
Abstract
Objective:
Combined idiopathic pulmonary fibrosis with pulmonary emphysema (CPFE) is a syndrome with a characteristic presentation of upper lobe emphysema and lower lobe fibrosis. Dyspnea on exertion (DOE) is a major symptom of CPFE. We report a patient with DOE due to CPFE who was successfully treated with acupuncture.
Design:
Case report.
Case presentation:
A 72-year-old Japanese man with a 4-year history of DOE was diagnosed with CPFE 2 years previously in another hospital. He received standard Western medicine treatment, which included bronchodilators. However, his DOE did not improve. Consequently, he visited our hospital for acupuncture treatment and received acupuncture treatment once a week for 1 year.
Results:
After 10 weeks of acupuncture treatment, the results of the 6-minute walk test (6-minute walking distance, 379 m; lowest oxygen saturation, 86%; modified Borg dyspnea scale score: 2 units) were better than those at baseline (352 m, 84%, 4 units, respectively). These values were sustained at both 30 weeks (470 m, 88%, 1 unit) and 60 weeks (473 m, 85%, 2 units). Serum interstitial biomarkers, Krebs von den Lungen and surfactant protein-D, decreased after commencement of acupuncture therapy.
Conclusion:
A patient with CPFE showed improvements in dyspnea scores, exercise tolerance, and serum biomarkers during a 1-year course of acupuncture treatment. Use of acupuncture might be an effective adjunct therapy in relieving DOE due to CPFE. A large, well-designed cohort study that includes patients with CPFE treated with acupuncture should be conducted.
Introduction
C
Acupuncture is a major component of traditional Eastern medicine and has reduced breathlessness in patients with chronic obstructive pulmonary disease (COPD) 4 –7 and cancer. 8 Transcutaneous electrical nerve stimulation over acupuncture points has been reported to reduce dyspnea and consequently improve the forced expiratory volume in 1 second (FEV1) by increasing β-endorphin levels in patients with COPD. 9 Suzuki et al. demonstrated that acupuncture is a useful adjunctive therapy to reduce dyspnea on exertion (DOE) in patients with COPD. 4 –6 Acupuncture can be beneficial as an adjunct to standard pharmacologic therapy in patients with respiratory disease, including COPD and CPFE.
However, to the best of our knowledge, acupuncture to treat dyspnea in patients with CPFE has not been reported. We describe a patient with CPFE who was successfully treated for DOE by acupuncture.
Case Presentation
The patient was a 72-year-old Japanese man with a 4-year history of DOE who was diagnosed with CPFE 2 years previously at another hospital. He received standard Western medicine treatment, including a combination of inhaled corticosteroids (ICS; 640 μg/d), long-acting β-agonist (LABA; 18 μg/d), and long-acting anti-muscarinic agent (LAMA; 50 μg/d). Other Western medicine treatments included rehabilitation twice per week for 1 year and home oxygen therapy during the night (at 0.5 L/min) for 6 months in another clinic. However, his DOE did not improve. Thus, he visited our hospital to receive acupuncture treatment.
He had a medical history of hypertension, dyslipidemia, reflex esophagitis, and candida esophagitis and a smoking history of 40 pack-years; he had stopped smoking when he was 40 years old when a pulmonary bulla was observed during a medical check-up.
Clinical data at baseline (before acupuncture was started) are shown below. Clinical examination demonstrated fine Velcro-like crackles of the lung at the base of the back. The patient's body weight was 64 kg, and his body–mass index was 21.9 kg/m2. During palpation, the muscle tone was increased in the accessory respiratory muscles, including the smaller pectoral, sternocleidomastoid, and scalene muscles.
Shortness of breath at rest was observed, and his respiratory rate was 23 breaths/min. On occasion, dry cough was observed. On the 6-minute walk test (6-MWT), 10 oxygen saturation (SpO2) decreased 11 percentage points (from 95% to 84%) and the 6-minute walking distance (6-MWD) was 352 m; the modified Borg scale 11 for scoring DOE was 4 units (Table 1).
VC, vital capacity; RV, residual volume; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; CV, closing volume; ΔN2, the slope of phase 3 of the single-breath nitrogen test; DL
His chest radiograph and computed tomography images are shown in Figures 1 and 2. Emphysema in the upper lobe and fibrosis in the lower lobe were observed. Variables in the respiratory function test at baseline are shown in Table 1. The test showed an FEV1 of 110.7% predicted, a forced vital capacity (FVC) of 92.5% predicted, and a diffusing capacity in the lung for carbon monoxide of 55.2% predicted.

Chest radiograph.

Chest computed tomographic images. Emphysema in upper lobe
The serum levels of surfactant protein-D (SP-D) and Krebs von den Lungen (KL-6) 12 were higher (211.0 ng/mL and 1212 U/mL, respectively) than the normal limit (110 ng/mL and 500 U/mL, respectively) (Table 1). White blood cell counts (7750 cells/μL) and C-reactive protein levels (0.16 mg/dL) were within the normal limits (3400–9200 cells/μL and <0.20 mg/dL, respectively). However, red blood cell counts (385 × 104 cells/μL) and hemoglobin levels (12.2 g/dL) were slightly lower than normal limits (399–566 × 104 cells/μL and 12.9–17.2 g/dL).
Acupuncture treatment was conducted once a week for 61 weeks by an experienced acupuncturist who had been in clinical practice for over 10 years. Acupuncture points used for the study patient were LU 1, LU 7, ST 36, KI 3, CV 12, CV 4, BL 13, BL 17, BL 20, and BL 23. CV 22 and KI 7 were later added at 4 and 10 weeks for a dry cough that had developed. The location of these acupuncture points were in accordance with the World Health Organization standard textbook. 13 These acupuncture points were mainly chosen after consideration of previous reports of acupuncture for COPD and the Traditional Chinese Medicine theory. 4 –7,14 Acupuncture at points LU 1, CV 4, CV 12, ST 36, KI 3, BL 13, BL 20, and BL 23 improves DOE and 6-MWD, respiratory function test results (e.g., FEV1/FVC), and quality of life. 4 –6 LU 1, CV 12, CV 4, and BL 13 were also selected because these points are close to the respiratory accessory muscles. 4 –6 ST 36, KI 3, and K I7 were selected for qi and yin deficiency as per the Traditional Chinese Medicine diagnosis. LU 1, ST 36, KI 3, CV 12, CV 4, BL 13, BL 17, and BL 23 were selected to modulate the lung, digestive system, and kidney as per the Traditional Chinese Medicine theory. KI 7 and CV 22 were later added at 4 and 10 weeks for a dry cough. In addition, GB 20 was used at 3 weeks for head heaviness and ST 25 during weeks 45–52 for constipation. Disposable stainless steel acupuncture needles (0.16 mm in diameter, 40 mm in length) were inserted to a depth of 4–20 mm, depending on the thickness of the skin and subcutaneous fatty tissue, and were left for 10 min without manipulation.
Previous medical treatments prescribed in another hospital were continued after acupuncture was started. After 5 weeks of acupuncture treatment, ICS was stopped because the patient developed esophageal candidiasis, probably an adverse effect of the treatment. Consequently, he received an antifungal medicine for 7 days. In addition, trimebutine maleate was prescribed at another hospital because he experienced loss of appetite 5 weeks after acupuncture treatment was started. The other inhaled agents, LABA and LAMA, were continued at the same dose throughout the acupuncture treatment period.
To evaluate the effects of acupuncture, the 6-MWT, 10 the respiratory function test, and the blood test for interstitial biomarkers (which included KL-6 and SP-D) were performed approximately every 10 weeks. SpO2 at 1-minute intervals throughout the 6-MWT was evaluated. To rate breathlessness immediately after 6-MWT, the modified 10-point Borg dyspnea scale, 11 with 0 signifying “nothing at all, barely breathless” and 10 signifying “very, very strong, severely breathless,” was used. The 6-MWT was performed according to the American Thoracic Society guideline, 10 once on the assessment day. Respiratory function tests were performed 1 hour later, after use of bronchodilators.
Results
The changes in SpO2 during 6-MWT at baseline, 11 weeks, and 31 weeks after acupuncture treatment are shown in Figure 3. The variables for 6-MWT and the interstitial makers at every 10 weeks are also shown in Figures 4 and 5, respectively.
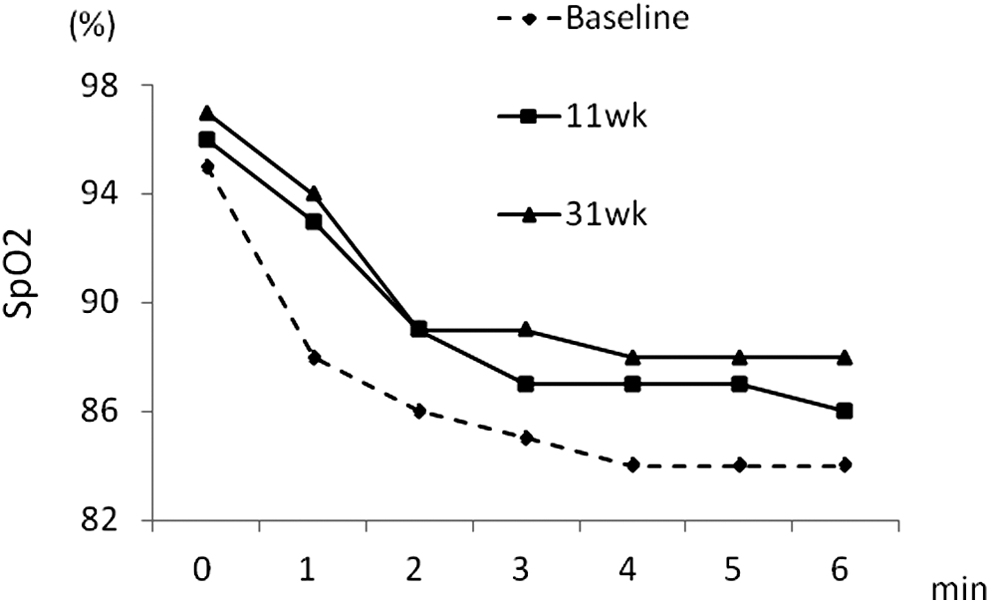
Changes of oxygen saturation (SpO2) during 6-minute walk test at baseline and at 11 weeks and 31 weeks after acupuncture treatment.

Changes in 6-minute walk test.
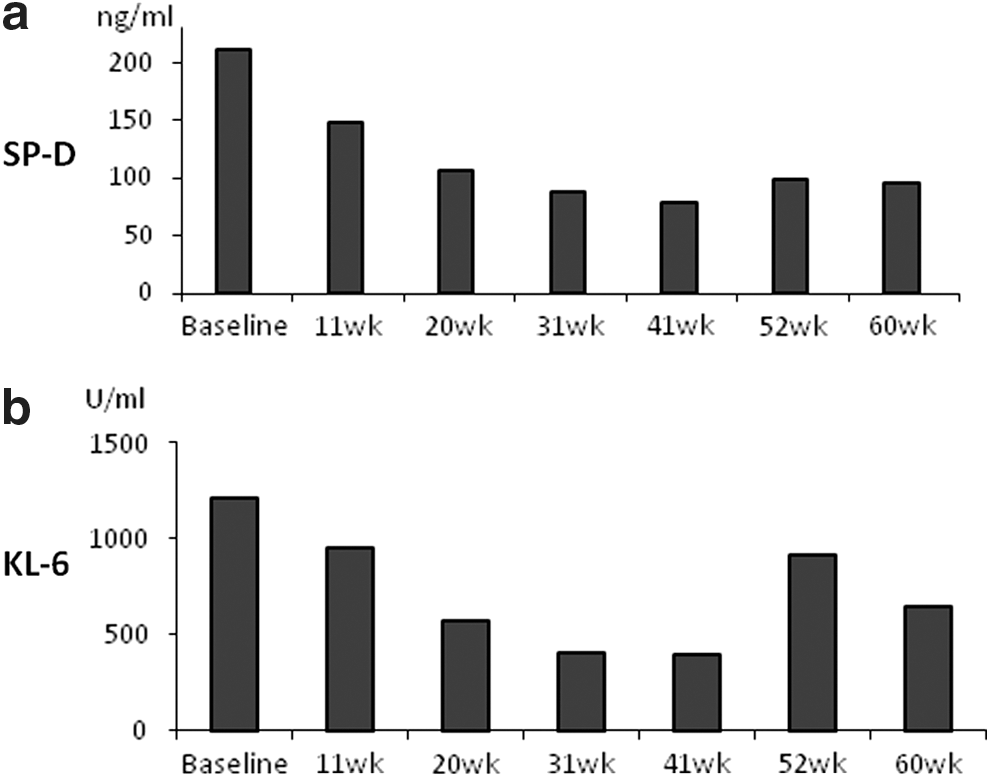
Changes in the interstitial biomarkers.
After two sessions of acupuncture treatment, the patient reported that his DOE during his daily schedule was slightly reduced; his family reported that his walking speed appeared to have increased. After seven sessions of acupuncture, the patient also reported that episodes of dry cough had decreased.
After 10 weeks of acupuncture treatment, DOE decreased further. The results of the 6-MWT after 10 weeks of acupuncture were better than those at baseline. In addition, 6-MWD increased from 352 to 379 m, the lowest SpO2 also increased from 84% to 86% (Fig. 3), and the Borg scale score decreased from 4 to 2 units. Moreover, those improvements in 6-MWT were sustained after 31 weeks (470 m, 88%, 1 unit, respectively) and 61 weeks (473 m, 85%, 2 units) after acupuncture was started (Figs. 3 and 4).
The serum levels of SP-D and KL-6 were also reduced after acupuncture treatment started (Fig. 5). After 20 weeks of acupuncture treatment, the values in SP-D decreased to a level within normal limits (<110 ng/ml) and the value of KL-6 also decreased to within levels of the normal limit (<500 U/mL) after 30 weeks. KL-6 increased temporarily at 50 weeks but showed a reducing trend again at 60 weeks.
The results from the respiratory test are shown in Table 2. Vital capacity, FVC, and FEV1 showed an increasing trend compared with baseline over the long term. However, those values at 11 weeks were temporarily reduced, whereas the values for 6-MWT improved. A gradual reduction in ΔN2 was observed.
Body weight and body–mass index were slightly increased from 64 kg and 21.9 kg/m2 at baseline to 65.0 kg and 22.2 kg/m2, respectively, at 10 weeks; 65.3 kg and 22.3 kg/m2 at 18 weeks; 66.3 kg and 22.7 kg/m2 at 40 weeks; and 65.2 kg and 22.3 kg/m2 at 50 weeks.
The patient's CT images at 3 and 12 months after acupuncture treatment were not remarkably different from baseline images.
Discussion
To the best of our knowledge, there are no reports of patients with CPFE treated with acupuncture, although some reports indicate a beneficial effect on dyspnea in patients with COPD by acupuncture treatment. 4 –7 This is the first description of a beneficial effect of acupuncture in a patient with CPFE.
In the patient, the reduction of the Borg scale score in the 6-MWT started after acupuncture, compared with baseline, and was more than 2 units. It is known that variations of 2 units or more with respect to baseline values are associated with a perceived improvement in sensation. 4,5,15 The increase in the SpO2 during the 6-MWT was observed after acupuncture started compared with baseline. The 6-MWD also increased after acupuncture started compared with baseline. Although the lowest SpO2 during the 6-MWT was reduced to baseline value (84%) 40 weeks after acupuncture commenced, the increase in the 6-MWD (130 m) was sustained for longer compared with baseline. This increase in the 6-MWD score was larger than what has been considered clinically important elsewhere in a review of pulmonary rehabilitation for patients with COPD (from 32 to 55 m) 16,17 and in idiopathic pulmonary fibrosis (from 16 to 55 m). 18 Dyspnea due to hypoxemia at exercise is a characteristic of CPFE, inducing exercise limitation. 1 The noted improvements in the aforementioned indicators strongly suggest that acupuncture was effective in improving exercise capacity and oxygenation, leading to reduced DOE in the patient.
The mechanisms underlying the influence of acupuncture on the respiratory function remains unclear. Although respiratory function tests such as FVC and FEV1 did not consistently improve in the first year of acupuncture treatment, a gradual increase in FVC (by 500 mL) and FEV1 (by 360 mL) in the long term was observed. Predicted FEV1 at baseline was 110.7%, indicating that airflow limitation due to emphysema was not severe and not irreversible in our patient. Therefore, acupuncture treatment might help increase the FEV1 and FVC during the first year of treatment. ΔN2, which indicates changes in the small airways, 19,20 reduced after acupuncture started, suggesting that abnormalities in the small airway were relieved because of acupuncture; this might be the reason for reduced DOE. The mechanical effects of acupuncture are mediated via effects on the autonomic nervous system. 21 Bronchomotor tone is primarily controlled by the parasympathetic nervous system, but it is also affected by stimulation of β-adrenergic receptors in the bronchial smooth muscle. Therefore, we speculated that autonomic functions activated by acupuncture treatment were associated with beneficial effects on respiratory function.
Respiratory muscle strength might be associated with clinical effects because previous reports 4,6 have shown that increased respiratory muscular strength in patients with DOE due to COPD by acupuncture treatment. The reduction of tension in the hypertonic respiratory muscles in the thoracic cage by acupuncture stimulation has been suggested and is thought to be related to improvements in DOE. 4 However, this is unclear because we could not evaluate the respiratory muscle strength or tonus using objective measurement in the present patient.
The reduction of disease activity in pulmonary fibrosis might also be related to the acupuncture effect because reductions in SP-D and KL-6 were observed, which are good indicators of the presence of fibrotic lesions in the lungs of patients with CPFE. 12 In a Chinese report, 22 stimulation with moxibustion at BL13 and BL43 acupuncture points reduced transforming growth factor-β1 mRNA in the pulmonary tissue in rats with bleomycin-induced pulmonary fibrosis as well as prednisone treatment. Similar changes might have occurred and resulted in inhibition of the activity of pulmonary fibrosis in the present patient by using acupuncture stimulation at BL 13, although we did not use moxibustion.
It has been reported that the reduction of dyspnea by stimulation of acupuncture points with transcutaneous electrical nerve stimulation in patients with COPD 9 has been associated with an increase in β-endorphins. The change in endogenous opioid production, such as β-endorphin release, may have been associated with a reduction of DOE in the present patient but this is speculation.
This is only a case report; we cannot come to a solid conclusion regarding the effectiveness of acupuncture. In addition, the effects of rehabilitation and learning might also contribute to the changes in variables of the 6-MWT. Unfortunately, there were no data relating to the 6-MWT, respiratory function, SP-D, and KL-6 before commencement of acupuncture therapy because the patients had regular visits to another clinic. The trends in these objective variables before commencement of acupuncture therapy in our hospital were not clear. The patient's DOE had not improved before commencement of acupuncture therapy, although the rehabilitation continued for 1 year previously. His DOE and certain parameters of the 6-MWT, such as 6-MWD; lowest SpO2; and serum biomarkers tended to improve after commencement of acupuncture therapy. Given these findings, we believe that acupuncture therapy as an adjunct to standard medical care had important clinical effects in this patient.
In conclusion, we describe a patient with CPFE who showed improvements in dyspnea scores, exercise tolerance, and serum biomarkers during a 1-year course of acupuncture treatment. There is no specific treatment for CPFE. Acupuncture treatment may therefore be a beneficial adjunctive therapy in current management strategies. Further long-term effects require to be elucidated in addition to a large cohort study to investigate the effect and the mechanism of acupuncture in patients with CPFE.
Footnotes
Acknowledgment
No competing financial interests exist.