasis model assessment-estimated insulin resistance (HOMA-IR), fasting serum insulin, fructosamine, and oral glucose tolerance test (OGTT) in prediabetic and diabetic populations were examined. After data extraction, the parameters of FBG and HbA1c had appropriate data for meta-analyses. Extracted data were verified and then analyzed by StatsDirect Statistical Software. Reductions of FBG and HbA1c were reported as the weighted mean differences from baseline, calculated by a random-effects model with 95% confidence intervals. Subgroup analyses to determine clinical and statistical heterogeneity were also performed. Publication bias was assessed by using the Egger bias statistic.
Results:
Nine studies were included in the FBG parameter (n = 283); 5 of these studies included HbA1c data (n = 89). Aloe vera decreased FBG by 46.6 mg/dL (p < 0.0001) and HbA1c by 1.05% (p = 0.004). Significant reductions of both endpoints were maintained in all subgroup analyses. Additionally, the data suggest that patients with an FBG ≥200 mg/dL may see a greater benefit. A mean FBG reduction of 109.9 mg/dL was observed in this population (p ≤ 0.0001). The Egger statistic showed publication bias with FBG but not with HbA1c (p = 0.010 and p = 0.602, respectively).
Conclusion:
These results support the use of oral aloe vera for significantly reducing FBG (46.6 mg/dL) and HbA1c (1.05%). Further clinical studies that are more robust and better controlled are warranted to further explore these findings.
Introduction
T
Individuals diagnosed with DM are also 1.6 times more likely to seek complementary and alternative medicine than those without DM. 7 In fact, it has been estimated that up to 49% of diabetics have taken dietary supplements or used another form of complementary and alternative medicine in an effort to treat their DM or other health condition. 8 One of these remedies that is frequently sought is the topical use or oral consumption of aloe vera (Aloe barbadensis) (Fig. 1). 9

Aloe vera (Aloe barbadensis). Photo credit: Dharam Vasnani, PharmD.
The leaves of the aloe vera plant comprise two major components: the green outer rind, which includes the vascular bundles, and the colorless inner gel-like parenchyma. 9 The vascular bundles, or peripheral bundle sheath cells, are a yellowish color and are found between the outer rind and the inner parenchyma. Aloe vera products are derived from one or both of the major components or portions of them. The vascular bundles contain an extremely bitter sap-like substance that is often referred to as aloe latex or sap and contains high amounts of anthraquinones, which produce pronounced diarrhea when ingested. 10,11 Aloe vera leaf juice is derived from the whole leaf and in most cases is cleansed of aloin, the principal anthraquinone responsible for the laxative effect. Aloe vera gel is made from the inner gel fillet, which can also be juiced to produce inner fillet juice. Both juice products can be concentrated or converted to a powder form as well. 10
On the basis of folk medicine, the people of Greece, Egypt, India, Mexico, Japan, and China have used aloe vera for a variety of medicinal purposes for thousands of years. 12 In more recent history, the topical use of aloe vera has been found to be useful in the treatment for seborrheic dermatitis, psoriasis vulgaris, and genital herpes; oral formulations have been used as a laxative. 13 Limited or inconsistent evidence supports the ingestion of aloe vera consumption for the treatment of chronic diseases, such as asthma, glaucoma, dyslipidemia, hypertension, osteoarthritis, inflammatory bowel disease, and DM. 7 However, data are increasing with regard to the treatment of DM because oral consumption of aloe vera has been found to lower blood glucose and its use in traditional medicine is becoming more common. 14,15
Several studies have sought to measure the effect of aloe vera ingestion on diabetic parameters, with varying or contradictory results. A systematic review performed in 1999 by Vogler and Ernst found that oral administration of aloe vera to decrease blood glucose might be effective but that the evidence should be regarded as preliminary. 12 Another review performed by Ngo et al in 2010 concluded that most evidence suggests that oral aloe vera use may be an effective treatment for DM. However, this review also cautions that given the weaknesses and inconsistencies among the included trials, a use of aloe in treating DM cannot be recommended. 7 Additional studies regarding the effects of oral aloe vera administration on DM have now been completed and substantially contribute to the existing data. Therefore, the current study is the first known meta-analysis on the effectiveness of oral aloe vera dietary supplements on fasting blood glucose (FBG) and hemoglobin A1c (HbA1c).
Materials and Methods
Search strategy and selection
A literature search was conducted in PubMed (1966–November 11, 2014) and CINAHL (1960–November 11, 2014) using the search terms “aloe” AND “diabetes” OR “blood glucose.” The search was limited to clinical trials or observational studies conducted in humans and published in English. A repeat search conducted in PubMed with the same search terms but not limited to humans found that four trials had been erroneously classified as animal studies. 16 –19 These four studies were also included in our analysis. Monographs that contained the word “aloe” in the title and were identified from both the Natural Medicines Comprehensive Database and Natural Standard databases were also researched for additional resources. Published authors in the field of aloe vera and recognized industry experts were also consulted to determine whether any unpublished data were available. Finally, the bibliographies of all found studies were searched for any additional trials not yet found by the aforementioned means.
Studies were included for analysis if they met the following criteria: (1) placebo or active controlled clinical trials, observational studies, or trials that measured the addition of oral aloe vera to an established diabetic medication regimen; (2) studies that reported a change from baseline in the glycemic parameters FBG, HbA1c, homeostasis model assessment-estimated insulin resistance (HOMA-IR), fasting serum insulin, fructosamine, or oral glucose tolerance test; and (3) studies carried out in prediabetic and diabetic patients. Trials were excluded if they were retrospective; available as an abstract only; or had irrelevant, missing, or inappropriately reported data.
Eligibility and data abstraction
Resulting studies were evaluated for appropriateness to criteria by two study researchers (W.R.D. and S.A.S.), with a final review for eligibility made by the third investigator (E.A.F.). Data were then abstracted with the use of a standardized data abstraction tool by the primary author and independently checked for correctness by the other two study researchers (E.A.F. and S.A.S.). The following were extracted from each article: principal author, country of study origin, year of publication, aloe product used and dose, duration of study, patient population, and all endpoint data (including change from baseline and standard error of the mean [SEM] or standard deviation [SD] if provided). After completion of data abstraction, it was determined that only the endpoints of FBG and HbA1c had sufficient data to include in our meta-analysis.
Statistical analysis
Changes in FBG and HbA1c were assessed as the weighted mean differences (WMD) from baseline. A DerSimonian-Laird random effects model was used to calculate the WMD with a 95% confidence interval (CI). In cases where only SEM was reported, it was converted to SD (SEM = SD/√[sample size]) before calculations. All analyses were performed using StatsDirect software, version 2.8.0 (StatsDirect Ltd, Cheshire, United Kingdom).
Several subgroup analyses were also performed to assess clinical and statistical heterogeneity. The latter was gauged by using the I2 statistic. FBG and HbA1c WMDs from baseline were also evaluated by using a Mulrow-Oxman fixed-effects model even though results were reported with a random-effects model, which showed a more conservative treatment effect.
The Egger bias statistic, along with visual inspection of funnel plots, was used to assess publication bias.
Results
Included studies
The initial literature search identified 205 studies. After the inclusion and exclusion criteria were applied, there were a total of 9 unique studies for meta-analysis (Fig. 2). 16 –19,20 –24 All 9 trials had data for the FBG parameter (n = 283), while only 5 trials 17,20,21,23,24 had data for the HbA1c parameter (n = 89).

Study selection method. FBG, fasting blood glucose; HbA1c, hemoglobin A1c.
The characteristics of included trials are listed in Table 1. Three trials administered aloe vera juice preparations, 18,19,24 1 used aloe gel consumption, 17 4 used powdered aloe gel capsules, 16,20 –22 and 1 used dried aloe latex resin. 23 Two of the trials that administered powdered aloe gel capsules used commercially produced products 20 or an aloe supplement that contained an additional bioactive ingredient. 22
BID, two times daily; FBG, fasting blood glucose; BMI, body–mass index; OGTT, oral glucose tolerance test; TG, triglyceride; HDL, high-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; TID, three times daily.
Meta-analysis results
Oral aloe vera use significantly decreased FBG by 46.6 mg/dL (95% CI, −66.54 to −26.74 mg/dl; I2 = 97.6) (Fig. 3). HbA1c was also significantly decreased by 1.05% (95% CI, −1.78% to −0.33%; I2 = 90.9) (Fig. 4). The Egger statistic showed publication bias with FBG but not with HbA1c (p = 0.010 and p = 0.602, respectively). A lack of publication bias cannot be ruled out upon visual inspection of the funnel plots (Fig 5A and B).
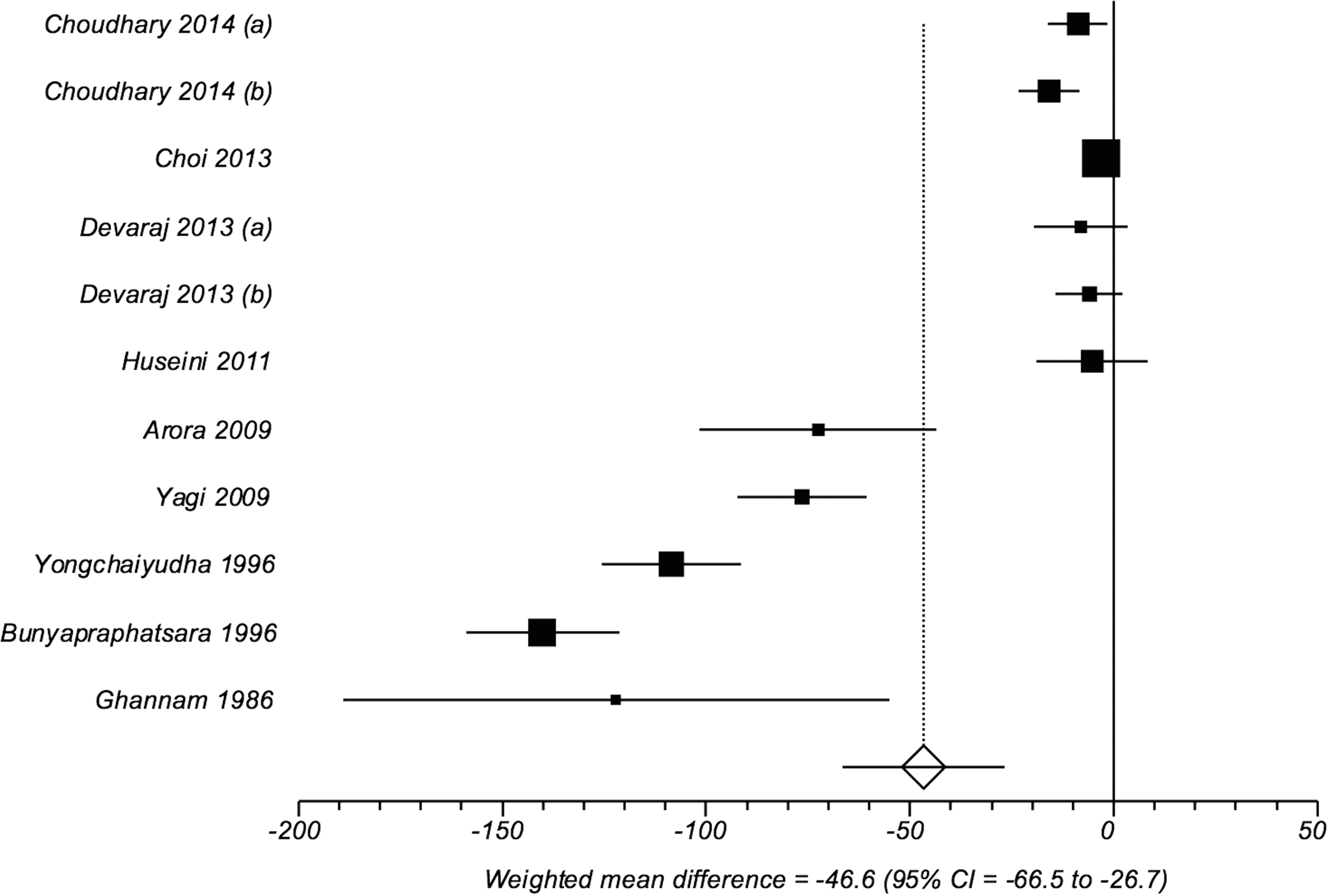
Change in FBG from baseline. CI, confidence interval.
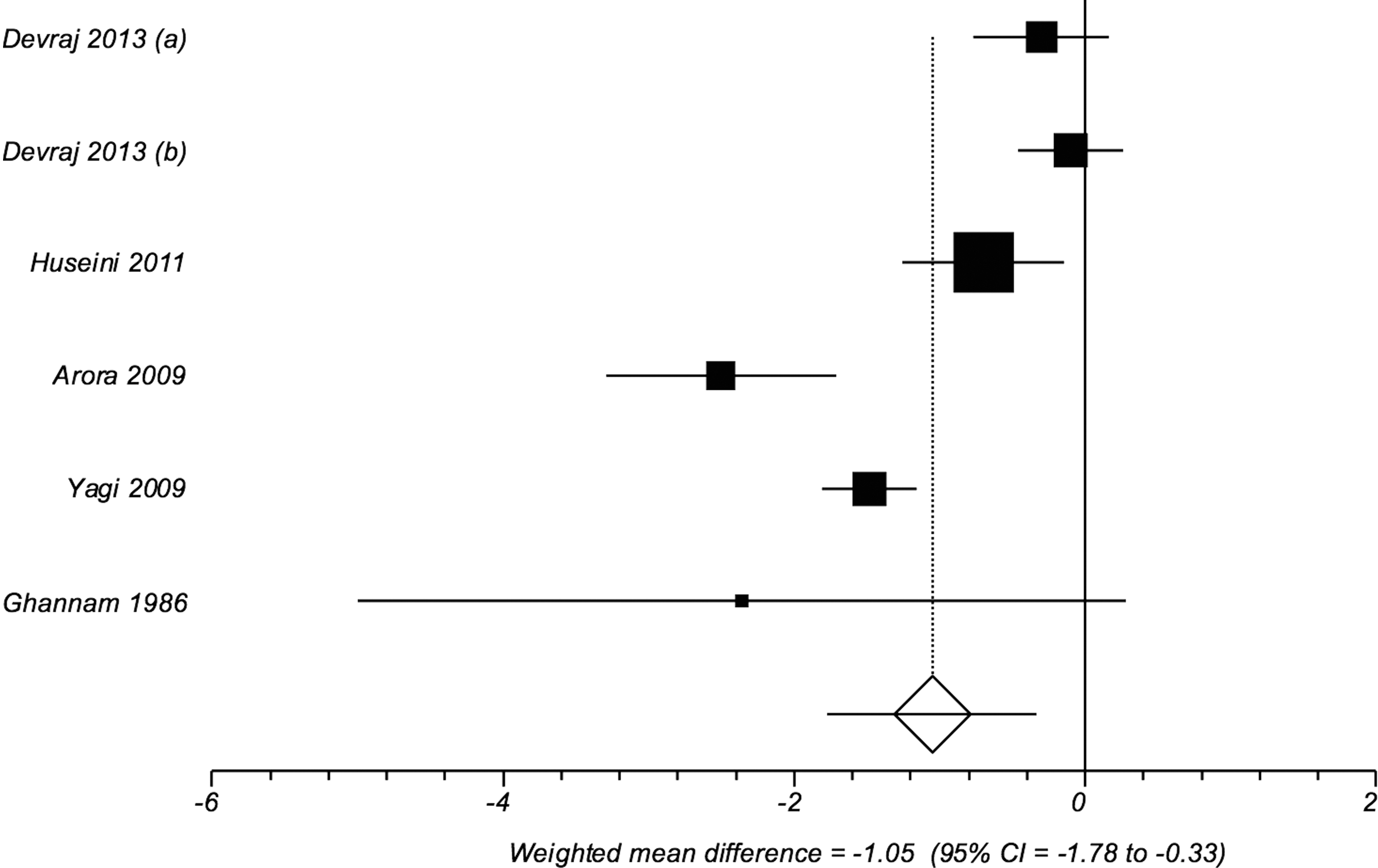
Change in HbA1c from baseline.
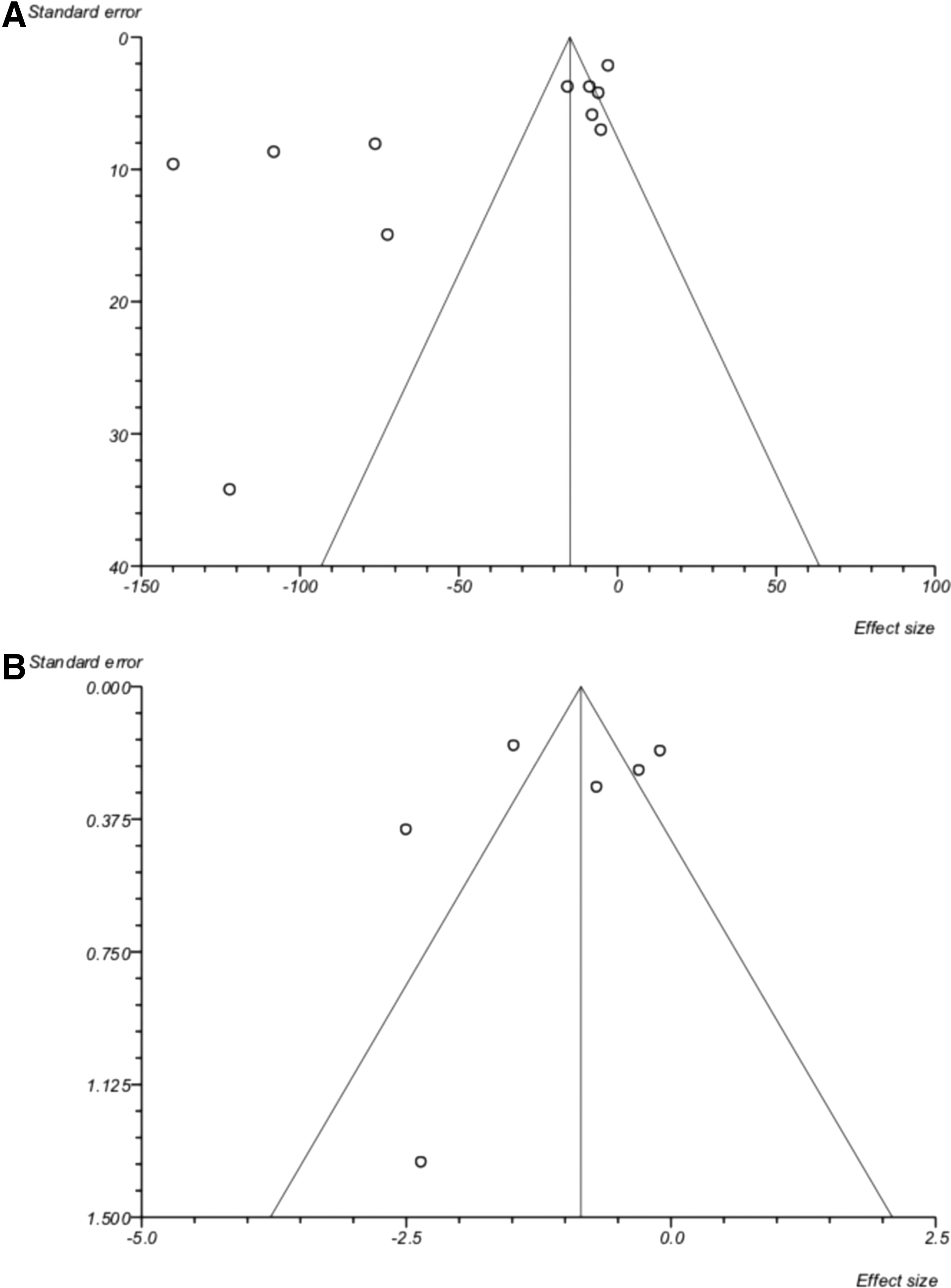
Funnel plots.
Significant reductions in both endpoints were maintained in subgroup analyses. A study by Ghannam et al. suggested a substantially greater benefit (large CI) in both endpoints than the other included trials. 23 Upon exclusion of this study from the overall analyses for FBG and HbA1c, the significant benefits were still sustained (WMD, −42.9 mg/dL [95% CI, −63.09 to −22.70 mg/dL]; WMD, −0.98% [95% CI, −1.72% to −0.23%], respectively).
Another subgroup analysis was completed to identify populations that might benefit more from oral aloe vera administration. This analysis was performed using 4 trials, whose populations had a FBG ≥200 mg/dL at baseline. 17 –19,23 This population experienced mean FBG reductions of 109.9 mg/dL (95% CI, −142.1 to −77.7 mg/dL).
Conversely, a significant reduction in FBG of 7.62 mg/dL (95% CI, −11.94 to −3.29 mg/dL) was also maintained in a subgroup of 4 trials in which the baseline FBG was <200 mg/dL. 16,20 –22 One study by Arora et al. was excluded for having a much greater reduction in FBG than the other trials that included patients with a baseline FBG <200 mg/dL. 24 All analyses, including subgroup analyses, maintained significance when a Mulrow-Oxman fixed-effects model was used.
Discussion
These results suggest a significant benefit on FBG and HbA1c with oral consumption of aloe vera. The exact mechanism by which consumption of aloe vera can lower blood glucose and the specific active component responsible for these benefits remain unknown. Many animal studies have confirmed the antidiabetic effects of aloe vera and have proposed mechanisms by which this may occur. In studies that used streptozotocin or alloxan diabetic rats or mice, reduced blood glucose, 25,26 increased serum insulin concentrations, 27 decreased insulin resistance, 28,29 reduced FBG, 30 or increased liver gluconeogenesis 31 have been documented after oral administration of aloe vera. The use of Zucker diabetic fatty rats in a trial where oral aloe vera was administered specifically found that the expression of the genes related to glucose metabolism were altered. 32 In another study, obese mice fed an aloe vera complex decreased insulin resistance by activation of adenosine monophosphate–activated muscle protein kinase, which contributes to the regulation of glucose metabolism. 33 Although no exact mechanisms by which aloe vera reduces FBG and HbA1c in humans have been proposed, the animal studies provide some working hypotheses.
More research is also needed to surmise what compounds within aloe vera are responsible for the reductions of FBG and HbA1c. The aloe vera plant contains at least 75 active compounds, which notably include vitamins, enzymes, minerals, anthraquinones, monosaccharide, polysaccharides, lignin, saponins, salicylic acids, phytosterols, and amino acids. 9,34 The trace elements of chromium, magnesium, manganese, and zinc are important in the metabolism of glucose by improving the effectiveness of insulin and are also contained in aloe vera. 35,36 A trial conducted by Arora and associates hypothesized that it was the high polysaccharide content of the aloe vera product in their study that was responsible for the favorable effects on FBG and HbA1c. 24 Three additional studies specifically name acemannan, a polysaccharide, as the active component that was thought to be responsible for the reductions of FBG and/or HbA1c seen in their respective trials. 17,20,21 Conversely, a study performed by Tanaka et al. proposed that the phytosterols contained within aloe are responsible for improved blood glucose control. 26
Another area with limited data is the evaluation of the long-term safety of aloe vera supplementation. However, the information currently available is promising. Mice and rat studies reveal no toxicities associated with acute or subchronic therapeutic doses. 17,37 Five of the studies included in our analysis showed that aloe vera did not cause any hepatic or renal adverse effects. 17 –21 Contrarily, some case reports found acute hepatitis and thyroid dysfunction after supplementation with aloe vera, so the risk cannot be entirely ruled out. 38 –40 The adverse effects that are possible with ingestion of aloe vera include abdominal pain and cramping, diarrhea, muscle weakness, and low blood glucose. 41 One source also recommends against its use during pregnancy. 11 Besides safety, purity of product is also of concern. Currently, only three aloe vera product manufacturers (Aloecorp, Lacey, WA; Pharmachem Laboratories, Kearny, NJ; Terry Laboratories, Melbourne, FL) have “generally recognized as safe” status. 42 –44 Furthermore, product certification by the International Aloe Science Council would also provide confidence in the purity and overall manufacturing quality of the aloe product. 45
Although the results of this meta-analysis appear favorable, several inherent limitations are worthy of mention. Different formulations and doses of aloe vera products were used in all but two trials. 18,19 Because of the lack of standardization, it is difficult to ascertain which products would be comparable and efficacious. Because weight-related changes were not reported, an analysis as such could not be performed. The duration of these aloe interventions also varied from 4 to 14 weeks. Moreover, it is problematic that many of the trials differed in their control for concomitant medications or supplements, use of blinding or randomization, or measuring of adherence. Small sample size was a limitation in all included trials. The I2 statistic showed significant heterogeneity for both endpoints. However, seeing the differences in the magnitude of benefit in the subgroup of patients with FBG ≥200 mg/dL compared to <200 mg/dL suggests that baseline FBG was the driving factor. Because this analysis looked only at articles published in the English language, it is possible that articles published in other languages may change the outcome of the findings.
Because less than half of patients with type 2 diabetes have their disease well controlled 46 and adequate treatment is often limited by unfavorable side effects, 17 additional investigation into the use of oral aloe vera as an antidiabetic compound is needed. This is especially true as aloe may represent an efficacious and more affordable treatment option with fewer side effects experienced when compared with traditional therapies. 17,47
Conclusion
The results of this meta-analysis support the use of oral aloe vera for significantly reducing both FBG (46.6 mg/dL) and HbA1c (1.05%) in prediabetic and diabetic patients. However, given the current overall quality and relative scarcity of data, further clinical studies that are more robust and better controlled are warranted to confirm and further explore these findings.
Footnotes
Acknowledgments
No funds were used in the completion of this analysis. The views expressed in this material are those of the authors and do not reflect the official policy or position of the U.S. government, the Department of Defense, or the Department of the Air Force.
Author Disclosure Statement
No competing financial interests exist.