
Abstract
Objective:
To examine the effects of an 8-week yoga program on heart rate variability and mood in generally healthy women.
Design:
Randomized controlled trial.
Participants:
Fifty-two healthy women were randomly assigned to a yoga group or a control group.
Interventions:
Participants in the yoga group completed an 8-week yoga program, which comprised a 60-minute session twice a week. Each session consisted of breathing exercises, yoga pose practice, and supine meditation/relaxation. The control group was instructed not to engage in any yoga practice and to maintain their usual level of physical activity during the study.
Outcome measures:
Participants' heart rate variability, perceived stress, depressive symptoms, and state and trait anxiety were assessed at baseline (week 0) and after the intervention (week 9).
Results:
No measures of heart rate variability changed significantly in either the yoga or control group after intervention. State anxiety was reduced significantly in the yoga group but not in the control group. No significant changes were noted in perceived stress, depression, or trait anxiety in either group.
Conclusions:
An 8-week yoga program was not sufficient to improve heart rate variability. However, such a program appears to be effective in reducing state anxiety in generally healthy women. Future research should involve longer periods of yoga training, include heart rate variability measures both at rest and during yoga practice, and enroll women with higher levels of stress and trait anxiety.
Introduction
W
Yoga has received considerable attention for its therapeutic benefits over the past few decades. 5 It has been associated with increased positive mood and decreased stress and benefits many stress-related disorders, such as depression and anxiety. 6 –11 In women, yoga practice relieves stress in those who are pregnant, 12,13 have mental distress, 14 and have restless legs syndrome. 15 Yoga practice was also effective in reducing symptoms of depression in women with elevated depressive symptoms, 16 breast cancer, 17,18 and menstrual irregularities. 19 Moreover, previous findings suggested that yoga may have an anxiolytic effect in healthy women 20 and women with breast cancer, 21 mental distress, 14 or restless legs syndrome. 15 Collectively, these findings suggest that regular yoga practice may be an effective strategy women can adopt to cope with stress and symptoms of depression and anxiety.
Heart rate variability (HRV) is a measure of cardiac autonomic activity. Reduced HRV indicates high sympathetic and low parasympathetic activity and has been linked to increased cardiovascular morbidity and mortality. 22 –24 Chronic stress, such as ongoing troubles and the failure to resolve negative emotional states, can generate imbalance between the sympathetic and the parasympathetic nervous system and result in reduced HRV. 25 Epidemiologic studies revealed an association between depression and autonomic dysfunction, including elevated heart rate and low HRV. 26 Davydov and his colleagues 27 indicated that compared with healthy controls, depressed patients have significantly lower HRV. A higher level of state anxiety has also been linked to decreased HRV. 28 These findings suggest a relationship between mental stress and physiologic stress.
Yoga practice has improved HRV (i.e., reduced sympathetic and increased parasympathetic nervous system activity). 29 Yoga breathing provides a unique and powerful tool for adjusting imbalances in the autonomic nervous system and thereby influencing a broad range of mental and physical disorders. 30 Studies have shown that a single session of yoga can acutely improve HRV in experienced yoga practitioners 31 and inexperienced office workers. 32 It is unclear, however, whether regular yoga training will result in positive adaptations in HRV. A study of pregnant women showed no changes in HRV after 16 weeks of yoga training. 13 In the study by Cheema et al. 28 , HRV decreased after a 10-week yoga intervention at an office worksite. Further investigation of the long-term effects of yoga on HRV is warranted.
The purpose of this study was to examine the effects of an 8-week yoga program on HRV and mood in generally healthy women. The study hypothesis was that HRV would improve and perceived stress and symptoms of depression and anxiety would decrease after the yoga intervention.
Materials and Methods
All participants were volunteers recruited through flyers and word of mouth from a university in southern Taiwan and the surrounding community. To enroll in this study, participates had to be women, aged 18–50 years, have a body–mass index less than 30 kg/m2, and not be currently engaged in regular yoga practice. Because ectopic beats would influence the analysis of HRV, 33 participants with ectopic beats during the electrocardiography (ECG) assessments were excluded from the study. Additionally, because hypertension has been associated with altered HRV, 34 blood pressure screening was performed by assessing participants' blood pressure two times separated by a 5-minute interval in a seated position. Those with hypertension (i.e., an average blood pressure ≥140/90 mmHg) or reported use of hypertension medication were excluded from the study.
To ensure that participants could safely engage in an 8-week yoga program, participants were excluded if they were pregnant or nursing or had physical contraindications to exercise (e.g., orthopedic problems or heart disease, assessed through Physical Activity Readiness Questionnaire 35 ).
The sample size of 26 participants per group was calculated with an α level of 0.05, a power of 0.80, and an effect size of 0.79. The effect size was calculated using the means (yoga and control; 8 and −4) and standard deviations (13 and 17) of the changes in high-frequency HRV (in normalized units) derived from the authors' earlier interventional study in women. G*Power software 36 was used for these calculations. The Kaohsiung Medical University Chung-Ho Memorial Hospital institutional review board approved the study protocol. All participants provided informed written consent.
All eligible participants were randomly assigned to the yoga group or the control group via a computer-generated random allocation sequence by simple randomization. The yoga group engaged in a yoga program in a group of 10–15 participants for 8 weeks. The yoga program was 60 minutes per session, which incorporated pranayama (breathing exercises), asana (postures), and savasana (meditation/relaxation). All yoga classes were offered twice per week and led by the same instructor. Participants in the control group were instructed not to engage in any yoga practice and to maintain their usual level of physical activity during the study. After completing the post-test, participants in the control group were provided a free 8-week yoga program.
All outcome measures were collected and analyzed at baseline (week 0) and after the intervention (week 9) by a qualified experimenter blinded to the group assignment.
Analysis of HRV was derived from continuous heart rate recording, at a sampling rate of 1024 Hz, using an ECG system (MP 150, BIOPAC Systems, Goleta, CA). Participants were instructed to avoid exercise 1 day before the assessment session and abstain from caffeinated food and beverages on the day of assessment. During the assessment, participants were instructed to relax in a supine position for 20 minutes while the ECG was recording. The last 10 minutes of the ECG recording was analyzed for HRV. R-R intervals were computed and the HRV power spectrum was obtained via a fast Fourier transformation algorithm using an appropriate software program (HRV Analysis for Windows; Biosignal Imaging Group and Analysis, Kuopio, Finland). The energy in the specific frequency bands of HRV was expressed as normalized units for the two frequency bands: low frequency (LF, 0.05–0.15 Hz), and high frequency (HF, 0.15–0.50 Hz). LF measures both sympathetic and parasympathetic influences, and HF measures parasympathetic influences on the heart. The LF/HF ratio is a measure of sympathovagal balance. 37
Perceived stress was measured by the 14-item Perceived Stress Scale. 38 Participants were instructed to complete the Perceived Stress Scale by indicating how often they felt or thought a certain way. The scale has a 5-point scoring system, from 0 to 4, with reverse scoring for seven positive items (items 4, 5, 6, 7, 9, 10, and 13). The final score is a sum of the scores for all 14 items. This scale has demonstrated acceptable internal consistency, with Cronbach α values ranging from 0.84 to 0.86. 38
Depressive symptoms were assessed using the Center for Epidemiological Studies Depression Scale (CES-D). 39 The scale has 20 items, and participants were instructed to rate each item on a scale from 0 (rarely or none of the time) to 3 (all of the time) on the basis of the question “How often you have felt this way during the past week?” Total score is calculated by reversing scores for items 4, 8, 12, and 16, then summing all of the scores, with higher scores indicating more severe depressive symptoms. A score of 16 or higher was identified in early studies as identifying persons with depressive illness. The CES-D has good internal consistency, with Cronbach α values of 0.85 for the general population and 0.90 for a psychiatric population. 39
Anxiety levels were assessed using the State Trait Anxiety Inventory (STAI), which includes separate measures of state anxiety (SA) and trait anxiety (TA). 40 The SA scale and the TA scale contain 20 items each, which evaluate feelings of apprehension, tension, nervousness, and worry. Both subscales use a 4-point Likert scale to allow participants to show how often or how much each question applies to them in both situations. Item scores are added to obtain a total score for each subscale. The higher score indicates greater anxiety. The STAI has demonstrated acceptable internal consistency, with Cronbach α values ranging from 0.86 to 0.95. 40
The yoga program was group-based and led by an experienced yoga instructor. Each 60-minute session consisted of 5 minutes of breathing exercises (pranayama), 5 minutes of warm-up, 40 minutes of yoga pose practice (asana), and 10 minutes of supine meditation/relaxation (savasana). Yoga props, such as blocks and belts, were used in accordance to each participant's particular body type and needs to help participants achieve precise yoga postures safely and comfortably. Examples of yoga poses practiced were Mountain Pose, Downward Facing Dog, Warrior I, Triangle pose, Tree Pose, Cat Pose, Child's Pose, and Corpse Pose. Not all poses were practiced in each session, and some more advanced poses (e.g., Warrior III, Plow Pose) were introduced later into the program as training progressed. Participants were instructed to maintain their concentration and breath control at all times during the yoga session.
This study had a two-group, pre–post design. Descriptive statistics were performed for baseline characteristics of the participants. The baseline values were checked for matching between the groups by the independent-samples t test and the chi-squared test. Intention-to-treat analysis of all participants was conducted. Missing data were imputed by carrying forward the last recorded observation. Differences between the yoga and control group were investigated using analysis of covariance of the post-test value controlling for the baseline value. Because HRV decreases with age, 41 age was added as a covariate in all analyses of covariance for HRV. The significance level (α level) was set at 0.05. All data analyses were performed with the Statistical Package for the Social Sciences, version 19 (SPSS, Inc., Chicago, IL).
Results
A total of 63 individuals volunteered for the study and 52 of them were found eligible and randomly assigned to a yoga group (n = 26) or a control group (n = 26). Six participants dropped out during the study for the reasons stated in Figure 1. There were no differences between those who dropped out of the study and those who completed the study with regard to any demographic characteristics, HRV, or psychological variables at baseline.
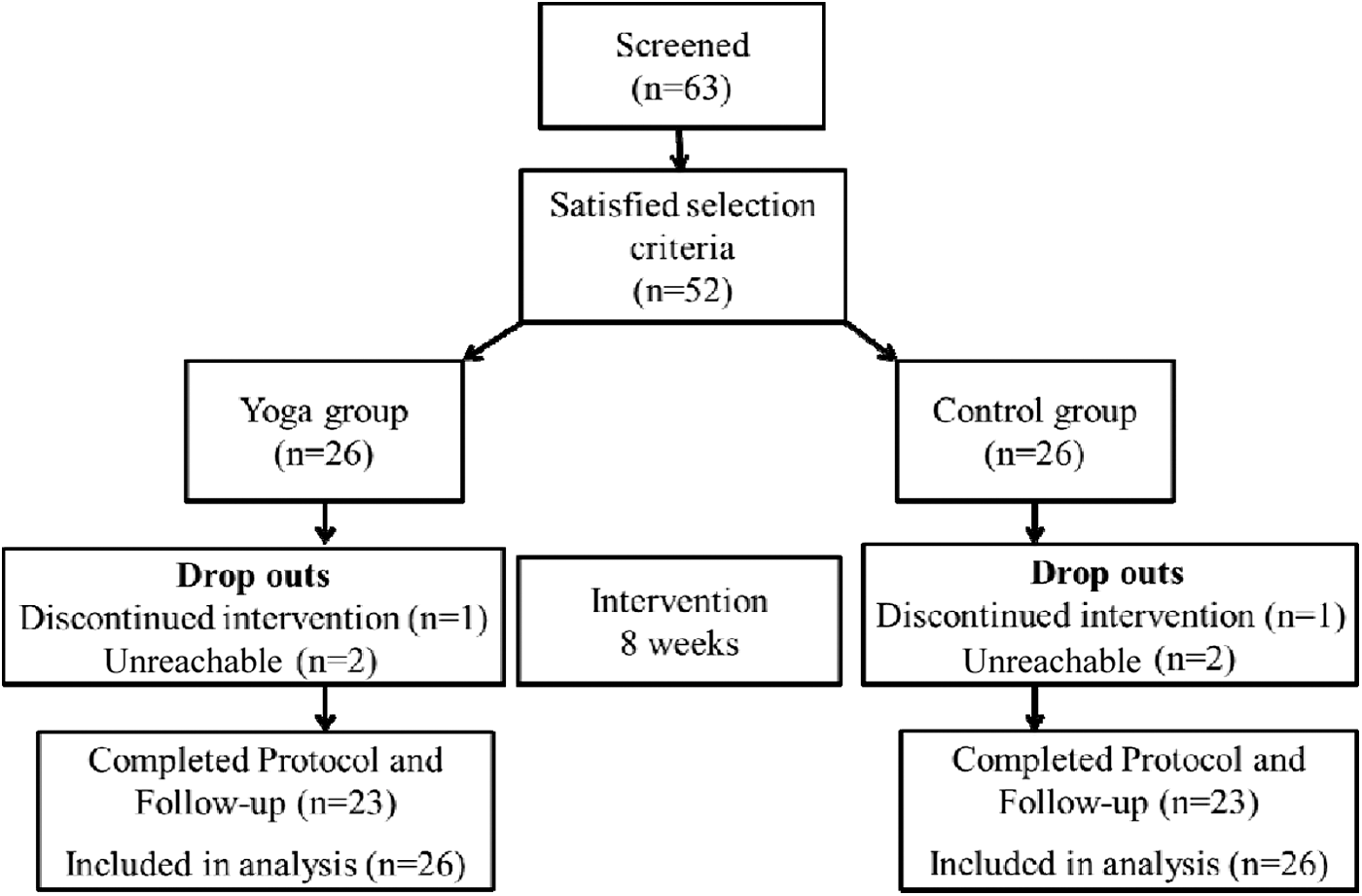
Flow of participants.
Descriptive statistics for the 52 participants are presented in Table 1. At baseline, the yoga and control groups did not significantly differ for any of the characteristics presented. Three participants were overweight (body–mass index ≥25.0 kg/m2). None of the participants were current smokers, and none had a history of tobacco use. The only two chronic conditions reported were asthma (n = 2) and mild scoliosis (n = 1). None of the participants reported engaging in regular yoga practice. For the yoga group, the average attendance rate was 83.4% (range, 62.5%–100%). No adverse events were reported in either group during the study.
Unless otherwise noted, data are presented as mean ± standard deviation.
All HRV measures are presented in Table 2. The results revealed no significant difference between the yoga and control groups in HF, LF, and LF/HF after adjustment for the baseline values and age. None of these HRV measures improved significantly in either group after the intervention.
Unless otherwise noted, data are presented as mean ± standard deviation. p and effect size (partial η2) are for between-group difference in post-baseline by analysis of covariance.
LF, low frequency; HF, high frequency; nu, normalized units; LF/HF, low- to high-frequency ratio.
All psychological measures are presented in Table 3. Yoga training had a significant effect on state anxiety after accounting for the baseline values. The yoga group had significantly reduced state anxiety after 8 weeks (p = 0.015), while the control group showed no changes. There was no significant difference between the yoga and control group in trait anxiety, depression, or perceived stress after adjustment for the baseline values. Both groups reported decreased trait anxiety, depression, and perceived stress after intervention; however, these reductions were not statistically significant.
Unless otherwise noted, data are presented as mean ± standard deviation. p and effect size (partial η2) are for between-groups difference in post-baseline by analysis of covariance.
PSS, Perceived Stress Scale; CES-D, Center for Epidemiological Studies Depression Scale.
Discussion
This study investigated the effect of yoga on HRV, stress, depression, and anxiety in women. The results suggest that an 8-week yoga program prescribed twice a week for 60 minutes per session was effective in reducing state anxiety. On the other hand, yoga practice did not significantly decrease trait anxiety, depression, or perceived stress in this population. In addition, the yoga program used in the current study was not sufficient to improve HRV. Nonetheless, the high attendance rate of yoga sessions seen in the current study suggests that yoga practice may be both feasible and acceptable for generally healthy women.
Currently, there are limited data to suggest that long-term yoga practice can result in improved HRV, that is, increased HF, decreased LF, and decreased LF/HF. Cheema et al. 28 investigated the effect of a 10-week yoga intervention in a cohort of office workers. The yoga program was three sessions per week, 50 minutes per session, and involved practice of postures, breathing exercises, and supine meditation/relaxation, similar to our yoga program. The results showed no improvement in HF and LF. Additionally, this study revealed significantly increased LF/HF in the yoga group versus the control group, different from the current findings.
Satyapriya et al. 13 examined the effect of a longer and more frequent yoga intervention in healthy pregnant women. The 16-week yoga program involved postures, breathing techniques, and meditation/relaxation techniques; it lasted 2 hours per session and was held 3 days per week during the first month. After 1 month, the participants continued to practice for 1 hour daily at home using an instruction cassette. In agreement with our findings, this study revealed no change in LF, HF, and LF/HF in the yoga or control group. However, this study showed that in the yoga group, the reduction in LF and LF/HF and increase in HF during the meditation/relaxation period were significantly greater at 16 weeks than at baseline. These findings suggest that although resting HRV remained unchanged, long-term yoga training was effective in improving HRV response during yoga practice in pregnant women. Because our study did not assess HRV during yoga sessions, it is unknown whether participants in the yoga group were more able to relax and improve HRV during yoga practice after intervention. Future studies may include HRV measures both at rest and during yoga practice to further elucidate the effect of yoga training on HRV.
Yoga training did not significantly reduce perceived stress in the current study. Previous studies have reported reductions in perceived stress after 7–16 weeks of yoga intervention in pregnant women 12,13 and women with mental distress 14 and restless legs syndrome. 15 In contrast with the results of these studies, participants in the current study were not pregnant and were generally healthy, and thus they may not perceive as much stress as women in the aforementioned studies. This may explain the small and nonsignificant changes in perceived stress found in the current study. Research involving women who experience higher levels of stress (e.g., medical professionals) may be more likely to show reduction in perceived stress after yoga intervention.
Previous studies have reported that yoga has antidepressant effects in women with depression, 16 breast cancer, 17,18 and menstrual irregularities. 19 This study, however, did not find significant changes in depression scores after 8 weeks of yoga training. The baseline values of CES-D for the yoga (11.1) and the control (13.1) groups were both lower than the cutoff score (i.e., 16) for identifying individuals with depression, 39 suggesting that our study participants were not depressed at study entry. Therefore, it may be unlikely that these participants show any further improvement in depressive symptoms after the intervention.
State anxiety was reduced significantly in the yoga group after 8 weeks' intervention. This finding provides additional evidence supporting the anxiolytic effect of yoga training in women. Michalsen and colleagues 14 found significant reductions in state and trait anxiety after a 3-month yoga program in women with mental distress. Women with breast cancer reported decreases in both state and trait anxiety after a 24-week yoga program. 21 Innes et al. 15 also indicated that state anxiety was reduced significantly after an 8-week yoga program in women with restless legs syndrome. The current finding adds to the literature suggesting that regular yoga practice is an effective strategy for generally healthy women to cope with state anxiety.
Trait anxiety, on the other hand, did not change after yoga intervention in the current study. Trait anxiety is defined as the tendency to experience anxiety, which is considered to be a characteristic of personality and may not be easily changed. 42 Studies that have shown significant reductions in trait anxiety after yoga intervention mainly involved chronically diseased 14,21 and stressed 43 populations. These studies also involved longer durations of yoga training (e.g., 10 weeks–6 months). Additional studies involving longer yoga training and enrolling individuals with high trait anxiety are warranted to further investigate the potential effect of yoga on trait anxiety.
The strengths of this study were the randomized controlled study design and the inclusion of both psychological and physiologic measures. One limitation of this study was that we recruited only women; thus, the results cannot be generalized to men. Because the majority of population who practice yoga in Taiwan are women, our findings can still be applied to those who practice yoga the most. Another limitation of this study was the low statistical power, which reduced the likelihood of the current study to detect an effect in HRV. The small sample size and the small effect size for the group differences in changes in HRV may both contribute to the low statistical power. It is thus suggested that a larger sample size may be required to provide an adequate power to detect an effect in HRV in generally healthy women. Also, since yoga sessions were performed in a group setting, it is possible that the social interaction among the yoga instructor and the study participants during yoga sessions may have had some beneficial effects. Previous studies on individuals with depression have reported a placebo effect from social interaction during intervention. 44,45 Future research on yoga may include a contact control group to control for this potential placebo effect.
In conclusion, an 8-week yoga program was not sufficient to improve HRV in generally healthy women. However, such a program appears to be effective in reducing state anxiety in this population. Future research should involve a longer period of yoga training, include HRV measures both at rest and during yoga practice, and enroll individuals with higher levels of stress and trait anxiety to further delineate the potential benefits of yoga in women.
Footnotes
Acknowledgments
This work is supported by a Kaohsiung Medical University grant (KMU-Q099012) and a Taiwan National Science Council grant (NSC100-2410-H-037-013). The authors thank the Statistical Analysis Laboratory, Department of Medical Research, Kaohsiung Medical University Hospital, Kaohsiung Medical University, for their help. Also, we would like to thank all participants for their time and effort.
Author Disclosure Statement
No competing financial interests exist.