
Abstract
Objectives:
Postoperative ileus (POI) is a common problem after abdominal surgery. Acupuncture is being accepted as an option for reducing POI and managing various functional gastrointestinal disorders. Therefore, this pilot study was conducted to evaluate the effect of acupuncture on reducing duration of POI and other surgical outcomes in patients who underwent gastric surgery.
Design:
A prospective, randomized, controlled pilot study was conducted on patients who underwent gastric cancer surgery from January 2013 to December 2013. Ten patients were randomly assigned into the acupuncture (A) or nonacupuncture (NA) groups at a 1:1 ratio.
Interventions:
The acupuncture treatment was performed by Korean traditional medicine doctors (KMDs). The style of acupuncture was Korean. In the A group, acupuncture treatment was given once daily for 5 consecutive days starting on postoperative day 1. Each patient received acupuncture at 16 acupoints based on expert consensus provided by qualified and experienced KMDs. No acupuncture treatment was performed in the NA group.
Outcome measures:
The primary outcome measure was the number of remnant Sitz markers in the small intestine on abdominal radiography. Secondary outcome measures were time to first flatus, start of sips water, start of soft diet, hospital stay, and laboratory findings.
Results:
The A group had significantly fewer remnant Sitz markers in the small intestine on postoperative days 3 and 5 compared with those in the NA group (p = 0.025 and 0.005). A significant difference was observed in the numbers of remnant Sitz marker in the small intestine with respect to time difference by group (p = 0.019). The A group showed relatively better surgical outcomes, but without statistical significance.
Conclusions:
Although further studies are warranted, acupuncture may reduce duration of POI after gastric surgery and could be a potential factor in enhanced recovery after surgery protocols.
Introduction
I
The precise mechanism and cause of POI are not completely understood. It seems that altered contractile activity of the small bowel due to interactions between the enteric nervous system, central nervous system, hormones, and local molecular and cellular inflammatory activity is an important mechanism for POI. 2 Patients have diffuse discomfort but no sharp colicky pain or distended abdomen. Stasis and progressive accumulation of gastric and intestinal secretions and gas result in abdominal distention, pain, nausea, vomiting, and obstipation.
Successful management for reducing duration of POI is challenging. Although chewing gum, epidural local anesthetics, prokinetic agents, and opioid antagonists have been used to shorten the time to recovery of intestinal function, 3,4 the duration of POI is still reported to be as long as 4 days. 5
Additional treatment modalities are needed to reduce duration of POI because prompt recovery of bowel function after surgery is important not only for the well-being of patients but also for healthcare costs. In addition, prolonged ileus can lead to other complications that prolong hospital stay. It is estimated that reducing the mean length of hospital stay by only 1 day may reduce the annual healthcare system costs in the United States by approximately $1 billion. 6
Acupuncture is a minimally invasive integrative oncologic modality with a very low incidence of side effects. 7 It has been used in China for thousands of years to treat a variety of gastrointestinal (GI) problems 8 and has recently been used as a treatment option for reducing POI and various functional gastrointestinal disorders. 5,9,10 Although the role of acupuncture in reducing duration of POI is less clear, several studies have shown accelerated motility and promoted contractility of the bowel via parasympathetic and cholinergic pathways after acupuncture treatment. 11,12
The current prospective randomized pilot study was conducted to evaluate the efficacy of acupuncture on reducing duration of POI and other surgical outcomes in patients who underwent gastric cancer surgery for a later large-scale study.
Materials and Methods
Study design
This prospective, randomized, controlled pilot study was performed among patients who underwent surgery for histologically proven gastric carcinoma at the Department of Surgery of Daegu Catholic University Medical Center, Korea, from January 2013 to December 2013. Participants were recruited from inpatients who were awaiting scheduled surgery for gastric cancer. Inclusion criteria were gastrectomy for gastric cancer, age older than 18 years, American Society of Anesthesiologists grade I–III, 13 and written informed consent. Excluded were patients who received epidural anesthesia or analgesia, those who had contraindication for electrical stimulation devices (pacemaker or implantable defibrillator), those who were allergic to acupuncture needles, and those who had a history of major abdominal or pelvic surgery. Patients who enrolled in the study were informed by the principal investigator about the study details before their scheduled surgery. Ten patients were randomly assigned to the acupuncture (A) group or the nonacupuncture (NA) group before surgery (1:1 ratio) by a medical statistician who was not a study investigator. Because of the study was a pilot study, the sample size was not calculated.
Patients in both groups followed the same standard preoperative protocol, including bowel preparation, antibiotic prophylaxis, and preoperative fasting period. Both groups also received same postoperative management. Early ambulation was encouraged, and oral feeding was resumed as early as possible. Patients were discharged when they tolerated a solid diet and were fully ambulatory.
This study was approved by the Clinical Research Ethics Committee of Daegu Catholic University Medical Center (DCMC-CR-13-011), and informed consent was obtained from all patients
Acupuncture interventions
The acupuncture treatments took place in the East-West Medical Center of Daegu Catholic University Medical Center and were performed by Korean traditional medicine doctors (KMD) who had at least 3 years of clinical experience in acupuncture. The style of acupuncture was Korean. In the A group, the acupuncture treatment was given once daily for 5 consecutive days starting on postoperative day 1. Each session lasted 25–30 minutes, starting from the moment the first needle was inserted. Single-use, sterile, disposable acupuncture needles (stainless steel, 0.20 mm in diameter and 40 mm in length) were used. The selection of acupoints for this study was based on expert consensus provided by qualified and experienced KMDs and other studies. 5,11,12 During each acupuncture session, each patient received 16 acupuncture needles at bilateral ST 36 (Zusanli), SP 6 (Sanyinjiao), LI 4 (Hegu), TE 6 (Ziagou), LV 3 (Taichong), LI 11 (Quchi), and unilaterally at GV 20 (Baihui), EX HN3 (Yintang), GV 26 (Shuigou), and CV 24 (Chengjiang). The depth of acupoints located in extremities such as ST 36, SP 6, LI 4, TE 6, LV 3, and LI 11 was 20 mm, and acupuncture needles were inserted perpendicular to the skin. Acupoints located in the head, such as GV 20, EX HN3, GV 26, and CV 24, were incapable of 20-mm depth; therefore, we inserted acupuncture needles to a 5-mm depth with 30° angled to the skin. Electrical stimulation (ES-160, Ito Co., Ltd, Tokyo, Japan) of 100-Hz frequency was applied at bilateral ST 36, SP 6, LI 4, and TE 6. No acupuncture treatment was performed in the NA group, and the same postoperative management was applied in both groups.
Outcome evaluation
To evaluate postoperative recovery of small bowel movement, Sitz marker count was used. The Sitz marker is composed of 20 radio-opaque spherical plastic markers (diameter of 4 mm) inside one capsule, which has been widely used for evaluation of gastrointestinal transit time. 14,15 A Sitz marker capsule was inserted into the duodenum of patients who underwent distal gastrectomy, and the capsule was inserted into the jejunum side of the esophago-jejunal anastomosis in patients who underwent total gastrectomy. Abdominal radiographs were obtained for all of patients at postoperative day 1, 3, 5, and 7. The primary endpoint was the number of remnant Sitz markers in the small intestine that did not pass through ileocecal (IC) valve measured by radiography. The remnant Sitz markers were counted by one specialized radiologist to reduce bias. The radiologist was blinded so that he did not know whether the radiograph was from the A or NA group. Figure 1 shows representative abdominal radiographs of patients in the A and NA groups.
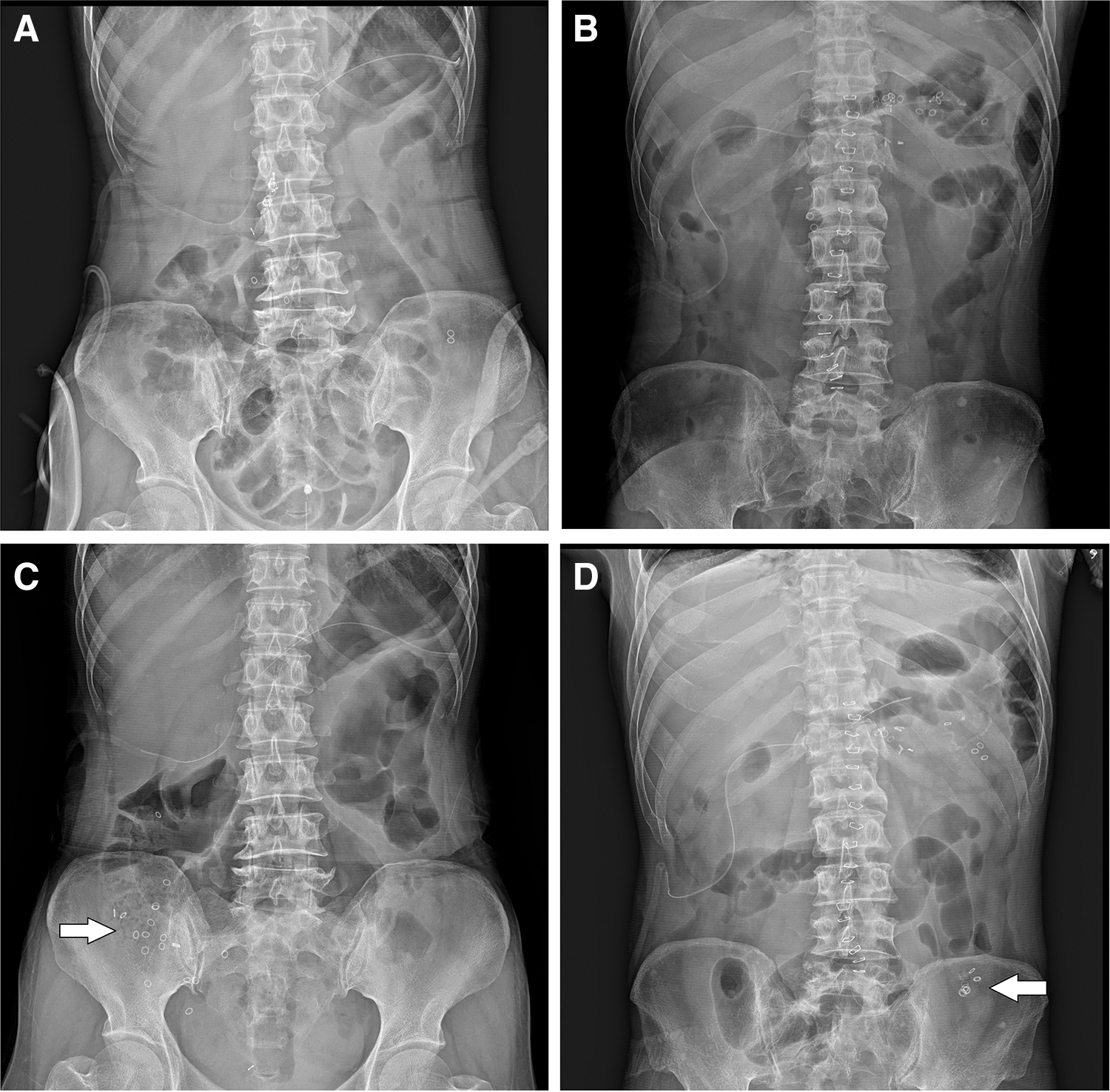
Remnant Sitz markers in the small intestine on abdominal radiograph of patients in the acupuncture and nonacupuncture groups.
The secondary outcomes included time to first flatus, start of sips water, start of soft diet, hospital stay, serum albumin level (to assess changes in nutritional status), and white blood cell (WBC) count and C-reactive protein (CRP) level (to assess acute inflammatory reaction changes).
Statistical analysis
A descriptive analysis was done to summarize the characteristics and operative outcomes using mean (standard deviation) and median (interquartile range) for quantitative variables and frequency (percentage) for qualitative variables. Comparisons of the characteristics and operative outcomes between the A and NA groups were analyzed by using the two-sample t-test for quantitative variables and the chi-square test for qualitative variables. The transit analysis of the Sitz markers and laboratory parameters by time, group, and interaction (time difference by group) effects was performed by using a repeated-measured two-factor analysis of variance. Contrasts were used for the multiple comparisons. All tests were two-sided, and p-values <0.05 were considered to represent statistically significant differences. SPSS software, version 19.0 (IBM, Inc., Armonk, NY) was used for the analysis.
Results
Patient demographic characteristics
Ten patients were enrolled and randomly assigned to the A (n = 5) or NA (n = 5) group. All recruited patients were available for the analyses of primary and secondary outcomes. No adverse events related to the use of acupuncture were reported. The study groups were similar with respect to demographic data and surgical details (Table 1). The patient characteristics were well balanced between the groups with respect to age, sex, body mass index, operation method, extent of gastric resection, postoperative stage, retrieved lymph nodes, and combined resection.
Values are expressed as number (percentage) of patients or as mean ± standard deviation.
BMI, body–mass index.
Primary outcome
The comparison between the numbers of remnant Sitz markers in the small intestine between the A and NA groups is shown in Table 2 and Figure 2. On postoperative day 1, all 20 markers remained in the small intestine in both groups. The A group had significantly fewer remnant Sitz markers in the small intestine on postoperative days 3 and 5 compared with those in the NA group. On postoperative day 3, only 5.8 ± 7.5 remnant Sitz markers were noted in the A group compared with 16.4 ± 5.68 in the NA group (p = 0.025). On postoperative day 5, all markers had passed through the ileocecal valve in the A group, and 6.6 ± 5.03 markers remained in the small intestine in the NA group (p = 0.005). On postoperative day 7, there was no significant difference between two groups because all 20 markers had already passed on day 5 in the A group. Overall, the A group showed faster Sitz marker passage than the NA group, which is shown as a significant difference in time and group interaction (p = 0.019) in Table 2.
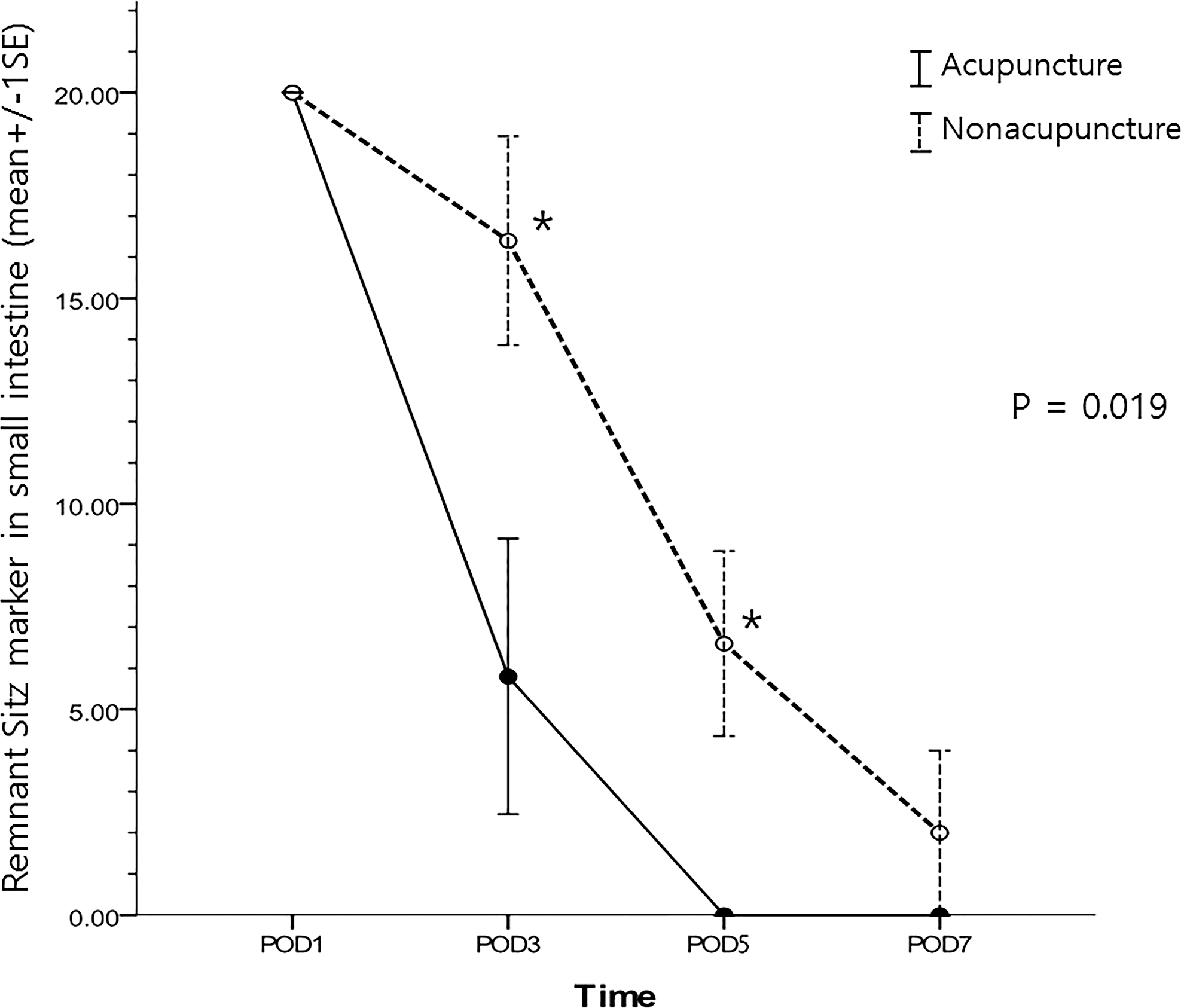
Comparison of the numbers of remnant Sitz markers in the small intestine between the acupuncture and nonacupuncture groups. Significantly fewer Sitz markers were found in the small intestine of the A group than the nonacupuncture group on postoperative days 3 and 5 (*p = 0.025 and 0.005, respectively). Significantly fewer remnant Sitz markers were detected in the acupuncture group than the nonacupuncture group with respect to the time and group interaction (p = 0.019). PO, postoperative.
Unless otherwise noted, values are expressed as mean ± standard deviation.
Result of the Mann–Whitney U-test for a non-normal distribution.
p < 0.05
Result of repeated-measures two-factor analysis of variance.
Result of multiple comparisons by contrast.
POD, postoperative day.
Secondary outcomes
Table 3 compares surgical outcomes between the A and NA groups. The A group tended to show relatively faster time to first flatus (2.4 ± 0.55 vs. 2.6 ± 0.55 days), earlier ingestion of water (2.8 ± 0.45 vs. 3.2 ± 0.45 day), earlier consumption of a soft diet (4.8 ± 0.45 vs. 5.2 ± 0.45 days), and shorter hospital stay (9.4 ± 2.07 vs. 11.2 ± 1.92 days) than those in the NA group, but no significant differences were detected (p = 0.549, 0.180, 0.180, and 0.206, respectively).
Unless otherwise noted, values are expressed as mean ± standard deviation.
Table 4 compares laboratory outcomes between the A and NA groups. Postoperative total WBC counts increased gradually and were significantly lower on postoperative day 5 in the A group than in the NA group (p = 0.028), but the difference was not significant for the time and group interaction (p = 0.415). Postoperative CRP levels in the A group were significantly lower on postoperative day 5 than in the NA group (p = 0.028), but the difference was not significant by the time and group interaction (p = 0.155). Postoperative albumin level decreased gradually in each group, but no significant difference was observed between the groups.
Result of the Mann–Whitney U-test for a non-normal distribution.
p < 0.05.
Result of repeated-measures two-factor analysis of variance.
Result of multiple comparisons by contrast.
Discussion
Acupuncture has been a minimally invasive integrative modality for GI motility disorders in China and Korea for thousands of years and is now being accepted by clinicians and patients in the West as an effective treatment option for various functional GI disorders. Acupuncture improves GI motility in laparotomy animal models 16 –19 and has a positive effect on GI motility in healthy volunteers, patients with diabetic gastroparesis, and those who underwent colonic surgery. 20 –25
To date, three properly conducted randomized controlled trials published in the English literature have assessed the role of acupuncture in POI after surgery. Meng et al. 25 randomly assigned 90 patients with prolonged POI to receive electroacupuncture or no acupuncture after surgery but failed to show significant differences between the two groups. Deng et al. 26 randomly assigned 81 patients to receive electroacupuncture or sham acupuncture after colonic surgery, but electroacupuncture did not reduce POI compared with sham acupuncture. Ng et al. 5 randomly assigned 165 patients who underwent elective laparoscopic surgery for colon cancer to receive electroacupuncture, sham, or no acupuncture after. As a result, electroacupuncture reduced the duration of POI, time to ambulation, and the postoperative analgesic requirement compared with those in the no- or sham-acupuncture groups. However, no studies have been conducted among patients who underwent gastric surgery. Therefore, the current study was conducted to evaluate the effect of acupuncture on reducing duration of POI after gastric cancer surgery.
In this study, the selection of acupoints was based on expert consensus provided by qualified and experienced KMDs. The style of acupuncture was Korean. Acupoint ST 36 was used, which is the most commonly used acupoint for reducing POI in clinical studies. 24,25 Electroacupuncture at ST 36 reduces the postoperative analgesic requirement and associated side effects in patients undergoing lower abdominal surgery. 27 The current study also used other acupoints, such as SP 6, LI 4, and TE 6, with electrical stimulation, which is effective in POI, 5 and LV 3 and LI 11, which are widely used acupoints to treat GI disorders. TE 6 is used in the treatment of chronic functional constipation, 28 LI 4 and SP 6 are used for alleviating abdominal pain, 29 and LI 11 has a positive therapeutic effect in treating internal organ disease. 30 Several clinical trials reported that acupuncture at LI 4 and LR 3 could modulate intestinal motility. 31,32 Although the GV 20, GV 26, CV 24, and EX HN3 points are located in the head, the meridian of these acupoints flows through the central vertical line of the body and is also effective in treating GI disorders.
The electroacupuncture therapy gives a stronger stimulus than simple acupuncture therapy. Electroacupuncture could alleviate many diseases or symptoms, such as pain, 33 stroke, 34 erectile dysfunction, 35 nausea and vomiting, 36 depression, 37 gastric motility, 38 and obesity. 39 Yin and Chen 40 reported that electroacupuncture has the potential for treating GI motility disorders. With regard to gastric motility functions, it seems that electroacupuncture might have therapeutic potential for functional dyspepsia and gastroparesis by enhancing gastric accommodation, slow waves, contractions, and emptying. 40
It is important to define specific parameters when evaluating a patient for POI. One commonly used parameter is time to recover GI function (gastrointestinal-3), which is a three-component composite endpoint that includes time until the patient first tolerates solid food, passes first flatus, and first bowel movement. 41 However, flatus is often regarded as an insensitive parameter, and the time to resume a diet can be influenced by the patient's perception and can be easily manipulated by the attending clinician. 42
Two techniques have been used to evaluate GI motility: transit of Sitz markers viewed by radiography and transit of radioisotope detected with scintigraphy. 43,44 The Sitz marker has been widely used for evaluation of GI transit because it is a simple and clearly identifiable marker and is accepted as a tool for diagnosing bowel motility disorders. 14,15 In this study, a Sitz marker capsule (20 Sitz markers per capsule) before anastomosis and counted the remnant numbers of markers in the small intestine on radiography. It was thought that this method could be useful to provide quantitative data for POI. Therefore, the numbers of remnant Sitz markers in the small intestine was used as the single primary outcome measure for this study. The patients in the A group had fewer remnant Sitz marker than the NA group on postoperative days 3 and 5, and the A group showed faster passage of Sitz marker than did the NA group. The results indicate that there was faster recovery of small bowel movement in the A group and that acupuncture might be able to reduce duration of POI after gastric cancer surgery.
Reducing duration of POI, which is a major cause of delayed discharge after abdominal surgery, is the most important objective of enhanced recovery after surgery (ERAS) protocols. The term ERAS is often used to describe a multimodal perioperative care program that was previously called “fast-track surgery.” 45 This program is composed of several evidence-based perioperative care elements that are individually beneficial and result in substantially improved surgical outcomes when used together. 46 –49 These protocols reduce time to a bowel movement by 1–2 days. In this way, this study demonstrated that acupuncture can be easily and safely applied to enhance recovery of bowel motility and could be used as a potential factor in ERAS protocols.
This study had some limitations. First, although the same postoperative management was applied in both groups, the A group had received more attention for at least 25–30 minutes per each day of acupuncture treatment compared with the NA group. The lack of interaction between physician and patient in the NA group could have affected the study results. Second, the small number of patients may have been insufficient to allow a comparison of the surgical outcomes, including time of first flatus, time to start ingesting water, time that patients tolerated a soft diet, and hospital stay. On the basis on the results, the authors started a prospective randomized largescale study in March 2015. This study is expected to determine whether acupuncture has beneficial effects on postoperative clinical outcomes. Finally, although the current study compared acute inflammatory response laboratory findings and WBC and CRP significantly differed between groups on postoperative day 5, these parameters are not specific and can be influenced by many factors and various situations. Furthermore, the meaning and clinical implication of these results are unclear because there were no significant differences in the time and group interaction for WBC or CRP (Table 4).
Conclusions
This study showed that the A group had significantly fewer remnant Sitz markers in the small intestine than did the NA group. This result may reflect the potential effect of acupuncture on reducing duration of POI after gastric cancer surgery, by earlier recovery of small bowel movement. The A group showed relatively faster time to first flatus, earlier start of water and soft diet, and a shorter hospital stay than the NA group, but no statistical differences were detected. Although further studies are warranted to confirm these findings, acupuncture may reduce the duration of POI among patients undergoing gastrectomy for gastric cancer. A more significant result is expected in the large-scale study based on this pilot study, and it is thought that acupuncture could be used as an ERAS protocol method for patients undergoing gastric cancer surgery.
Footnotes
Acknowledgment
This study was supported by a grant from Korea Health & Welfare, Republic of Korea (project no: 090-091-3000-3033-340-320-01).
Author Disclosure Statement
No competing financial interests exist.