
Abstract
Objective:
This study aimed to demonstrate the effect of self-exercise with a therapeutic inflatable ball (SEIB) in elderly patients with myofascial pain syndrome.
Design:
Single-blind, randomized, controlled noninferiority trial.
Setting:
University campus.
Participants:
Forty elderly patients with myofascial pain syndrome completed the study. They were randomly allocated to SEIB (n = 22; mean age, 70.23 ± 6.11 years) or ultrasound (US) therapy (n = 18; mean age, 67.99 ± 5.64 years).
Intervention:
SEIB and US therapy (twice weekly for 4 consecutive weeks).
Outcome measures:
Visual analog scale (VAS), pressure pain threshold (PPT), and cervical lateral flexion (CLF) were measured at baseline and at 1, 2, 3, and 4 weeks.
Results:
The noninferiority test indicated that SEIB was not inferior to US for VAS, PPT, and CLF. Between-group comparisons showed no significant differences in the VAS (F = 2.579; p = 0.117), the PPT (F = 0.245; p = 0.624), and the CLF (F = 2.072; p = 0.159). In within-group comparisons, both groups presented significant differences in VAS (SEIB after 1 week and US after 1 week), PPT (SEIB after 3 weeks and US after 4 weeks), and CLF (SEIB after 4 weeks and US after 4 weeks) compared with baseline values.
Conclusions:
SEIB for 4 weeks has an effect similar to that of US for desensitizing myofascial pain and increasing joint flexibility. High accessibility and low cost would make SEIB a practical self-treatment method in elderly patients with myofascial pain syndrome.
Introduction
W
Instruction in self-treatment enables patients with musculoskeletal pain to exercise at any convenient time and place to prevent exacerbation of symptoms and secondary musculoskeletal disease. 11 –13 In particular, self-exercise for myofascial release is frequently recommended for treatment of musculoskeletal pain and restoration of extensibility of soft tissue. 14,15 Self- exercise for myofascial release is usually performed with compression tools, such as a foam roller or a tight ball, which are relatively simple to use, inexpensive, and easily available. 16,17
A therapeutic inflatable ball is also available for treating MTrPs, especially in the early stages of treatment. 18 The firmness of the therapeutic inflatable ball is easily adjusted by controlling the amount of air pressure according to individual need, and the ball would be suitable as a self-treatment tool. 18 Moreover, the therapeutic inflatable ball can concentrate pressure at specific areas, such as MTrPs. However, clinical evidence remains insufficient regarding the effect of self-exercise with a therapeutic inflatable ball (SEIB) for desensitizing MTrPs. Thus, additional empirical evidence is required to validate the use of the SEIB as a treatment method in elderly patients with myofascial pain syndrome.
Therefore, the current study aimed to demonstrate the therapeutic effect of SEIB techniques in the elderly with myofascial pain syndrome. Ultrasound (US) therapy was the control intervention because it is a common and useful clinical tool to desensitize MTrPs, among the techniques available in clinics. 19 –22 The study hypothesis is that SEIB is not inferior to US therapy in terms of reducing pain, pressure sensitivity, and increasing neck flexibility. Another hypothesis is that both SEIB and US therapy would show significant treatment effects on myofascial pain syndrome within 4 weeks. To test these hypotheses, elderly patients with myofascial pain syndrome received SEIB and US therapy for 4 consecutive weeks.
Materials and Methods
Study design
This study was a single-blind, randomized, controlled noninferiority trial. Participants who satisfied the inclusion criteria were randomly allocated to the SEIB or US group. They received eight sessions of treatment over 4 consecutive weeks in two treatment rooms in the physical therapy department of the university. To avoid conversing among the participants and subsequent contamination of the results, the two groups received treatment on different days. For all participants, measurements included subjective pain intensity, pressure pain threshold (PPT), and cervical lateral flexion (CLF) at baseline and at 1, 2, 3, and 4 weeks of therapy. Two physical therapists with at least 6 years of clinical experience were evaluators. They did not receive any information about the group allocation or the type of treatment used in each group and were not involved in treatment.
Participants
Forty elderly individuals participated in the study. All participants had MTrPs in the upper trapezius on at least one side for 3 months or longer. The diagnosis of MTrPs was based on the following criteria: (1) palpable, hypersensitive tender spot in a taut band; (2) pain reproduced by compression of the tender spot; (3) local twitch response on muscle palpation or snapping; and (4) referred and spontaneous pain elicited by firm compression. 23,24 Participants were excluded from the study if they had a history of surgery in the neck and shoulder or neurological deficits in the upper extremities. Those receiving another or ongoing treatment, or who had been medicated for 1 month or longer, were also excluded. 25 The purpose and procedures of this study were explained to all the participants, and informed consent was obtained before participation in this study. This study was approved by the Korea University Institutional Review Board (KU-IRB-14-179-A-1).
Randomization
After baseline data were recorded, the participants who satisfied the inclusion/exclusion criteria were randomly allocated to the SEIB or US group by using an online randomization tool (
Sample size
The sample size for the noninferiority trial was calculated. 26 The noninferiority margin was set at 1.5 cm on a 10-cm visual analogue scale (VAS) 27 as the acceptable difference between SEIB and US. The type I error rate was set at 2.5%, with a desired power of 90%. By using these parameters, a sample size of 19 participants was calculated for each group; one participant was added to each group to allow for a dropout rate of 5%. Thus, the plan was to recruit at least 20 participants per group.
Treatments
Two physical therapists with over 4 years of clinical experience performed US therapy on the patients in the US group. US therapy (Sonoplus 992, Enraf-Nonius, Delft, the Netherlands) was performed for 5 minutes in each of eight treatment sessions, with 1 MHz continuous wave, 1.0 W/cm2 of intensity, and a duty cycle of 100%. 28,29 The physical therapist applied US transmission gel (Aquasonic 100, Parker Laboratories, Fairfield, NJ) on an area of 40 cm2 around the marked MTrPs and performed slow circular movements at a speed of about 2–3 cm/s using the transducer head.
Patients in the SEIB group used a durable silicone therapeutic inflatable ball (Good Ball, Korean Association of Self-Release, South Korea) measuring 6.5 cm in diameter. Two physical therapists with over 3 years of clinical experience participated in the instruction of the SEIB group. Using a prepared document, they explained the purpose and detailed application method of SEIB for 1 hour before the first treatment session. To provide tailored pressure, patients adjusted the compression of the therapeutic inflatable ball themselves using an air pump, depending on the sensitivity of the MTrPs. It was recommended that the pressure be as high as tolerable because higher pressure is reportedly more beneficial for increasing the flexibility of soft tissue. 30 As patients began to experience less discomfort and pain with progressive sessions, the hardness of the inflatable ball was increased. At every SEIB treatment session, physical therapists recorded the application site and total number of treatment sessions.
The application and procedure of SEIB focused on releasing soft tissue tension, which was responsible for MTrPs in the upper trapezius. All participants performed three stages of SEIB for a total of 10 minutes, and each stage comprised one, two, and two trials, respectively (Fig. 1). All trials were maintained for 1 minute, with 1 minute for rest and change of position between each trial.
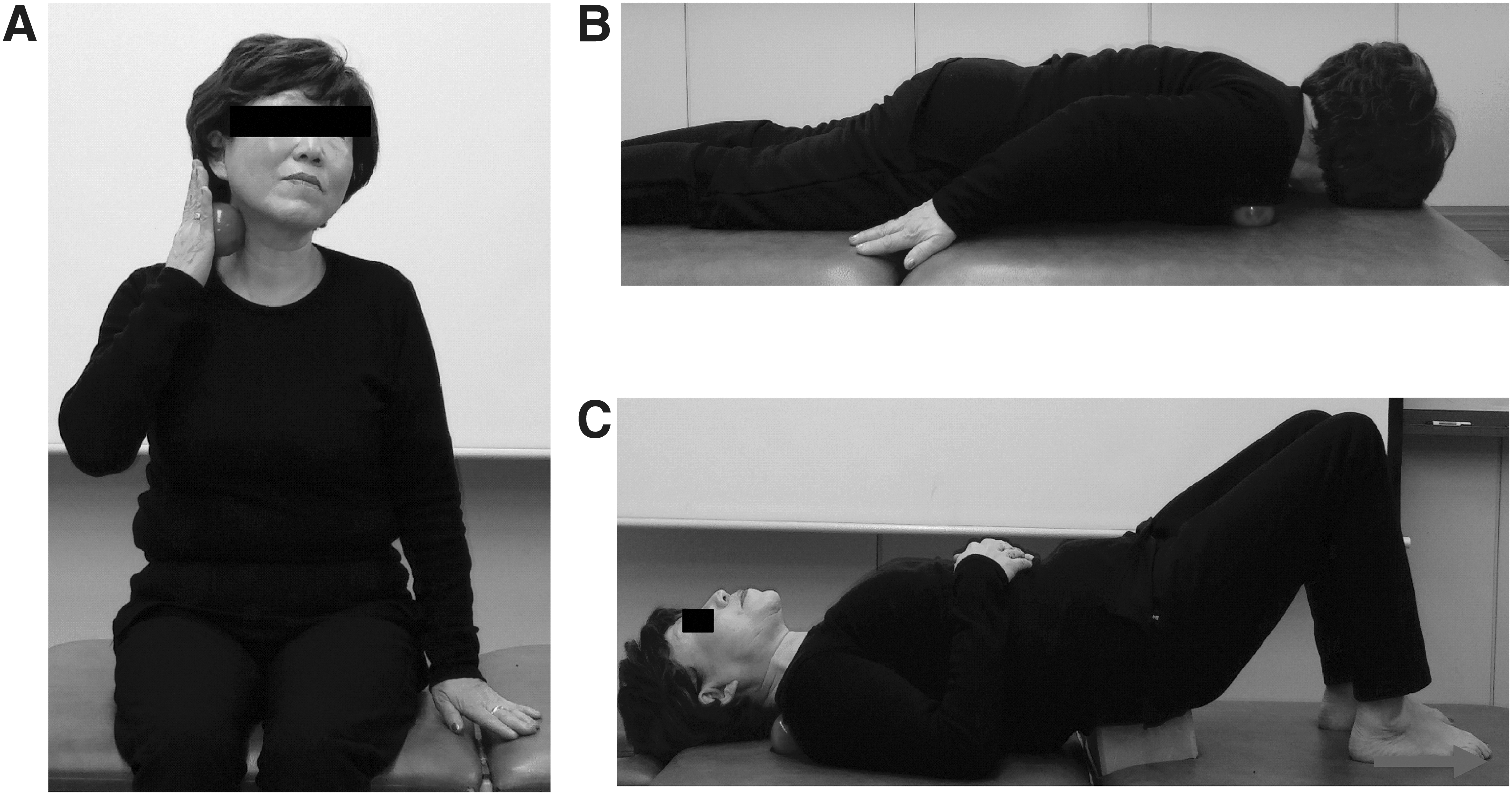
Steps for SEIB.
In the first stage, to release the tension in the sternocleidomastoid, patients in the sitting position gently rubbed the upper third of the sternocleidomastoid in circular motions with the therapeutic inflatable ball for 1 minute. This area was chosen because it is the site of penetration by the accessory nerve, which is responsible for the motor control of the upper trapezius. Compression of the nerve where it passes through the taut bands of the sternocleidomastoid muscle can cause ischemic pain and weakness in the innervated muscle. 31 In the second stage, to restore muscle balance, patients located the painful spot at the midpoint of the pectoralis major on the nipple line just below the fourth rib by adjusting the position of the therapeutic inflatable ball while in the prone position; pressure was maintained for 1 minute and repeated twice. This exercise was included because muscle imbalance between the pectoralis major and upper trapezius might be a secondary cause of MTrPs in the upper trapezius. 32 In the third stage, to desensitize MTrPs, patients applied pressure directly to the marked MTrPs in the upper trapezius with the therapeutic inflatable ball in a crook lying position. To concentrate the pressure on the marked MTrPs, a yoga block was positioned under the lumbopelvic area, and the patients were then asked to push toward the ground with the feet directed slightly downward for 1 minute and repeated twice.
Clinical outcomes
At baseline, the evaluator, a physical therapist with 8 years of clinical experience, searched for tender spots and then confirmed MTrPs using ultrasonic imaging. 20 If a participant had multiple MTrPs or involvement of both sides of the upper trapezius, the most painful MTrPs were selected by compression. The MTrPs were marked on the skin by using a pen, and medical tape was applied to the MTrP to ensure a consistent site for treatment and measurement. The medical tape was changed after every treatment. The Mini-Mental State Examination-Korean version (MMSE-K) and Short Form 36 Health Survey (SF-36) were also administered to each participant to evaluate cognitive status and health-related quality of life. In addition, PPT, subjective pain intensity, and CLF were measured at baseline and at 1, 2, 3, and 4 weeks. Outcome variables were measured three times at 30-second intervals; the total measurement time was less than 15 minutes. The order of clinical outcome measurements was as follows: CLF, subjective pain intensity, and PPT. For all measurements, patients sat on a flat-surfaced stool with no arm or back supports.
CLF was measured with an electronic goniometer (Nippon Medical and Chemical Instruments Co., Ltd., Osaka, Japan) and the greatest range of motion was recorded. With respect to the starting position for measuring CLF, the proximal goniometer arm was placed on the spinous process of the T1 vertebra and perpendicular to the floor, the central fulcrum of the goniometer was placed on the spinous process of C7, and the distal arm was placed on the spinous process of C2. 33
Subjective pain intensity was measured by using the VAS. This 10-cm horizontal line is divided into 10 equal parts, where 0 indicates no pain and 10 indicates the worst imaginable pain. Participants were asked to check the VAS when a mechanical pressure of 4.5 kg/cm2 was exerted on the marked MTrPs with a pressure algometer (FPK 20, Effegi, Alfonsine, Italy).
PPT was measured with a pressure algometer consisting of a dial gauge that could be set from 0 to 7.7 kg/cm2 and a rod. The end of the rod was a 1-cm-wide plastic plate; this was placed in direct contact with the marked MTrPs, and vertical pressure was applied to these MTrPs at a speed of 1 kg/s 34 until the participant expressed the first sensation of pain. 28 The evaluator recorded the amount of pressure at the moment of pain. In the current study, intra-examiner reliability showed high repeatability (intraclass correlation coefficient(3,1) = 0.83), and the 95% confidence interval (CI) ranged from 0.74 to 0.90.
Statistical analysis
The VAS, PPT, and CLF variables are reported as mean and standard deviation values averaged over three measurements. Normal distribution was estimated with the Shapiro-Wilk test. Independent t-test and chi-square tests were conducted for the homogeneity of demographic characteristics and for the MMSE-K and SF-36 scores.
To determine whether the SEIB was inferior to US, the CI approach was used. 35 The noninferiority margins were set at 1.5 cm on the VAS, 27 1 kg for the PPT, 36 and 11° for the CLF. 37 The test criterion for noninferiority was that the upper bound of 95% CI of the mean difference should be less than each noninferiority margin. This indicated that SEIB is “not inferior” to the US group. This criterion did not apply for the lower bound if 95% CI noninferiority was established. For noninferiority trials, per protocol is considered to be a more conservative analysis method than intention-to-treat analysis. 38 We conducted a primary per protocol analysis excluding participants in both groups who missed one or more assessment times. Secondary standard intention-to-treat analysis was conducted that included all participants in both groups who were originally randomly allocated regardless of the amount of treatment received. Secondary results are reported in the text where relevant.
To clarify the superiority between groups and reduce the risk of type I error,
39
we also used two-way mixed analysis of variance to identify the effects of treatment on PPT, VAS, and CLF with time (baseline and at 1, 2, 3, and 4 weeks) as an intrasubject variable and treatment type (SEIB or US) as an intersubject variable. Post hoc testing was conducted using the Tukey honest significant difference test for multiple comparisons. Within-group differences were compared at baseline and at 1, 2, 3, and 4 weeks. In addition, the effect size (ES) was calculated to examine the magnitude of therapeutic effect. The ES was defined in the following equation, wherein SD represents standard deviation:
40
The cutoff points of ES were 0.2, 0.49, and 0.8, considered as small, medium, and large, respectively. 41 For superiority testing, we chose intention-to-treat analysis to avoid overoptimistic estimation of the therapeutic effects of intervention by noncompliers. 42 All statistical analyses were performed by using the Statistical Package for the Social Sciences (SPSS, version 21.0, IBM, Chicago, IL). The level of significance was set at 0.05.
Results
Overall, 59 participants were evaluated to verify eligibility for this study. Finally, 45 participants satisfied the inclusion/exclusion criteria and were randomly allocated into the SEIB or US groups. Reasons for ineligibility included other treatment (n = 6), history of neck surgery (n = 2), and refusal (n = 6). Thus, a total of 45 participants (23 in the SEIB group and 22 in the US group) were analyzed (Fig. 2). The two groups did not differ in terms of demographic characteristics or MMSE-K and SF-36 scores at baseline (Table 1).
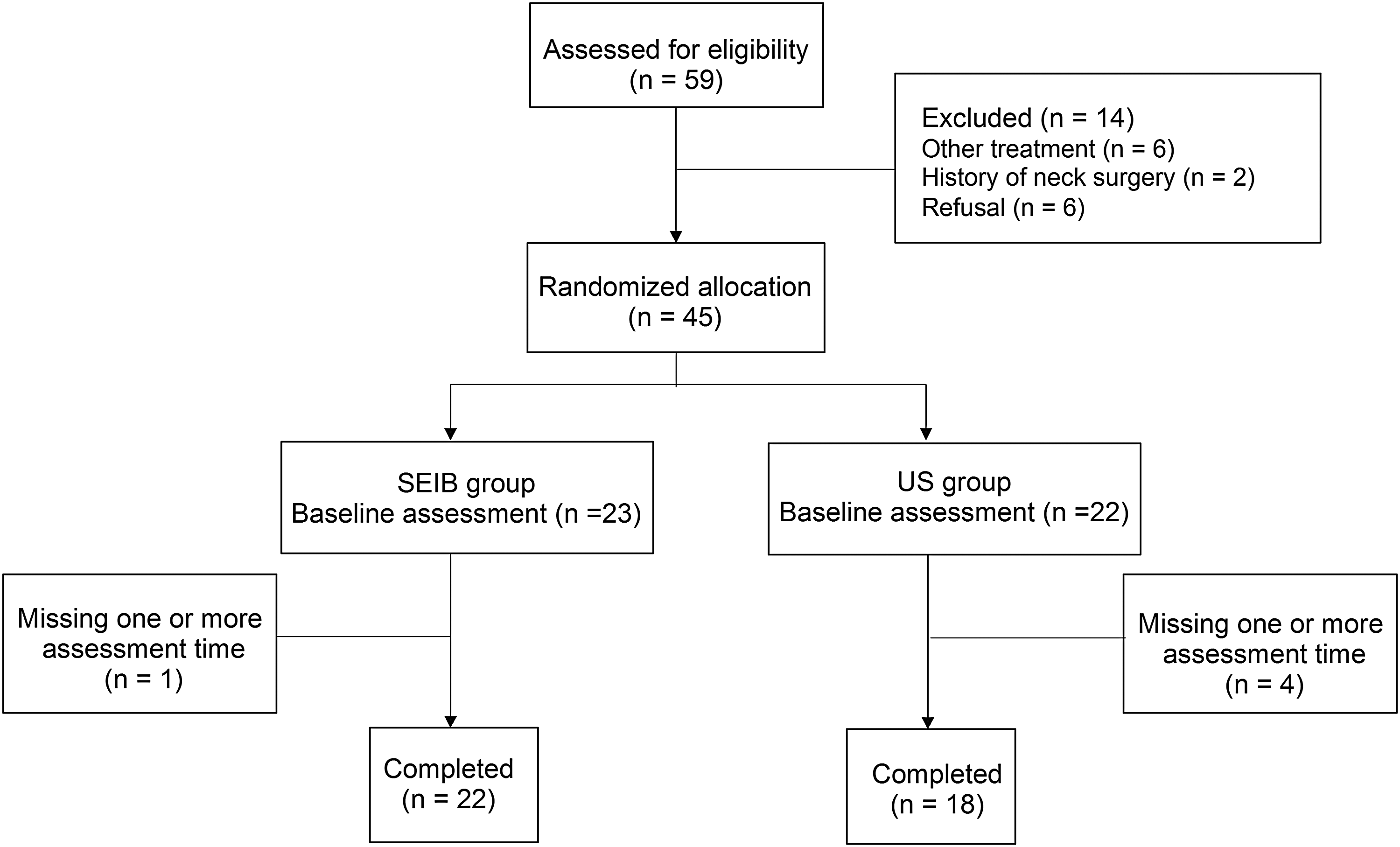
Consolidated Standards of Reporting Trials flowchart of the study and participants. US, ultrasound.
Unless otherwise noted, values are indicated as the mean ± standard deviation.
US, ultrasound; SEIB, self-exercise with a therapeutic inflatable ball; MMSE-K, Mini-Mental State Examination-Korean version; SF, short form; PCS, physical component score; MCS, mental component score.
According to the per protocol results, the VAS, PPT, and CLF showed that the upper bound of the 95% CI of the mean difference between groups did not exceed the noninferiority margin over 4 weeks, which satisfied the noninferiority criterion. For baseline and at 1, 2, 3, and 4 weeks, respectively, the 95% CI values of the mean difference are displayed in Figure 3. Intention-to-treat results also satisfied the noninferiority criterion.
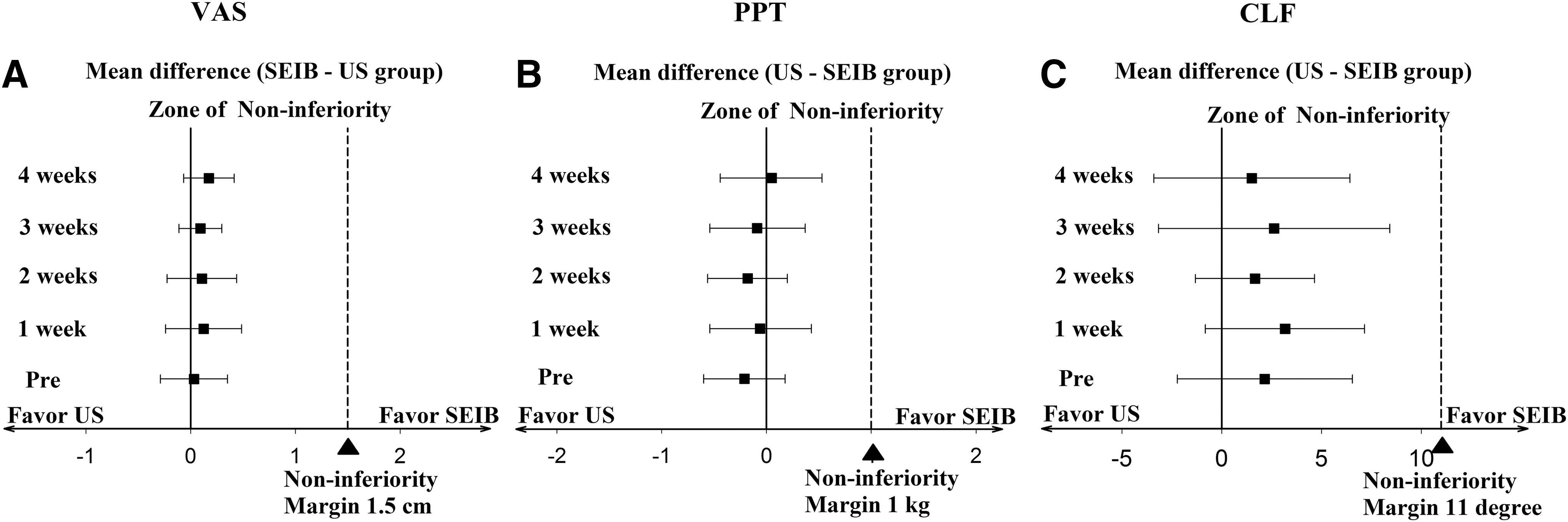
Schematic showing 95% confidence interval of mean difference between groups and noninferiority margin.
The two-way mixed analysis of variance showed no significant differences between the SEIB and US groups in the VAS (F = 2.579; p = 0.117), the PPT (F = 0.245; p = 0.624), and the CLF (F = 2.072; p = 0.159) (Table 2). No clinical outcomes showed a significant group-by-time interaction.
Unless otherwise noted, values are indicated as the mean ± standard deviation.
Significant within-group difference between baseline and 1, 2, 3, and 4 weeks in each group.
VAS, visual analogue scale; PPT, pain pressure threshold; CLF, cervical lateral flexion.
Both groups showed significant intragroup differences in all variables during treatment (p < 0.05). The VAS in both group significantly decreased at 1, 2, 3, and 4 weeks compared with baseline values. The PPT significantly increased at 3 and 4 weeks in the SEIB group and at 4 weeks in the US group. The CLF in both groups showed a significant increase at 4 weeks (Table 2). The ES in both groups showed a large decrease in VAS, and a large increase in CLF, at the end of the treatment period. The SEIB group showed a large increase in PPT, while the US group showed a moderate increase (Table 3).
Values are indicated as the effect size.
Discussion
This study is the first randomized, controlled noninferiority trial to demonstrate that SEIB can be as effective as US therapy for treating MTrPs in elderly patients with myofascial pain syndrome. Our main finding was that SEIB is noninferior to US therapy in all outcomes. Moreover, intragroup differences showed increased PPT, decreased VAS, and increased CLF compared with baseline in each group.
Most participants in the current study were elderly women, although no restriction was placed on recruitment for myofascial pain syndrome in the elderly. It has been speculated that women had greater prevalence of musculoskeletal pain than men. 43 No side effects or uncomfortable events occurred in either group during four consecutive intervention periods. To minimize the effects of ischemic compression by the pressure algometer on extensibility of soft tissue, CLF was measured first.
In noninferiority testing, 95% CIs for the mean differences in the VAS, PPT, and CLF were within noninferiority margins. This indicated that SEIB is noninferior to US therapy for reducing pain, decreasing pressure sensitivity, and increasing joint flexibility. Although previous studies showed that self-treatment, such as stretching 44,45 or use of a foam roll, 46 combined with conventional therapy, is more effective than single-component therapy for treating MTrPs, they did not directly evaluate the effectiveness of self-treatment. Thus, there was insufficient evidence to recommend self-treatment, which is a highly accessible and low-cost approach for treating MTrPs. However, the results of noninferiority testing in the current study supported the recommendation of SEIB as a therapeutic method for elderly patients with myofascial pain syndrome.
During the 4-week treatment period, the SEIB group showed remarkable changes and large therapeutic effects in the PPT, CLF, and VAS. The SEIB group showed an increase of 30% in the PPT and a large therapeutic effect at 4 weeks that was greater than the therapeutic effect of self-stretching but less than that of trigger-point manual therapy combined with self-stretching, with the respective techniques increasing PPT by 14% and 57%. 44 The SEIB group showed an increase of 32% in CLF and a large therapeutic effect at 4 weeks, which was greater than the 17% increase by ischemic compression of MTrPs in the neck and shoulder muscles after 4 weeks. 47 In particular, SEIB showed the largest increase of 46% and a large therapeutic effect in the VAS at 4 weeks, similar to that for dry needling, which increased the VAS by 50% for MTrPs in the lower trapezius. 48 Thus, although the mean differences for all clinical outcomes between the US and SEIB groups were too small to permit conclusions about clinical significance, SEIB showed clinical relevance for desensitizing MTrPs.
In addition, the therapeutic effects of SEIB in the current study concur with previous self-myofascial release studies, which reported decreased pain intensity and increased flexibility of soft tissue. 15,49,50 However, these demonstrated immediate effects with a single application in healthy adults and did not determine the therapeutic effect on specific pathologic sites, such as MTrPs. The results of the current study could provide further evidence that self-exercise for myofascial release is an effective technique.
Additionally, by repetitive measurements of VAS, PPT, and CLF, we identified the characteristics of the recovery process for MTrPs. In the SEIB group, the first significant recovery was observed in VAS scores at 1 weeks, then in the PPT at 3 weeks, and finally in the CLF at 4 weeks, as compared with the baseline values. These trends of the recovery process were similar to those in the US group. Previous studies also showed a similar recovery process. Dry needling and acupuncture significantly decreased the VAS at 1 and 2 weeks, which is an early stage, but did not affect PPT and joint flexibility. 51,52 Massage reduced the VAS at 1 day and 3 weeks, while joint flexibility increased at 3 weeks. 53 These results indicate that diminished pain is followed by recovery of joint flexibility in the recovery process for MTrPs. These results should also help clinicians understand the recovery stages in elderly patients with myofascial pain syndrome.
These findings may have resulted from sustained, tailored pressure and skin stretch applied to an area with the therapeutic inflatable ball. Such mechanical stimulation can elicit the excitation of mechanoreceptors and fusimotor neurons, potentially leading to changes in local fluid dynamics and tissue viscosity. 15,54 Furthermore, in the first stage of the SEIB technique, gentle rubbing with a circular motion may have released the pressure on the nerve and increased the lymph flow by stimulating superficial lymph nodes. 55 However, further physiologic studies are necessary to identify the precise mechanisms underlying the effects of SEIB.
Although this study identified changes in clinical outcomes, the intervention period was too short to demonstrate group differences, and there was no follow-up. Another limitation is the small sample size and sex imbalance. Although there was no restriction on sex in the process of recruiting participants, most participants were women. Thus, the results can be limited to elderly women with myofascial pain syndrome. In addition, the study included no treatment control group because of ethical concerns. However, because self-myofascial release is a highly accessible intervention that can be performed daily, the therapeutic effect of SEIB can be expected to be maintained by habitual application. Further long-term studies are necessary to investigate the therapeutic effect of home-based SEIB, with development of its applications.
Conclusion
The current study revealed that SEIB is as effective as US therapy for reducing pain, desensitizing MTrPs, and increasing joint flexibility. These findings provided clinical evidence that SEIB can be recommended as a safe, highly accessible, and low-cost self-treatment method for elderly patients with myofascial pain syndrome. For popularization of SEIB, further long-term studies are necessary to investigate therapeutic effects and its persistence of home-based SEIB.
Footnotes
Acknowledgments
This research was supported by a Korea University Institute of Health Sciences Grant, (K1508331). The authors would like to thank all the participants who volunteered for this study.
Author Disclosure Statement
No competing financial relationships exist.