
Abstract
Objectives:
To evaluate the effect of a single 10-minute session of Chinese head massage on the activity of the cardiac autonomic nervous system via measurement of heart rate variability (HRV).
Design:
In this pilot randomized crossover trial, each participant received both head massage and the control intervention in a randomized fashion.
Settings/Location:
The study was conducted at Children's & Women's Health Centre of British Columbia between June and November 2014.
Participants:
Ten otherwise healthy adults (6 men and 4 women) were enrolled in this study.
Interventions:
The intervention comprised 10 minutes of head massage therapy (HMT) in a seated position compared with a control intervention of sitting quietly on the same chair with eyes closed for an equal amount of time (no HMT).
Outcome measures:
The primary outcome measures were the main parameters of HRV, including total power (TP), high frequency (HF), HF as a normalized unit, pre-ejection period, and heart rate (HR).
Results:
A single short session (10 minutes) of head massage demonstrated an increase in TP continuing up to 20 minutes after massage and reaching statistical significance at 10 minutes after massage (relative change from baseline, 66% for HMT versus −6.6% for no HMT; p = 0.017). The effect on HF also peaked up to 10 minutes after massage (59.4% for HMT versus 4% for no HMT; p = 0.139). Receiving head massage also decreased HR by more than three-fold compared to the control intervention.
Conclusion:
This study shows the potential benefits of head massage by modulating the cardiac autonomic nervous system through an increase in the total variability and a shift toward higher parasympathetic nervous system activity. Randomized controlled trials with larger sample size and multiple sessions of massage are needed to substantiate these findings.
Introduction
C
However, this overall increase in awareness of the beneficial effects of massage lacks good research and valid documentation. 5,6 For this reason, this study was conducted to objectively assess the effect of head massage on the regulation of the cardiac autonomic nervous system.
Massage has been traditionally used as a therapeutic treatment in many cultures for thousands of years. Such treatment has mostly focused on localized myofascial pain, muscle spasms, or strains. Recently, however, studies have shown that massage therapy alone or in conjunction with conventional medicinal treatments has potential benefits for such indications as childhood asthma, 7 quality of life in patients with cancer, 8,9 nausea, 10 and Parkinson's disease. 11 Massage therapy has also shown some effects on reducing symptoms related to anxiety and depression. 12 These studies, however, suffer from methodological drawbacks, 5 such as small sample size, use of patient-reported outcomes that are prone to biases, or absence of control groups. 8 –11
Massage therapy is practiced in different styles and on different body parts. Head massage is a particular type of massage intervention that is popular in China and East Asia and focuses on gentle kneading and massaging different points of the head, including the scalp, forehead, orbital fissures, and cheeks. 13 Although the head and neck are highly innervated via the somatic and autonomic nervous systems, 14 no studies specifically investigating the physiologic and neurologic effect of head massage therapy on healthy volunteers were identified.
The autonomic nervous system (ANS) regulates and controls all unconscious bodily functions, including heart rate (HR); blood pressure; temperature regulation; bladder function; gastrointestinal secretion; and immune, metabolic, and endocrine responses to stressful situations, such as “fight-or-flight” situations. This system is composed of two primary components: (1) the sympathetic nervous system (SNS), also called the “catabolic nervous system,” which is in charge of fight-or-flight response, and (2) the parasympathetic nervous system (PNS), also referred to as the “anabolic nervous system,” which is in charge of digestion, elimination, and regulation of the body repair and immune system mostly during rest. 15 The SNS and PNS have constant and complex interactions with each other to keep the body functioning properly in a homeostatic state. These interactions can be analyzed by assessing cardiovascular rhythm with appropriate spectral methods. Spectral analysis of cardiovascular signal variability and in particular of the beat-to-beat (also known as R-R) period—the HR variability (HRV)—is considered a precise, noninvasive, and convenient procedure to investigate the status of the autonomic nervous system and/or target function impairment. 16
The effect of body massage on the activity of the ANS has already been investigated, with main effects of decreasing SNS activity and stimulating PNS activity. 17 –23 These studies suggest that moderate-pressure massage is the most effective with regard to enhanced relaxation and increased sympathovagal balance. 18 –20,23 Such effects are also evident with even a single session of massage. 12 The authors recently published an article reporting the effect of foot and hand massage in critically ill children, showing the increase in PNS function during one massage session (mean percentage increase in high frequency [HF], 75%; p = 0.04; n = 18), as well as a persistence in this trend of effects across several consecutive sessions separated by a period of 60–90 minutes. 24
Given the unique value of spectral analysis of cardiovascular signal variability in assessing the autonomic function, this pilot trial assessed the effect of 10-minute-long Chinese head massage therapy (HMT) on cardiac autonomic function of otherwise healthy adults using a randomized cross-over design.
Materials and Methods
Design and setting
The institutional research ethics board approved the study through the University of British Columbia, and the trial was registered at
Participants
The study involved 10 otherwise healthy adult volunteers. Exclusion criteria were a history of a disorder known to affect ANS activity or HRV, such as diabetes, hypertension, and neurologic or psychiatric disorders. Participants were also excluded if they were using antidepressants or any other drugs that could affect the activity of the ANS or HRV, smoked more than 10 cigarettes a day, or were unable to communicate or provide consent.
Procedure
After signing the informed consent, each participant was randomly assigned to one of the two interventions (described below) using computerized randomization procedure. In a crossover design, each participant was exposed to both interventions during two consecutive days at approximately the same time (between 15:00 and 16:00 hours) in order to control for the effect of the circadian rhythm on the ANS. A 24-hour gap was also considered sufficient for the washout of a possible residual effect of massage on the ANS given the transient nature of changes in HRV.
Intervention 1: HMT
A registered Traditional Chinese Medicine doctor (M.L.) performed a 10-minute-long head massage by following a Chinese HMT protocol involving gentle kneading and massaging of the scalp, forehead, orbital fissures, and cheeks while the participant remained seated on a comfortable office chair.
Intervention 2: simple relaxation or no massage (no HMT)
During this control intervention, the participant was asked to sit quietly on the same chair for 10 minutes with eyes closed.
Measurement of cardiac ANS
ANS was assessed by following a protocol for capturing and analyzing HRV. All participants were asked not to perform heavy exercise 24 hours before the assessment of their ANS. They were also asked not to drink caffeinated beverages within 3 hours of the assessment and refrain from eating a heavy meal within an hour and a half of their ANS assessment. ANS testing comprised spectral analysis of HRV and impedance cardiography (ICG) with data collected by a Biopac MP150 data acquisition system (Biopac Systems Inc., Goleta, CA) using six electrodes placed on the skin surface of the chest, neck, and lower back. Data were recorded in 5-minute segments. Signals were sampled at 500 Hz throughout all the testing. All participants were asked to sit comfortably on a chair for 5 minutes before recording of any HRV data. After the 5-minute adaptation period, baseline data were recorded for 5 minutes followed by 10 minutes of intervention 1 or 2. During the intervention period, all participants remained seated on the same chair without any HRV data being recorded. At the end of the intervention period, HRV data acquisition was immediately pursued and continued for 20 minutes in order to observe the length of the intervention effect (Fig. 1).
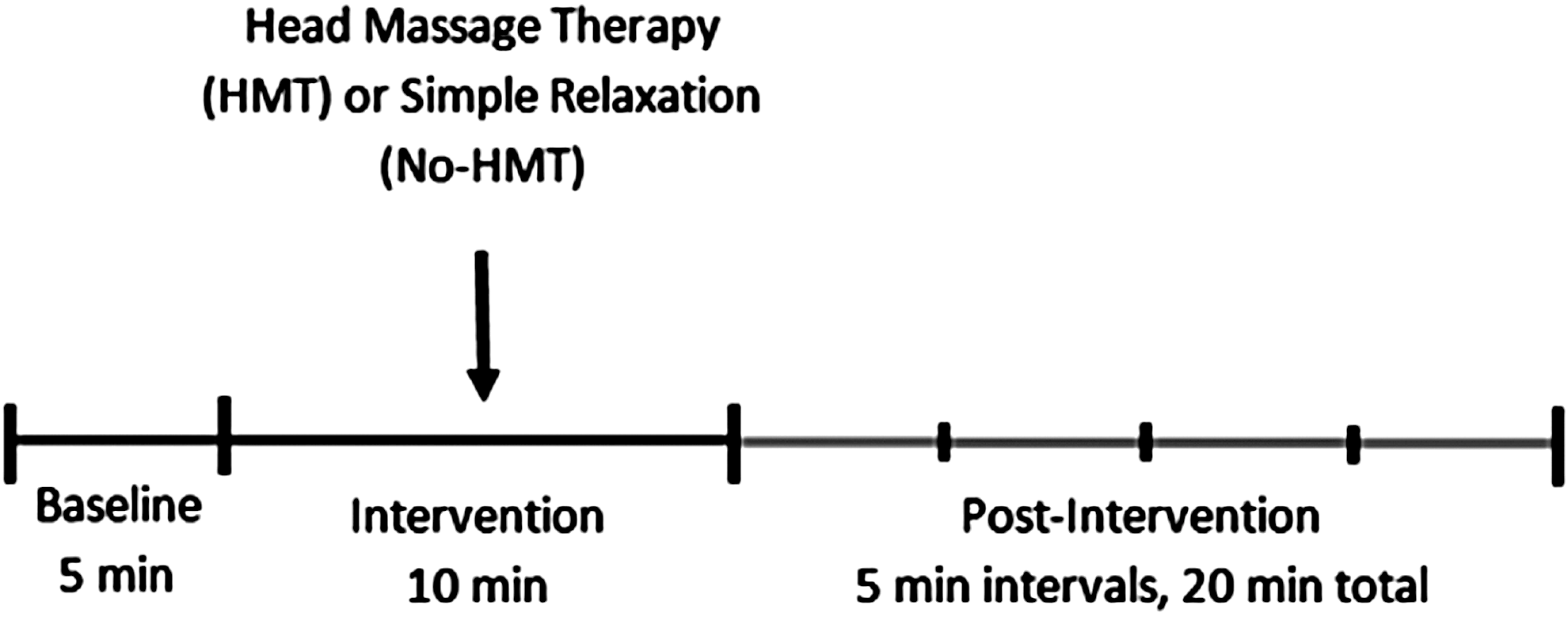
Timing of assessments for each participant. HMT, head massage therapy.
Recorded data were then reviewed manually by the HRV expert (M.S.F.) for ectopic beats and analyzed using AcqKnowledge software, version 4.2 (Biopac Systems Inc.). The fast Fourier transformation technique was used to analyze frequency domain HRV. Three frequency bands were obtained from the HRV analysis: (1) very low frequency (VLF; <0.04 Hz); (2) low frequency (LF; 0.04–0.15 Hz), which is the marker of primarily sympathetic cardiac modulation with some influence from parasympathetic modulation; and (3) HF variability (0.15–0.4 Hz), which is a marker of pure cardiac parasympathetic modulation. Total power (TP) (≤0.4 Hz), which represents the variance of all RR intervals, was also calculated by summing all frequency bands. 16
Because of questionable physiologic explanations of the VLF and LF components, 16,25 –27 only HF and TP were considered in this analysis. HF is reported both in absolute values and normalized unit (HFnu) representing the relative value of HF in proportion to the total power minus the VLF component, which can indirectly show the balance between SNS and PNS arms of the ANS. 16 Pre-ejection period (PEP) was also obtained and reported from ICG analysis; this measures the time interval from the onset of electromechanical systole to the onset of the opening of the aortic valve and is inversely correlated with the SNS influence on the heart. 28 HR, which is under the influence of both the SNS and PNS, was also obtained from ICG data analysis.
Statistical analysis
Descriptive statistics on baseline characteristics and intervention periods were used to report the results of this pilot study. Relative percentage change from baseline to postintervention period was assessed to control for the baseline differences between participants. To compare the between-interventions difference in the change from baseline to postintervention, a Wilcoxon signed-rank test was used. A p-value less than 0.05 was considered to represent a statistically significant difference. Statistical analyses were performed using SPSS software, version .22.0 (IBM, Armonk, NY).
Results
Ten healthy adult volunteers (six men and four women; mean age, 34 years) with no medical history affecting the activity of the ANS were recruited into the study. Pooled baseline values for the main variables of the study (HF, HFnu, TP, PEP, and HR) were consistent for the 2 days of intervention (Table 1).
Values are median (interquartile range). p-Values are reported using Wilcoxon rank-sum test.
HMT, head massage therapy; HF, high frequency; TP, total power; HFnu, high frequency normalized; PEP, pre-ejection period; HR, heart rate.
Comparisons of the pre- and postintervention period measures for the HRV and ICG variables are shown in Table 2 as relative percentage change from baseline rest in 5-minute segments up to 20 minutes after the intervention. Compared with simple relaxation intervention, HMT caused a significant increase in TP, peaking up to 10 minutes after the intervention and staying high up to 20 minutes after HMT (Fig. 2). The median TP relative change from baseline to 10 minutes after the intervention was 66% for HMT versus −6.6% for no HMT (p = 0.017). The activity of the PNS represented by HF was also enhanced after HMT (Fig. 3). The median HF relative change from baseline to 10 minutes after the intervention was 59.4% for HMT versus 4% for no HMT (p = 0.139).
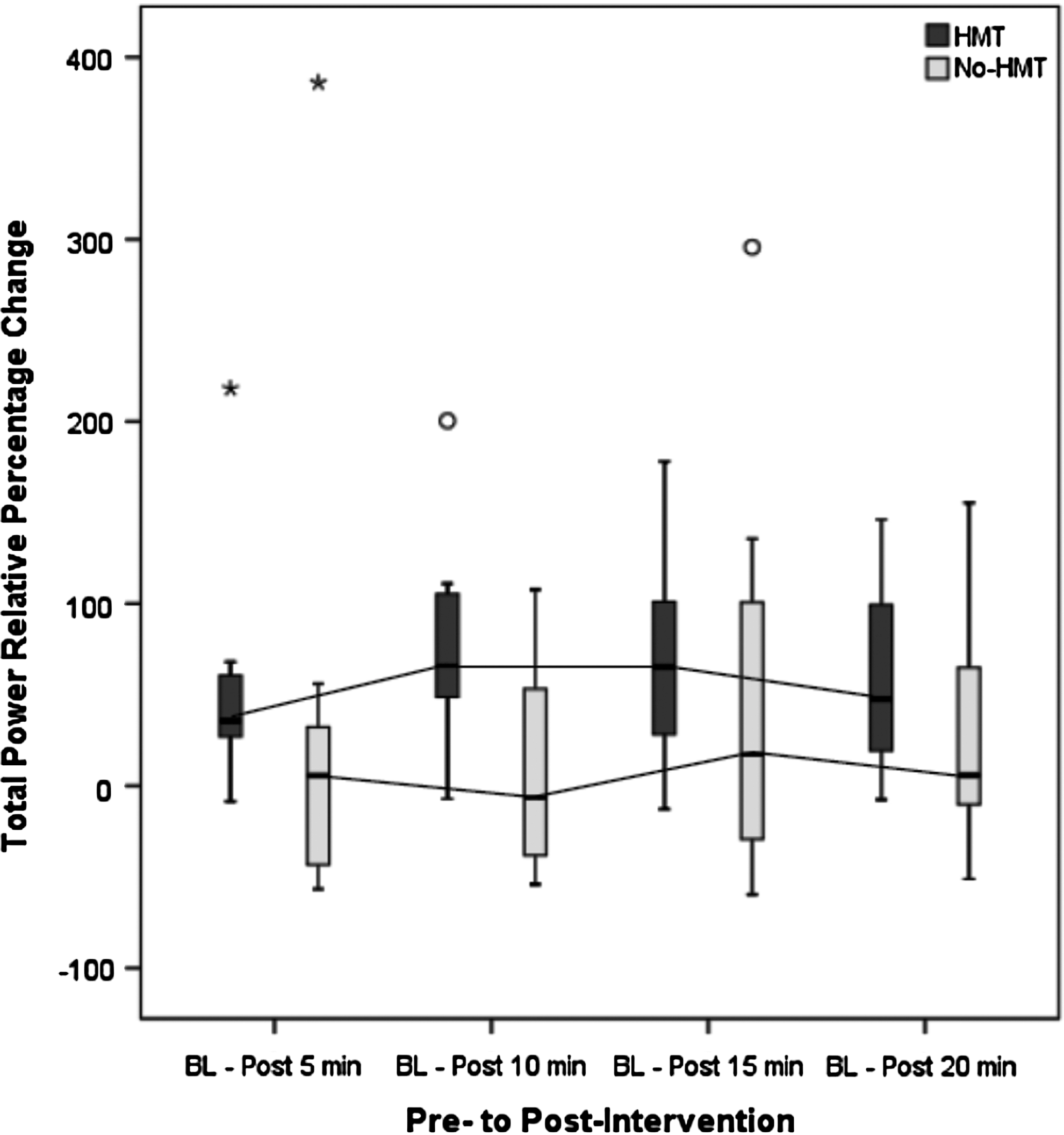
Relative percentage change in total power from baseline (BL) to 5, 10, 15, and 20 minutes after head massage therapy (HMT) and after no HMT. The boxes represent the interquartile range, whiskers indicate maximum and minimum values, open circles represent outliers (outside the inner fence but within the outer fence), and asterisks represent extreme outliers (outside the outer fence). n = 10.

Relative percentage change in high frequency (HF) from baseline to 5, 10, 15, and 20 minutes after HMT and after no HMT. The boxes represent the interquartile range, whiskers indicate maximum and minimum values, open circles represent outliers (outside the inner fence but within the outer fence), and asterisks represent extreme outliers (outside the outer fence). n = 10.
Values are median (interquartile range). p-Values are reported using Wilcoxon rank-sum test.
Participants also experienced almost three times as great a percentage decrease in their heart rate 5 minutes after receiving HMT compared with simple relaxation. The median HR relative change from baseline to 5 minutes after the intervention was −5.1% for HMT versus −1.7% for no HMT (p = 0.169). The two intervention groups also showed a difference between pre- and postintervention period measures for HFnu, which reached significance at 10 minutes after the intervention (Table 2). Median HFnu relative change from baseline to 10 minutes after the intervention was −5.1% for HMT versus 9.4% for no HMT (p = 0.022).
PEP also slightly changed for both interventions; however, the change was minimal and nonsignificant. The direction of the change was a slight increase in PEP for both interventions, with massage showing a higher change (Table 2). The median PEP relative change from baseline to 10 minutes after the intervention was 0.63% for HMT versus 0.36% for no HMT (p = 0.646).
Discussion
This pilot randomized crossover trial is the first study that objectively evaluates the effect of a single session of HMT on the modulation of the cardiac ANS, using each participant as his or her own control and followed up to 20 minutes after the intervention. The results provide valuable information suggesting that a single 10-minute session of HMT can effectively increase total variability within the cardiac ANS up to 20 minutes after HMT while reaching statistical significance at 10 minutes after the massage. The finding of increased HF extending up to 10 minutes after HMT was also somewhat in line with previous studies showing that massage may have a more prominent effect on the PNS component of the ANS. 19,20,23
The current results of our study also showed a minimal change in PEP values for both interventions. This can be interpreted as massage not having a significant effect at the level of cardiac SNS system. This may be due to the relatively higher presence of the PNS fibers innervating the head and neck surface area compared with the SNS fibers.
A few studies have investigated the effect of massage therapy on the activity of the ANS; however, these studies suffer from important methodological limitations, such as lack of proper control groups, confounding by other stress factors, not adjusting for the time of the day, and not specifying the body area being treated or the specific massage technique being administered. They also had substantial variability in the specific ANS profile report, such as assessing the ANS through non-HRV–measuring procedures 29 or reporting debatable or incomplete HRV variables. 18 –20 Furthermore, on the basis of the literature search performed before the current study, no study has assessed the effect of head massage on ANS function.
Diego and Field 19 have already shown in a pilot randomized trial on 20 healthy adults that the amount of massage pressure has different effects on the ANS: “Light” massage stimulates the SNS, while “moderate” pressure massage stimulates the PNS (as measured by HF raw values). 19 The authors also interpreted the reduction in the LF-to-HF ratio during massage as a sign of “shift” from SNS to PNS activity during massage. However, this assumption is not well established because the LF component of the HRV comprises a complex mixture of SNS (as a dominant factor), PNS, and other unidentified factors and provides a poor index of cardiac sympathetic regulation. 16,25 –27
The current study reports both HF raw values and normalized HF values (HFnu) to get a better sense of the PNS activity alone and in relation to TP for the sake of better understanding the balance between the arms. HFnu has been suggested and reported previously;
16
however, the research on this variable is not solid. The current study found a statistically significant change in HFnu in an unexpected direction (median HFnu relative change from baseline to 10 minutes after intervention was −5.1% for HMT versus 9.4% for no HMT; p = 0.022). To understand this counterintuitive result, the formula from which the value of HFnu is calculated needs to be addressed
One area of strength in this study is the comparison of the participants with themselves in a randomized crossover design conducted over 2 consecutive days at approximately the same time of the day to control for the effect of the circadian rhythm on the ANS. The HMT intervention was also administered by a TCM doctor with considerable expertise.
The study does, however, have some weaknesses: Because of the position of some of the electrodes on the neck area, their proximity to the hands of the massage therapist, and the resultant artifacts created in the HRV/ICG data, it was not feasible to record the HRV during massage. In addition, the sample size for this study is small (n = 10), which affects the power. However, the effect of HMT was prominent enough that the study could find a significant increase in the total variability of the cardiac ANS, which peaked up to 10 minutes after massage. Other parameters, such as HR and HF, also showed an important change; however, these did not reach statistical significance at α = 0.05 because of low power.
This pilot study is important in the context of the increased demand for therapeutic massage, which is becoming more acceptable and appreciated by both public as well as other healthcare professionals. 4 Head massage also has the advantage of possibly being self-administered, 13 thus leading to the possibility of keeping the same trend (higher total variability, higher PNS activity, and decreased HR) by repeating massage sessions during the day.
Nevertheless, future studies are required with larger sample sizes and more objective assessment of the outcomes investigating multiple sessions of massage (including self-massage procedure) in the context of disorders that affect the activity of the ANS, as well as evaluation of cost-effectiveness of this treatment compared with conventional medical treatment options.
In conclusion, the results of this pilot randomized crossover trial in 10 healthy adults suggest that a single 10-minute session of HMT compared with a control intervention of simple relaxation in a controlled laboratory environment has the ability to significantly increase the total variability of the cardiac ANS by more than 60-fold up to 20 minutes after massage while shifting the autonomic balance toward higher activity of the PNS.
Footnotes
Acknowledgments
The authors would like to thank Mojgan Gitimoghaddam for her help in preparing the ethics application for this study. The authors also thank all participants of this study for their time and cooperation.
Author Disclosure Statement
No competing financial interests exist.