
Abstract
Objectives:
Clinical aromatherapy is a complementary therapy that may be very helpful for elderly dementia care. Aromatherapy may reduce the behavioral and psychological symptoms of dementia (BPSD), improve quality of care, and thus improve the quality of life for people with dementia. In this pilot study, aroma hand massage therapy was used for elderly patients in a medical institution in Japan. The study assessed the effectiveness and safety of clinical aromatherapy as part of routine integrative care among people with dementia in a clinical care setting.
Interventions:
The randomized, crossover pilot trials were performed among 14 patients with mild-to-moderate dementia older than age 65 years living in a nursing home in Nara, Japan. Participants were divided into two groups and offered, alternately, control therapy and clinical aromatherapy 3 times a week for the 4-week trials. The effects on BPSD and activities of daily living (ADLs) were evaluated quantitatively before and after the study and 4 weeks after the study ended as a follow-up. Observation records were also collected to obtain qualitative data.
Results:
The quantitative data showed that neither therapy significantly improved the BPSD or ADL results. The qualitative data were classified into four main categories—mood, behavior, verbal communication, and nonverbal communication—reflecting the positive experiences of participants during both therapies. No harmful reactions or changes in medication occurred during the study.
Conclusions:
This pilot study demonstrated that clinical aromatherapy was clinically safe but did not lead to statistically significant improvements in BPSD or ADL among people with dementia. Further research on therapeutic effects is needed to develop high-quality care with clinical aromatherapy for elderly patients with dementia in Japan and to fully establish evidence for effective and safe practice in health care institutions.
Introduction
T
For the treatment of people with dementia, pharmacologic interventions: antidepressants, antipsychotics, anxiolytics, and hypnotics along with antidementia drugs are used to treat BPSD. 4 However, the limitations of pharmacologic interventions for achieving a positive clinical effect and their adverse effects are increasingly being discussed. People with dementia have physiologic changes and are vulnerable to adverse effects. In recent years, nonpharmacologic and psychosocial interventions have been of increasing concern in the management of BPSD. These interventions have been recommended in general dementia guidelines, without prior agreements about specific practices, as first-line treatment in combination with careful use of antipsychotics for BPSD. 5
Still, psychosocial interventions included in nonpharmacologic intervention have also been recommended for the treatment of people with dementia not only to improve cognitive abilities, enhance emotional well-being, reduce behavioral symptoms, and promote everyday functioning but also to reinforce and augment pharmacologic treatments and complement support from family caregivers. Evidence to support psychosocial interventions is urgently need to ensure they are both safe and effective. 6,7
As a nonpharmacologic and psychosocial intervention, aromatherapy was reported as a possibly effective dementia treatment. This complementary, alternative, and integrative medicine offers person-centered, individual treatment with a holistic view of wellness and well-being in life. 8,9 Aromatherapy is used clinically with essential oils from plants for hypertension, depression, anxiety, pain relief, and dementia. 10 For dementia treatment, aromatherapy acts on cognitive performance, attention, and mood via olfactory stimulation with essential oils and has benefits for dementia-related mood and behavior disorders. 11 Aromatherapy and massage as multisensory stimulation treatments are also recommended by the United Kingdom's National Institute for Health and Care Excellence for dementia with BPSD. 12
Although the positive effects of aromatherapy for the treatment of dementia have been reported, recent reviews showed only equivocal benefits in the clinical effectiveness of aromatherapy for people with dementia. For agitation and the behavioral symptoms of BPSD, one systematic review concluded that aromatherapy did not reduce agitation when assessors were blinded to the intervention. 13 –15 This report of randomized controlled trials of aromatherapy in long-term care facilities demonstrated that (1) aromatherapy with external application of essential oil Melissa officinalis was safe and effective for clinically significant agitation with severe dementia in a nonblinded study and (2) there was no immediate or long-term improvement relative to the control group among participants with severe agitation in a high-quality blinded study, and this study showed no evidence that Melissa aromatherapy was superior to placebo or donepezil. 13 –15 Another review also reported the equivocal aromatherapy benefits for agitation and behavioral symptoms of BPSD, adverse effects, quality of life (QOL), and activities of daily living (ADLs) in dementia. 16 In terms of adverse effects, Burns et al. 15 and Fu et al. 17 found no significant difference between aromatherapy and placebo. Thus, the evidence indicating adverse effects from aromatherapy for dementia appears low. 15,17
Other small studies of the effectiveness of aromatherapy among people with dementia reported the benefits of reducing insomnia and anxiety and improving cognitive function through inhalation. 18,19 The combination of aromatherapy and massage showed the greatest reduction in behavioral disturbance in dementia compared with conversation and aromatherapy and massage only. 20 However, these studies have methodologic limitations due to not only small samples size and flaws in the randomized controlled trial design but also in the differences in choice and blending of essential oils, their application, the frequency of intervention, the intervention period, and follow-up practice. Each of these variables may have affected research results so far.
Thus, aromatherapy, as a nonpharmacologic and psychosocial intervention for dementia with BPSD, does not generate consistent evidence for effectiveness and safety among people with dementia. However, it may still be a therapeutic, safe complementary treatment for dementia with BPSD.
In this pilot study, aroma hand massage therapy was begun among elderly patients in a medical institution in Japan. The study administered clinical aromatherapy with the synergistic sensory stimulation of essential oils and hand massage as routine care in a clinical care setting. The randomized crossover trials monitored the efficacy of clinical aromatherapy in integrative care among people with dementia and measured (1) the effectiveness of aromatherapy for BPSD and ADLs, (2) the safety of aromatherapy as routine care in a clinical care setting, and (3) the qualitative effect with regard to quality of care. This pilot study of clinical aromatherapy was expected to contribute to the development of high-quality care for the elderly in the aging society of Japan.
Materials and Methods
Participants
Study participants were recruited from a nursing home in Nara, Japan, in July 2014. Participants were enrolled according to the following inclusion criteria: (1) residence in the nursing home, (2) age 65 years or older with dementia diagnosed by the International Classification of Diseases, 10th revision, 21 (3) mild-to-moderate dementia (score of 10–26 on the Mini-Mental State Examination [MMSE]), 22,23 (4) score of III on the Independence Degree of Daily Living for the Demented Elderly scale, 24 (5) negative reaction on a patch test with jojoba oil and Delight & Harmony oil (D&H oil; Aromatica Wellness, Turku, Finland), and (6) consent for participation from patients and their families. Exclusion criteria were any acute physical illness. Types of dementia were distinguished. After the facility manager granted permission to recruit patients, residents who might meet the inclusion criteria were identified. Permissions was received for a total of 14 residents and their families according to the informed consent form. Participant demographic characteristics relevant to this study were obtained from resident records with the permission of the participants, their families, and the facility manager. This study was approved by Tenri Health Care University Human Research Ethics Committee and the management of the facility.
Materials
This study compared results of control therapy with jojoba oil with those of clinical aromatherapy with D&H oil administered by the same method. It was massaged gently on one hand and then the other in the following order: forearm, wrist, palm, fingers, and back of the hand. D&H oil is made from pure organic vegetable oils and essential oils and is used as a massage oil for aromatherapy. It contains the following essential oils: Citrus aurantium leaf, Cymbopogon martini, Picea mariana, Lavandula angustifolia, Rosa damascena, Citrus paradisi, and M. officinalis. Table 1 shows the analysis of the main chemical components of D&H oil obtained by gas chromatography–mass spectrometry at the Faculty of Pharmacy, Division of Pharmaceutical Biosciences, University of Helsinki, Finland. The diluted ratio of essential oils in D&H oil is about 1% less than that of general massage oils for aromatherapy (2%–3%). No adverse effects of the oil have ever been reported during the combination of massage and medication. Jojoba oil was used as a control. 25
Reproduced with permission: Copyright ©Aromatica-Wellness Finland 2014.
Study design
This pilot study was conducted as foreground to a full-scale study. In the single-blind crossover trials, participants were randomly assigned to the following two groups: (1) hand massage therapy that began with clinical aromatherapy and then switched to control therapy and (2) hand massage therapy that started with control therapy and then switched to clinical aromatherapy. In both the first and second trials both therapies were administered 3 times per week for a total of 4 weeks, with a 4-week washout interval. A single researcher and aroma therapist administered each therapy with a total of 3 mL per both hands for 10 minutes in the living room of the facility in the afternoon. The therapies were withheld when participants had infections, external injuries, or acute physical illness or when they declined treatment. Medications and other therapies for participants continued during the trials. Before and after the trials and 4 weeks after the study as a follow-up, a single researcher evaluated the effect on BPSD and also ADLs. The therapist collected observation records before and after each therapy session during the trials.
Measures
BPSD, especially in depression and agitation, and ADLs were measured by a single researcher with sufficient training. This researcher strictly followed the measures' criteria to ensure objectivity and reliability. The researcher assessed three measures of BPSD with dementia: (1) the Cornell Scale for Depression in Dementia (CSDD) for depression symptoms, a reliable and valid instrument; 26,27 (2) the Cohen-Mansfield Agitation Inventory (CMAI), a validated instrument to assess the frequency of agitated behavioral disturbance; 28 –32 and (3) the Neuropsychiatric Inventory–Brief Questionnaire Form (NPI-Q), a reliable and valid instrument for assessing the degree of psychiatric symptoms and care burdens. 33,34 ADLs were scaled by using the Functional Independent Measure (FIM), which measures the degree of disabilities and assistance required in ADLs with excellent reliability and validity. 35 –37 The MMSE is a good validated measurement to assess cognitive function. 22,23 The Independence Degree of Daily Living for the Demented Elderly, commonly used in the Long-term Care Insurance System in Japan, measures the independence and care support level of daily living for people with dementia. Levels less than III exclude patients with mild dementia, who are almost independent or mainly need home care support. 24 These last two measurements were used to enroll suitable participants. Observation records, including visual and verbal expressions of individual participants, were recorded by the therapist before and after each massage therapy in order to obtain qualitative data.
Analysis
The sample size was calculated for a null hypothesis with a type I error rate of 0.05. To analyze the improvement in BPSD before versus after the trials and before versus 4 weeks after the study, each participant's CSDD, CMAI, NPI-Q, and FIM data were individually analyzed by sign test (binominal exact test), which is a paired and nonparametric test suitable for small numbers of participants (<25). This was used to compare both therapies directly. The changes in CSDD and CMAI scores after the trials and 4 weeks after the trials (follow-up) in each participant were also analyzed by Friedman chi-square test as a nonparametric test for repeated measures. The results of the analysis are presented by p-values. For the qualitative data, another researcher inductively classified the description of each participant's expressions into four main categories—mood, behavior, verbal communication, and nonverbal communication—to specify the importance of the positive experiences in aromatherapy care for individual participants.
Results
Sixteen residents were recruited from the medical facility. Residents and their families granted permission for the assessment of eligibility. After exclusion of 2 participants not meeting the inclusion criteria, 14 participants were randomly assigned. All but 2 participants completed both trials. Figure 1 shows the flow chart of participants' progress through the randomized crossover trials. Table 2 shows participant characteristics. All were elderly women (mean age ± standard deviation, 82.8 ± 9.503 years). Participants were diagnosed with the following dementia subtypes: Alzheimer's dementia (n = 5 [42%]), vascular dementia (n = 3 [25%]), fronto-temporal dementia (n = 1 [8%]), and other (n = 3 [25%]). Ten participants (83%) showed moderate cognitive impairment according to MMSE score; the other 2 (17%) had mild cognitive impairment. Some participants had already taken the following medication for BPSD: hypnotics (33%), antipsychotics (25%), antidepressants (8%), and/or mood stabilizers (17%). In addition, each participant had taken medications for physical complications, such as hypotensive, antidiabetic, and antihyperlipidemic agents.

The flowchart of the participants' process through the randomized crossover trials.
MMSE, Mini-Mental State Examination.
Table 3 shows the analysis of the improvements in BPSD and ADLs with both therapies before versus after the trials and before versus 4 weeks after study end, with direct comparison of each participant's data. The symptoms related to depression improved (CSDD score), but not statistically significantly, after the trials (versus before; p = 0.0625). Agitated behavior consisting of complaining and repetitious mannerisms, measured by CMAI, changed but did not show statistical significance. BPSD, measured by NPI-Q, and ADL, measured by FIM, also did not significantly improve with either therapy. In addition, scores on CSDD, CMAI, NPI-Q, and FIM before and after the trials and 4 weeks after the study (follow-up) did not significantly change for either therapy. Figure 2 shows the changes in CSDD score for both therapies.
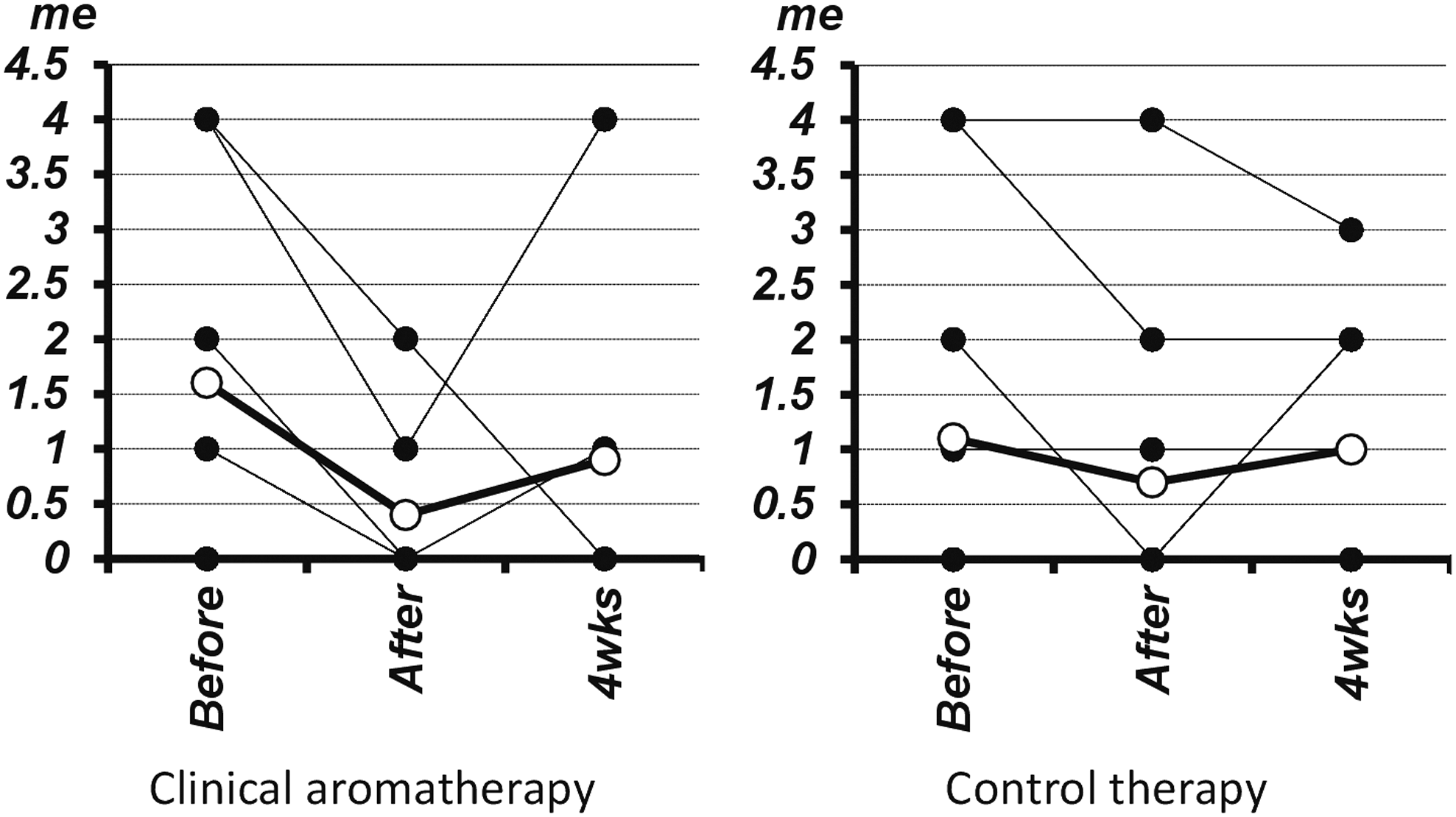
Changes in Cornell Scale for Depression in Dementia (CSDD) score associated with clinical aromatherapy and control therapy. Friedman chi-square test: two-tailed (clinical aromatherapy p = 0.1612, control therapy p = 0.7985). ●, score point; ○, mean score point; me, mean.
CSDD, Cornell Scale for Depression in Dementia; CMAI, Cohen-Mansfield Agitation Inventory; NPI-Q, Neuropsychiatric Inventory–Brief Questionnaire Form; FIM, Functional Independent Measure.
For qualitative data, Table 4 shows the positive experiences of participants during or after each therapy. With neither therapy did participants' expressions differ, except for smelling the scent on the hands and the expressed feelings of comfort by two participants receiving clinical aromatherapy. A participant occasionally talked about feelings of persecution and hallucination but was not visibly disturbed during massage. Occasionally a participant declined both therapies, with no complaint about the therapies.
Neither oil caused dermatologic or other possible adverse effects. In addition, no harmful reactions, no deteriorating clinical symptoms, and no changes of medication occurred with either therapy performed 3 times per week for a total 4 weeks in the trials.
Discussion
There was no statistically significant improvement in clinical effects on BPSD measured by CSDD, CMAI, and NPI-Q or in ADLs measured by FIM for either therapy performed 3 times per week for a total of 4 weeks. No review has included the data on effect of mood in dementia by aromatherapy, 14 but this study demonstrated that symptoms related to depression (CSDD) improved during the trials (p = 0.0625) using clinical aromatherapy. The duration of each trial for both therapies was only 4 weeks, which may not have been long enough to gain more effectiveness with regard to BPSD and ADLs. The effects of the massage method and D&H oil themselves were not compared with different methods and applications. To provide more rigorous research into clinical aromatherapy, both methods and implementation could be considered more carefully.
This study used 10-minute sessions held 3 times per week during the daily activity of the nursing home, and it was not difficult to administer each therapy. During each 4-week trial, a participant occasionally declined both therapies without any complaint about the therapy itself. This patient was easily tired and declined because of her usual drowsiness and resistance against “being cared for.” People with dementia are highly sensitive to sensory experiences and care environments. Clinical aromatherapy needs to be managed carefully, and care experiences, personal relationships, and attitudes toward “being cared for” must be considered in order to provide acceptably administered, person-centered, individual, and collaborative care for people with dementia. To practice ethical and routine clinical care in health care institutions, further research on the frequency and duration of clinical aromatherapy is also needed.
In terms of quality of care, the positive experiences of care by participants were similar with both therapies through interaction with the therapist; however, clinical aromatherapy affected mood by creating a “comfortable” feeling via olfactory stimulation from the D&H oil blending with essential oils. These experiences of mood, behavior, and communication with both therapies cannot be generalized because of individual experiences, but they may reflect a high quality of care that generates (1) positive emotions; (2) a person-centered environment with an atmosphere of respect for individuals; and (3) communication and feedback in line with satisfaction, confidence, and positive social relationships. In 2012, Lawrence observed that psychosocial intervention had a benefit for people with dementia in connecting with others, making a social contribution, and reminiscing. 38 There is no consensus on QOL measures for people with dementia, 39 but domains of QOL (including the ability to engage in social behavior and create a favorable balance between positive emotion and absence of negative emotion) may well be measurable in future interventions for people with dementia. 40 For clinical aromatherapy as a psychosocial intervention for people with dementia, further qualitative research with stronger analytic methods and with reliability and validity is also needed to show clinical aromatherapy contributes to high-quality care, can help develop quality of care, and can improve a person's QOL during the treatment of dementia.
With respect to safety, the two aromatherapy oils for this study and the massage method in both therapies demonstrated no dermatologic effects, harmful reactions, worsening of clinical symptoms related to BPSD, or effect on medication. Clinical aromatherapy used D&H oil with a total of 1.02% essential oils and 0.2% lavender oil. A recent review of aromatherapy reported the potential cause of adverse effects, including dermatitis, from use of the most common essential oils: lavender, peppermint, tea tree, and ylang-ylang oil. 41 Because careful assessments are needed to evaluate both physiologic and psychological causes of dementia symptoms before any treatment is applied, 42 the appropriate dosage and concentration of blending oils with essential oils in clinical aromatherapy must be addressed, especially for the elderly, who have more fragile bodies and are often receiving multiple medications.
This pilot study had some limitations. The findings were based only on a small sample size of elderly female participants. The lack of inclusion of both men and women with dementia makes distinctions between specific types of dementia difficult. In addition, influence by the researchers of single-blind crossover trials should be acknowledged. The analysis of qualitative data did not contain the entire process of content analysis or the requisite reliability and validity. Therefore, further research, full-scaled and better designed, is needed to identify the therapeutic effectiveness and safety of clinical aromatherapy considering the methodologic and ethical matters discussed above.
In conclusion, this pilot study demonstrates that clinical aromatherapy is clinically safe but does not provide statistically significant effectiveness for BPSD and ADLs among patients with dementia. Further research on therapeutic effects is needed to develop high-quality care with clinical aromatherapy for elderly patients with dementia in Japan and to fully establish evidence for effective and safe practice in health care institutions.
Footnotes
Acknowledgments
The authors thank the participants, family members, and nursing staff at Seijuen elderly care home in Nara, Japan, for their support. They also thank the Association of Integrative Medicine for Mental Health Care for supporting clinical aromatherapy and Aromatica Wellness for supplying the certified organic massage oil (Delight & Harmony oil).
Author Disclosure Statement
No competing financial interests exist.