
Abstract
Background:
Behavioral and psychological symptoms of dementia (BPSD) are a common problem among patients with dementia. This problem is usually treated by drugs, but they have limited efficacy and often cause adverse effects. Aromatherapy is a nonpharmacologic treatment that is simple to use and devoid of significant adverse effects.
Objectives:
To review the literature on the effectiveness of aromatherapy treatment in patients with BPSD.
Design:
A descriptive analysis of randomized clinical trials (RCTs) published in the English-language literature and cited in PubMed.
Results:
Eleven articles on RCTs were found, of which 1 had fewer than 10 participants, 2 were mistakenly presented as RCTs, and another did not report treatment for BPSD. In all, 7 articles with 417 participants total (range, 15–114) were reviewed. The mean age in all studies was greater than 69 years (range, 69–85 years), and the percentage of women was 55% (range, 50%–57%). The intervention period ranged from 10 days to 12 weeks. Two studies used Melissa oil and 5 others used lavender oil. The studies described different methods of administration for the oils, including spraying and rubbing over various body organs. The duration of treatment differed among the studies. In 3 studies the investigators concluded that the treatment was not effective and in 3 that it was effective; in 1 study no clear conclusion could be drawn.
Conclusions:
The difference between positive and negative studies was not explained by differences in the study population, the type of oil, or the duration of treatment. The significant difference apparently stems from the method of administration. When the oil was applied close to the olfactory system the outcome was positive. A study should be designed to assess the effect of the site of application of aromatherapy.
Introduction
D
Diagnostic Instruments for BPSD
The diagnosis of BPSD can be problematic given the broad spectrum of symptoms. The assessment of BPSD includes a basic diagnosis that takes the cause of dementia into account, as well as the negation of other factors, such as delusion from drug therapy or adverse effects of treatment for comorbid conditions (e.g., depression, pain, and sleep disturbances).
7
Today there are more than 30 different scales for the evaluation of the behavioral manifestations of BPSD. The most commonly used instruments for measurement are the following: 1. Cohen-Mansfield Agitation Inventory (CMAI).
8
This tool was developed in 1984. It is a 7-point scale that assesses the frequency of 29 types of agitated behavior, including restlessness, verbal and physical aggression, and yelling. A higher score signifies a higher level of agitation. 2. Pittsburgh Agitation Scale (PAS).
9
This scale measures agitation through the use of 4 behavioral groups: aberrant vocalization, motor agitation, aggressiveness, and resisting care. Each group gets a score ranging from 0 to 4, so the highest possible score is 16. The higher the score, the greater the degree of agitation. 3. Neuropsychiatric Inventory (NPI).
10
This scale evaluates 10–12 common behavioral disturbances in dementia: delusions, hallucinations, depression, anxiety, restlessness, aggression, euphoria, disinhibition, irritability or instability, apathy, and aberrant motor activity. A high score reflects a greater severity of behavioral disturbance. 4. Philadelphia Geriatric Center Affect Rating (PGCAR).
11
This is an instrument for the assessment of types of evident emotions noted over a 1-minute period of observation of the patient. The emotions are divided into 2 categories: positive (including pleasure, satisfaction, and interest) and negative (including anger, sadness, and fear/anxiety). The most outstanding emotion is scored as 1 and the others as 0.
Treatment of Patients with BPSD
The aim of treatment is to identify the problem and treat it before the caregiver is burned out and the damage is irreversible. The treatment of BPSD is usually based on antipsychotic drugs, which often cause adverse effects. Studies have shown that the use of antipsychotic drugs increases the risk for stroke and death, so the U.S. Food and Drug Administration recommends averting the use of these drugs in the treatment of dementia. 12 Nonpharmacologic treatment is an effective alternative for coping with BPSD symptoms. In the last decade there has been a trend toward the use of complementary and alternative medicine. 13
Use of Aromatherapy
Recently, aromatherapy has been used in the treatment of BPSD to improve sleep and to reduce behavioral disturbances. Aromatherapy is based on the use of essential oils to affect the brain and the body. The oils enter the bloodstream and react with hormones and enzymes, causing a physical response. Essential oils are absorbed into the body through the digestive tract, the mucosa, the olfactory system, and the skin. 13 The hypothalamus and the thalamus are involved in behavioral aspects, such as motivation and emotion. They regulate body activities by control and activation of the autonomic nervous system and the neuro-endocrine system. Aromatherapy, by means of the essential oils, can modulate emotional reactions in these tracts by inhalation alone. 14 Despite an increased use of aromatherapy, few studies have provided evidence for its effectiveness. Although the use of essential oils has shown a positive effect on anxiety, there is not enough evidence of its effect on depression and behavioral problems. 14
This study consists of a comprehensive review of randomized controlled trials (RCTs) of aromatherapy in the treatment of BPSD.
Materials and Methods
English-language papers cited in PubMed from January 1965 to December 2014 and reviewed in this study were identified by using the search terms “dementia” and “aromatherapy.” Papers with potentially relevant titles underwent a preliminary review through reading of the abstracts. Only RCTs that evaluated the clinical application of aromatherapy in patients with dementia were included. In all, 62 papers were reviewed. Of these, 15 were clinical trials and 11 were RCTs. Of these 11 studies, 1 was found not to be an RCT upon review, 1 was a letter to the editor, 1 had a study population of only 10 patients, and 1 used aromatherapy for cognitive improvement and did not directly assess its effect on agitation. Thus, the present review included seven studies. Figure 1 summarizes the process in which studies included in this report were selected.
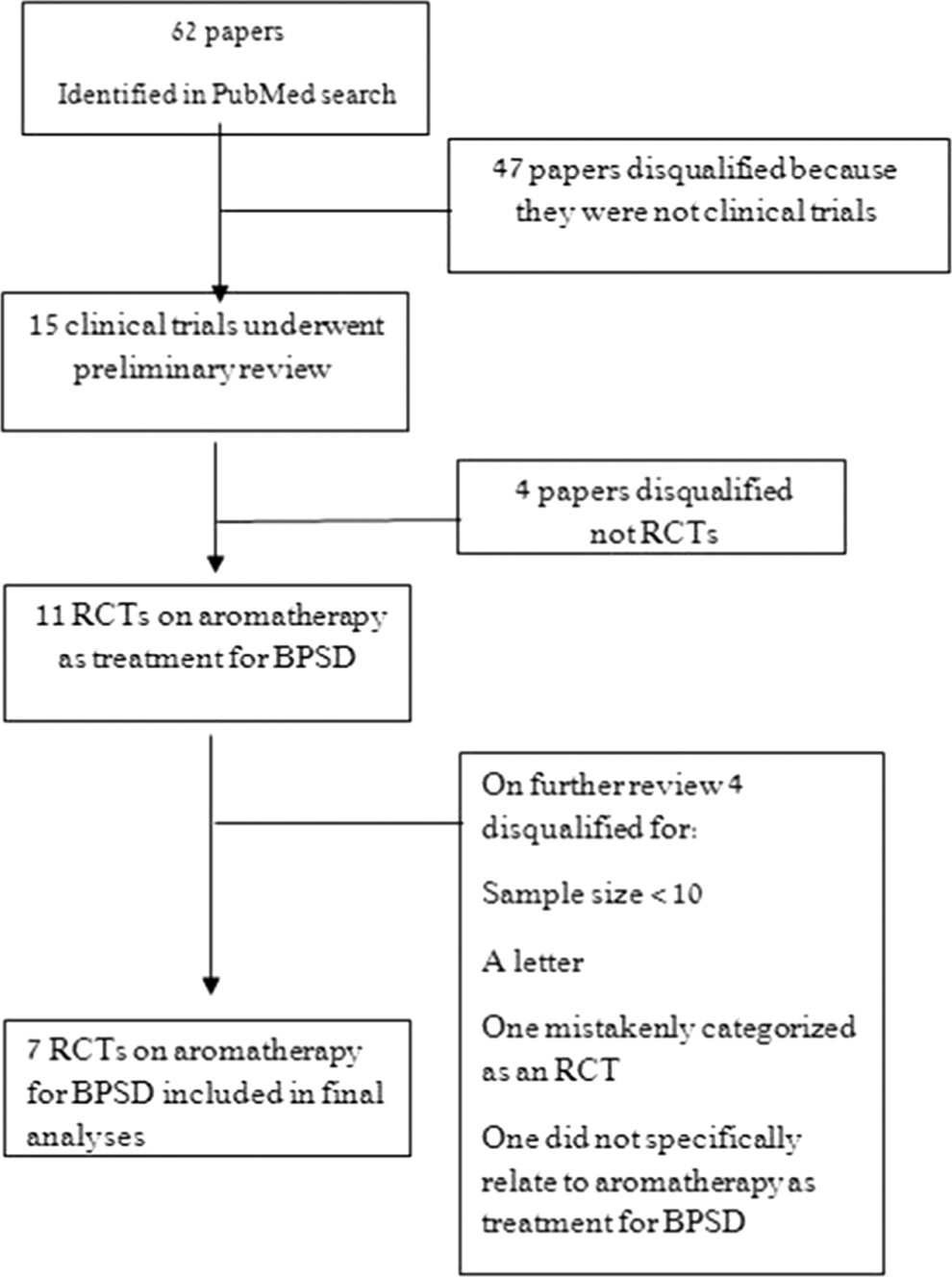
Flow diagram of the selection process for the literature review. BPSD, behavioral and psychological symptoms of dementia; RCT, randomized controlled trial.
Results
The studies are summarized in Table 1. A study by Fu et al. 16 included 61 patients (36 women) who had dementia with a history of agitation and aggression. The mean age was 84.6 ± 6.4 years. The study was funded by the Queensland Nursing Council (noncommercial funding). The patients were sampled from three long-term care nursing homes in Brisbane, Australia.
GC/MS, gas chromatography–mass spectrometry; CMAI, Cohen-Mansfield Agitation Inventory; NA, not available; PGCAR, Philadelphia Geriatric Center Affect Rating; NPI, Neuropsychiatric Inventory; PAS, Pittsburgh Agitation Scale.
On the basis of power calculations, the sample size required for each study group was 15 patients. The study had three groups: (1) 22 patients who received three spray applications of lavender oil to the chest, avoiding the face; (2) 19 who had lavender oil administered by three sprays to the chest and massaged into the palms of the hand; (3) 20 patients in a control group who had water sprayed onto the chest (placebo).
The study continued for 6 weeks, during which each group was treated twice a day (morning and afternoons). Agitation was measured by CMAI at baseline; at 2, 4, and 6 weeks of treatment; and 6 weeks after the end of treatment (in all, 5 measurements). There was a statistically significant reduction in aggressive behavior in the two treatment groups and the control group; p < 0.05). The mean CMAI scores were not reported, but there was no statistically significant difference in CMAI among the groups throughout the study.
A study by Lin et al. 17 included 70 elderly patients (41 women) with dementia who had clear manifestations of agitation (based on the Chinese version of the CMAI). The patients were sampled from care and attention homes in Hong Kong, China. The mean age of the patients was 78.3 ± 4.1 years. Sample size calculations were performed but not described in the paper. The study had a crossover design with two types of treatment: (1) aromatherapy by inhalation of lavender oil during sleep from specially designed machines that were placed by the caregivers next to the patient's pillow for 1 hour at night and (2) placebo therapy with sunflower oil using the same method of application.
The patients were allocated randomly into the two groups, with each group receiving one of the treatments for 3 weeks, followed by no treatment for 2 weeks and then the second treatment. The effect of the treatment was measured by CMAI and the NPI at baseline and at the end of each treatment period. There were no dropouts, and no adverse events were reported. There was no restriction on the use of psychiatric drugs during the study, but dose, number, and type of drug did not change during the study. The investigators reported a decrease in mean NPI scores from 24.7 to 17.8 (t = 14.6, df = 69; p < 0.001) and CMAI scores from 63.2 to 58.8 (t = 10.8, df = 69; p < 0.001) after 3 weeks of treatment with lavender compared with no significant changes with placebo (NPI changed from 24.3 to 24.4 [p = 0.24] and CMAI from 63.94 to 63.90 [p = 0.52]). There was a significant reduction in the five types of behavior in the NPI score after treatment with lavender compared with placebo. The agitation score dropped from 6.5 to 5.6 (p < 0.0001), the dysphoria score dropped from 0.34 to 0.13 (p = 0.03), the irritability score dropped from 5.39 to 4.61 (p < 0.001), and the aberrant motor activity dropped from 4.81 to 3.63 (p = 0.01). A parallel improvement occurred in the nighttime behavior score (p = 0.001). The withdrawal period between treatments had no effect on NPI (t = 0.26, df = 34; p = 0.87) or CMAI (t = 0.19, df = 34; p = 0.24). The authors concluded that lavender oil is an effective supplementary therapy for agitation in patients with dementia. Funding for the study was not cited.
The study by O'Connor et al. 18 included 64 elderly patients (59% women) who were diagnosed with mild or more severe dementia on the Clinical Dementia Rating Scale but had severely impaired cognitive (mean Mini-Mental Status Examination score of 6.1 ± 7.0) and features of agitation (mean CMAI score, 40.3 ± 18.8) that were not caused by pain, disease, depression, or psychoses. The patients were sampled from eight psychogeriatric nursing homes and three private nursing homes in Melbourne, Australia. The mean age was 77.6 ± 9.4 years. The required sample size was calculated but not described in the Methods section of the paper. The study had a cross-over design and included two types of treatment: (1) aromatherapy given by rubbing lavender oil on the forearms and (2) jojoba oil administered in the same way (control).
Each treatment was administered three times a day for 1 minute to each forearm. Each treatment period lasted for 3 weeks, with a four-day break before crossover to the other treatment. Measurements were conducted 30 minutes before treatment, during the first 30 minutes, and at 30 minutes after treatment. The research assistants followed the patients' behavior using the Philadelphia Geriatric Center Affect Rating. In addition, five types of behavior were measured, which included taking steps, repetitive behavior, restlessness, undressing, and intrusiveness. All the measurements are presented as means of a daily 30-minute observation period with the number of behaviors recorded every minute.
The investigators found fewer incidents of agitation in the aromatherapy group than in the placebo group, with a difference that almost reached statistical significance (incidence rate ratio [IRR], 0.884; 95% confidence interval [CI], 0.778–1.004); p = 0.57). However, the aromatherapy group's score was also lower at baseline, so the outcome indicates a lack of effectiveness for the therapy. Exposure time also did not affect the results at the first exposure (IRR, 0.961; 95% CI, 0.798–1.15; p = 0.672) or the second exposure (IRR, 1.045; 95% CI, 0.869–1.259; p = 0.636). Similar results were found for the patients' emotions. The score for positive emotion was higher in the treatment group than the control group, but the difference was not statistically significant (IRR, 1.072; 95% CI, 0.848–1.355; p = 0.56). Exposure time also did not affect this variable the first time (IRR, 1.020; 95% CI, 0.726–1.433; p = 0.910) or the second time (IRR, 0.954; 95% CI, 0.675–1.348; p = 0.790). The investigators concluded that treatment with lavender oil was not effective in the treatment of patients' behaviors or emotions. The study was supported by the National Health and Medical Research Council and the Dementia Collaborative Research Center.
A study by Holmes et al. 19 included a small sample of 15 patients (60% women) who were diagnosed with severe dementia (according to International Classification of Diseases, 10th revision). All the patients had agitation (a score of 3 or higher on PAS). This was a pilot study, so sample size calculations were not provided. The patients were sampled from the closed ward of the Allington Behavioural Center for Dementia, Moorgreen Hospital, United Kingdom. The mean age was 79.0 ± 6.3 years. The study had a crossover design and assessed two types of treatment: (1) aromatherapy with lavender oil sprayed into a common living area unit for 2 hours and (2) spray with water (placebo) under identical conditions.
The two treatments were given on alternate days over a 10-day period, so that each type of treatment was given five times. After a 2-hour treatment period (from 4 p.m. to 6 p.m.), agitation was assessed for 1 hour by research assistants using PAS. About 60% (9 of 15 patients) showed an improved agitation score, while about 33% (5 of 15) did not improve at all; 7% (1 patient) had a worse score after aromatherapy. The mean PAS score after aromatherapy was 3 compared with 4 after placebo therapy (p = 0.016).
The investigators concluded that aromatherapy with lavender oil spray reduces agitation in cases of severe dementia. However, because this was only a pilot study with a small sample size, a larger study is required to assess the best treatment modality for aromatherapy and the different types of reactions.
In a study by Smallwood et al., 20 the study population included 21 patients (12 women) with severe dementia, as determined by a psychiatrist. The patients were sampled from a hospital ward (not identified by the authors) in England. The mean age was 66.8 ± 11.5 years. Sample size calculations were not reported. The study included three treatment groups: (1) treatment with Lavender oil by massage (the article did not state where the oil was rubbed in or the duration of treatment); (2) treatment with simple oil in a similar manner (no further details were provided); (3) conversation with the patient together with the spraying of lavender oil through a disperser (no further details were provided). In all three study groups, the treatment was given twice over the course of the week.
The patients were videotaped for 15 minutes each time to record their behavior. This was done at four different time periods over the 2-week study: 10–11 a.m., 11 a.m. to noon, 2–3 p.m., and 3–4 p.m. Behaviors of an agitated nature were defined by the Bowie and Mountain criteria from 1993 and graded by scorers who were not involved in the study.
The results of the study indicate less agitation in the group that received aromatherapy by massage than in the other groups, but the difference was not statistically significant (p > 0.1). In contrast, there was a correlation between the time of day that the massage was given in the group that received aromatherapy by massage and the outcome, with the largest improvement seen between 3 p.m. and 4 p.m. (F[2,15] = 3.721; p = 0.05) in the massage aromatherapy group compared with the group that received spray aromatherapy with conversations. The authors concluded that aromatherapy by massage reduces agitation primarily when applied between 3 p.m. and 4 p.m. The study was funded by a Chief Scientist Office grant (noncommercial).
The next two studies used Melissa oil to treat agitation in patients with dementia. The study by Ballard et al. 21 included 72 patients with severe dementia (43 women) from eight nursing homes in the National Health Service. The patients were diagnosed with agitation by the CMAI and NPI scales. Ninety-two percent of the patients continued to take psychiatric medications, and any change in dosage or type of drug was recorded. The mean age was 78.5 ± 8.1 years. The calculated sample size was 30 patients in each of the two treatment groups: (1) aromatherapy with Melissa oil in the treatment group and (2) placebo therapy with sunflower oil in the control group.
In both studies the oil was integrated into a body cream and rubbed into the patients' faces and arms. The treatment was given twice a day for 4 weeks. CMAI and NPI measurements were conducted once a week for the 4-week intervention period.
The baseline characteristics of the two groups were similar except for higher CMAI scores in the treatment group. The results of the study showed an improvement of 35% in the CMAI score in the treatment group, which decreased from 68.3 ± 15.3 to 45.2 ± 10.4 (p < 0.0001) and an improvement of 11% in the CMAI score in the control group, which decreased from 60.6 ± 16.6 to 53.3 ± 17.7 (p = 0.0005).
When the total CMAI score was compared between the two study groups over the 4-week study period, 60% of the treatment group but only 14% of the control group had an improvement of 30% or more in the total CMAI score (chi-square = 16.3; p < 0.00001), which was set as the threshold for clinical significance in BPSD. The most significant improvement occurred 1 week after the initiation of treatment. There was also a significant improvement in quality of life in the aromatherapy treatment group compared with the control group. For example, there was a greater decrease in the percentage of time that the elderly patients were socially isolated in the aromatherapy treatment group compared with the controls (a decrease of 5.6 points compared with 1.4 points; Z = 2.6; p = 0.005). The investigators concluded that the use of aromatherapy for the treatment of agitation in patients with severe dementia is effective and safe. In addition, the treatment had a positive effect on measures of quality of life in elderly patients. Funding for this study was not cited.
A study by Burns et al. 22 included 114 patients (66 women) who were diagnosed with dementia, with a score of 3 in the Clinical Dementia Rating test and with features of agitation as diagnosed by a score of 39 or above on the CMAI. The patients were sampled from three centers in England. The mean age was 85 years. Sample size calculations indicated that 40 patients were needed in each treatment group to reach a power or 80%. The patients were allocated to three treatment groups: (1) aromatherapy with Melissa and a drug placebo; (2) active treatment with donepezil, which was previously shown to be effective in the treatment of agitation, 23 with aromatherapy placebo (sunflower oil); (3) double placebo.
The active and placebo oils (Melissa and sunflower seeds) were integrated into a body cream and applied by massage on the hands and the arms for 1–2 minutes twice a day for 12 weeks. The active drug was given in a dose of 5 mg/d for 1 month, after which the dose was increased to 10 mg/d. The following parameters were assessed in the study: symptoms of agitation by PAS and NPI as a measure of behavioral symptoms. Both of the parameters were measured at baseline and at the 4th and 12th weeks of the study. The investigators found no differences among the three treatment groups for PAS and NPI scores at any point in the study, but there was a significant difference in the quality-of-life score between baseline and 12 weeks between the aromatherapy group and the active drug group (p = 0.033). Quality of life significantly decreased in the donepezil group compared with the group treated with Melissa oil. The only significant difference in the subvariables of the NPI scale among the three study groups was in dysphoria/anxiety, where there was a decrease of 50% in the aromatherapy group compared with a 19% decrease (p = 0.017). Remarkably, placebo therapy was effective after 12 weeks, with an improvement of 18% in the PAS score for agitation and 37% in the NPI, which measures a spectrum of neuropsychiatric symptoms. The investigators concluded that aromatherapy has no advantage over active treatment with donepezil or placebo. The act of intervention per se led to an overall benefit in all groups, including the placebo group. The study was supported by the Alzheimer's Society.
Discussion
This study surveyed papers that reported the results of RCTs published to date in English in order to clarify whether aromatherapy with Melissa/lavender improves symptoms of agitation in these patients. The literature review included seven studies with an overall patient population of 417 patients with dementia.
Three of the seven studies (Ballard et al., 21 Lin et al., 17 Holms et al. 19 ) showed a beneficial effect in the treatment of BPSD symptoms in patients with dementia. In contrast, the studies by Burns et al., 22 Fu et al., 16 and O'Connor et al., 18 showed no beneficial effect or a similar effect in all treatment groups (including the placebo group). The seventh study, by Smallwood et al., cannot be categorized as positive or negative for reasons discussed below.
In theory, there could be several explanations for the inconsistent results, including the study population, the type and method of treatment, and the methods of outcome measurement.
Was there a difference between the positive and negative studies in terms of study population?
In the positive studies, the patients' age ranged from 78 to 79 years. Most of the patients were sampled from elderly nursing homes or hospital wards. The percentage of women in the studies was 60%, and all the patients were diagnosed with moderate to severe dementia. In the negative studies, the mean age ranged from 78 to 85 years, and most of the patients were women (59%). The patients were sampled from elderly nursing homes and hospital wards and were diagnosed with severe dementia. Thus, differences in the study population probably do not explain the difference in results.
Are there differences between the positive and negative studies in terms of treatment method?
A comparison of the various studies shows that the method of administration of the treatment was different between the positive and negative studies. In the negative studies, 16,18,22 the oil did not make direct contact with the face in general or with the nose in particular (i.e., the site of administration of the treatment substance was relatively far from the olfactory system). In contrast, in the positive studies, 17,21 there was direct stimulation of the olfactory system, 19 whether by spraying or direct application of the oil on the face. Thus, it would appear that aromatherapy has to affect this system to achieve an optimal result.
On the basis of comparisons of the studies, it does not appear that the type of oil was associated with effectiveness. In the case of both Melissa and lavender oils, some studies had negative outcomes and others had positive outcomes.
If the studies by Ballard et al. 21 and Burns et al. 22 are left out of the analyses, it appears that the length of time of active therapy affected its effectiveness. In the studies by Holmes et al. 19 and Lin et al., 17 there was a significant improvement in agitation after 1 and 2 hours of treatment, respectively. In contrast, in the negative studies by O'Connor et al. 18 and Fu et al., 16 the duration of treatment was relatively short at a few minutes per day. However, when the positive study by Ballard et al. 21 which showed a significant clinical improvement of 30% in agitation among patients treated by rubbing Melissa oil on the face, is compared with the negative study by Burns et al. 22 (Melissa oil rubbed into the hands and arms), the duration of treatment was identical at 1–2 minutes. Therefore, there is no clear association between the duration of therapy and its effectiveness.
Was there a difference between the negative and positive studies in methods used to assess BPSD symptoms?
The method of assessment of BPSD was not uniform among the seven reviewed studies. The positive studies used the PAS, CMAI, and NPI scales and the negative studies used the PAS, CAMI, NPI, and PGCAR scales. Thus, it is difficult to determine whether there was an association between the type of scale used for BPSD symptoms and the study outcome.
Other variables
Other variables could also have influenced the results. Did the placebo actually serve as a control treatment? For example, in the study by O'Connor et al., 18 no difference was found between the aromatherapy group and the control group, which received jojoba oil as placebo. The lack of difference between the two study groups might be related to jojoba having a similar effect as the essential oils. In this case the study oil (lavender) appeared to have a reduced effect compared with the “placebo.” A similar effect might also have occurred in studies that used sunflower seed oil. Thus, the choice of placebo might be problematic, and water should be used as placebo in control groups. In addition, the contact with the patients per se might have had a beneficial effect on agitation as reported by Fu et al., 16 Burns et al., 22 and Ballard et al., 21 independent of the effect of aromatherapy. All three studies showed a positive effect in the placebo group.
Beyond any doubt, the comparison of the studies by Burns et al. 22 and Ballard et al. 21 strengthens the assumption that applying the treatment through the olfactory system improved symptoms of BPSD. The two studies were conducted in a similar manner, the time of treatment was similar, the type of population was similar (the studies were also conducted in the same country), the oil was the same, and in both studies one of the scales was NPI. The only parameters that differed between the two studies were the method of treatment and the target organ that it affected. In Ballard and colleagues' study, 21 the treatment was administered close to the olfactory system, whereas in Burns and colleagues' study, 22 it was applied to the arms.
The characteristics of essential oils, such as their species as specified by their botanical name and chromatography–mass spectrometry characteristics, could affect the results of the studies. These characteristics were presented in only a small portion of the studies (Table 1). The absence of these data precludes a full comparisons among the studies.
Smallwood and colleagues' study 20 included a small sample (only 21 patients, with 7 in each of three study group). Many parameters, such as whether the treatment was applied close to the olfactory system and the duration of treatment, were not reported, making it difficult to categorize its outcome as positive or negative. In addition, the instrument used for scoring was subjective (viewing the patients' behavior in a videotape). Thus, this study was not included among the conclusive studies.
Although a study by Akhondzadeh et al. 15 assessed aromatherapy, it was not included in the review because it assessed cognitive parameters in Alzheimer's disease rather than BPSD. Yet there was an interesting “side effect” in that rate of agitation was reduced in the treatment group of this study. Thus, this study does shed further light on the effectiveness of Melissa oil on agitation, and it appears likely that Melissa oil does significantly improve measures of agitation.
Conclusions
In the authors' estimation, the factor that has a positive effect on aromatherapy is proximity to the nose in inhalation therapy. Additional studies are required to elucidate the therapeutic effectiveness of aromatherapy as an alternative to conventional drug therapy in the treatment of BPSD symptoms. Effective therapy can alleviate the suffering of elderly patients and the significant burnout that affects primary caregivers. Indirectly, it can reduce the rate of institutionalization, with its high cost, in elderly patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.