
Abstract
Objective:
To investigate the acute effect of a t'ai chi chuan session on blood pressure and heart rate in patients with peripheral artery disease (PAD).
Design:
Randomized crossover intervention study.
Setting:
Outpatient therapy center.
Participants:
Seven patients with PAD, aged 50–79 years, not using β-blockers, calcium-channel blockers, or nondihidropiridinic vasodilators.
Intervention:
T'ai chi chuan and control session (both sessions lasted 40 minutes).
Outcome measures:
Systolic and diastolic blood pressure and heart rate, which were evaluated before and after the intervention (10, 30, and 50 minutes).
Results:
T'ai chi chuan exercise acutely decreased systolic blood pressure at 30 minutes after exercise (p = 0.042) and increased diastolic blood pressure at 50 minutes after exercise (p = 0.041). Heart rate did not change after t'ai chi chuan exercise.
Conclusion:
T'ai chi chuan acutely decreases systolic blood pressure in patients with PAD.
Introduction
P
Hypertension is highly prevalent in patients with PAD. 9 Moreover, the risk for cardiovascular events in patients with PAD is 30% higher than in patients with other atherosclerotic diseases, such as coronary heart disease and cerebral arterial disease. 10 Consequently, strategies to control cardiovascular risk factors, especially the reduction in blood pressure (BP), have been recommended as a target in the therapeutic approach of these patients. 1,11
Previous studies have shown that both walking and resistance exercises have promoted lowering BP in patients with PAD until an hour after exercise. 12 –15 However, because walking and resistance exercises promote pain symptoms, considered a main barrier for physical activity practice in patients with PAD, 16,17 alternative exercise strategies to reduce cardiovascular risk without symptoms must be studied.
T'ai chi chuan (TCC) is a traditional Chinese martial art that has been practiced in China for many centuries. It combines deep diaphragmatic breathing and relaxation with many fundamental postures that flow imperceptibly and smoothly from one to the other through slow, gentle, graceful movements. 18 TCC is practiced to promote good health, memory, concentration, digestion, balance, and flexibility. Moreover, it is also thought to improve psychological conditions, such as anxiety and depression. 19 In addition, a systematic review has found that TCC is effective in lowering BP after a training period in hypertensive patients and those with cardiovascular disease. 20 However, whether TCC decreases BP and heart rate (HR) in patients with PAD, who have endothelial dysfunction, 21 increased arterial stiffness, 22 and increased cardiac sympathetic modulation to the heart, 23 is unknown.
Because previous studies have demonstrated that a single exercise session can predict the chronic response of exercise training, 24,25 the aim of this study was to investigate the acute effect after a single TCC session on BP and HR in patients with PAD.
Materials and Methods
Participants
Patients with PAD were recruited at public hospitals and private clinics in Recife, Pernambuco, Brazil. Patients were screened by a physician and were included if they (1) were aged 50 years or older; (2) had claudication symptoms; (3) had an ankle brachial index of 0.90 or less; (4) had systolic and diastolic BP lower than 160 mmHg and 105 mmHg, respectively; (5) had not undergone coronary artery bypass surgery or angioplasty in the last year; (6) were not using β-blockers, calcium-channel blockers, or nondihidropiridinic vasodilators; (7) did not present complex arrhythmias or myocardial ischemia; and (8) did not have amputated limbs. Information regarding the self-reported stress was also obtained. Seven patients were included in this study and signed a written consent form. This study was approved by the Research Ethics Committee of the University of the Pernambuco, Brazil (#0265.0.097.000-10).
Procedures
All patients underwent two experimental sessions (control and TCC session) conducted in random order and separated by at least 72 hours. Sessions were started between 7 am and 8 am; patients were instructed to have a light meal at least 2 hours before arriving at the laboratory and not to ingest coffee, tea, cola, or other stimulants thereafter. In addition, they were instructed to refrain from vigorous physical activity in the previous 48 hours and from alcohol ingestion in the previous 24 hours. Smokers were instructed not to smoke before testing sessions, and all patients continued to take their regular medication on experimental days.
In each experimental session, patients arrived at the laboratory and initially rested in a seated position for 20 minutes. After this period, BP and HR were obtained (preintervention period). BP and HR measurements were taken with the automatic digital Microlife device (Widnau, Switzerland), BP 3AC1-1 model, validated according to the British Association of Cardiology specifications for measurements taken at rest; 26 all measurements were taken by the same researcher. The mean value of the three measurements was considered to establish values at preintervention period. After this period, patients started the control or TCC intervention.
The TCC intervention started with a specific warm-up with the first part of the lian gong shi ba fa technique (5 minutes). After warm-up, patients performed postural movements, as ma-pu (rider posture), kun-ma (bow and arrow posture), and leg false posture. At the end, they performed movements with arms and yang simplified position (Pequim 24). The complete session lasted 40 minutes. All movements were carried out according to the guidelines and were supervised by an experienced TCC instructor. In the control condition, patients remained in a seated position for 40 minutes.
Thereafter, patients returned to the resting seated position for 60 minutes (postintervention period). BP and HR were obtained at 10, 30, and 50 minutes, respectively. For analysis, Δ values were considered (postintervention – preintervention values).
Statistical analysis
Normality of the data was not confirmed by the Shapiro-Wilk test, and nonparametric analysis were performed. The Friedman test was used to analyze the variables within each group. When significant differences were found between the values analyzed, comparisons were made of the paired data between each of two measurements (Wilcoxon test), penalizing the p-values found by the Bonferroni procedure. The Wilcoxon statistical test was used for comparisons between sessions in each time deemed. Data are presented as median and interquartile range (IQR; 25th–75th percentile values). Significance was set at p < 0.05.
Results
Table 1 shows the general characteristics of participants in this study.
Data are presented as median (interquartile range) or frequency.
The preintervention systolic BP values were similar between sessions (control: median, 122 mmHg [IQR, 22 mmHg]; TCC: median, 119 mmHg [IQR, 20 mmHg]; p = 0.249). The TCC session decreased systolic BP at 30 minutes after the intervention (p = 0.042) (Fig. 1).
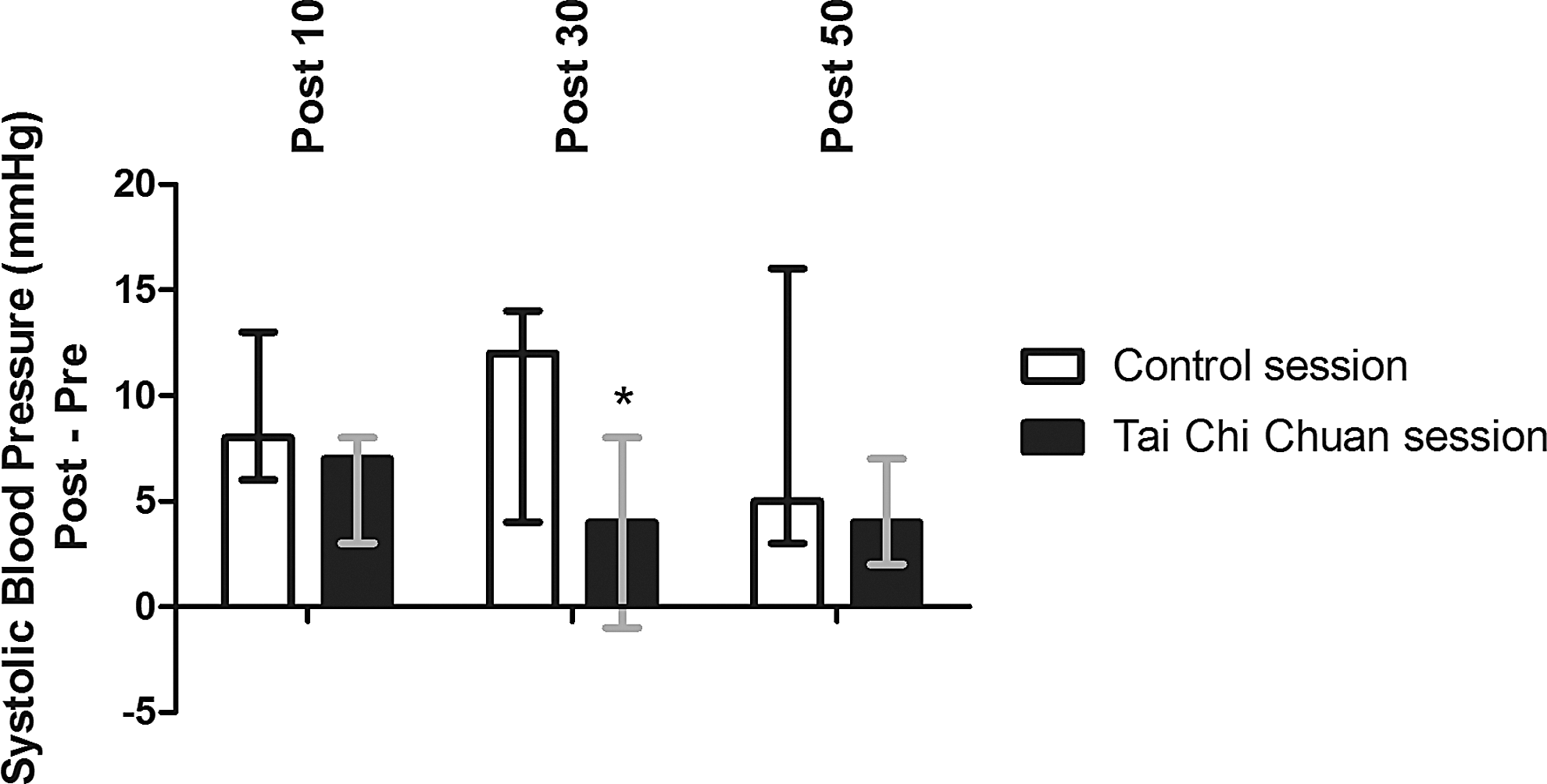
Postintervention acute response of systolic blood pressure. The values are presented as median and interquartile range. *p < 0.05 between sessions.
The preintervention diastolic BP values were similar between sessions (control: median, 74 mmHg [IQR, 12 mmHg]; TCC: median, 73 mmHg [IQR, 8 mmHg]; p = 0.063). TCC session increased diastolic BP at 50 minutes after the intervention (p = 0.041) (Fig. 2).
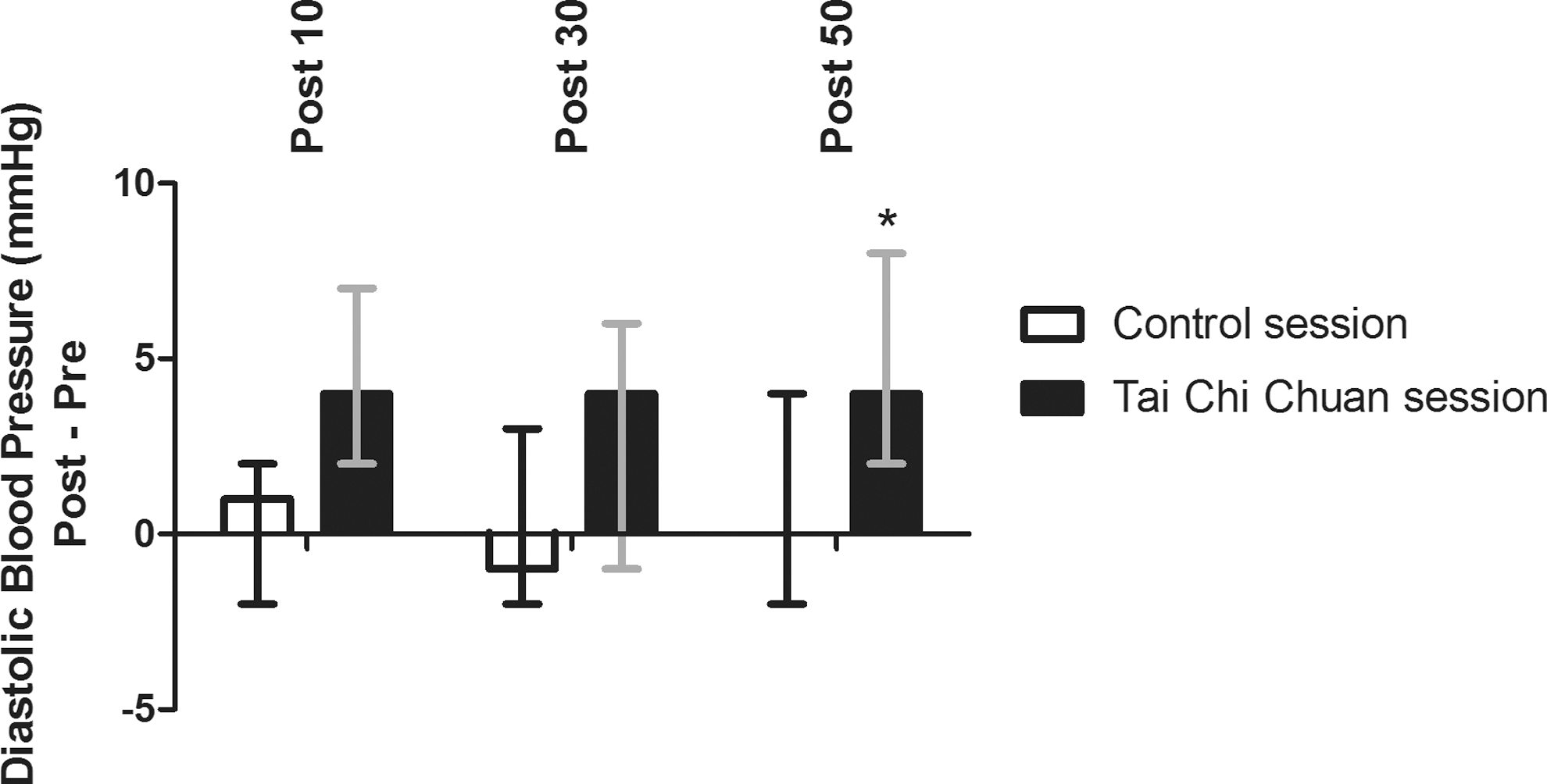
Postintervention acute response of diastolic blood pressure. The values are presented as median and interquartile range. *p < 0.05 between sessions.
The preintervention HR values were similar between protocols (control: median, 79 beats/min [IQR, 15 beats/min]; TCC: median, 79 beats/min [IQR, 18 beats/min]; p = 0.865). There were no significant changes in HR after the intervention (Fig. 3).
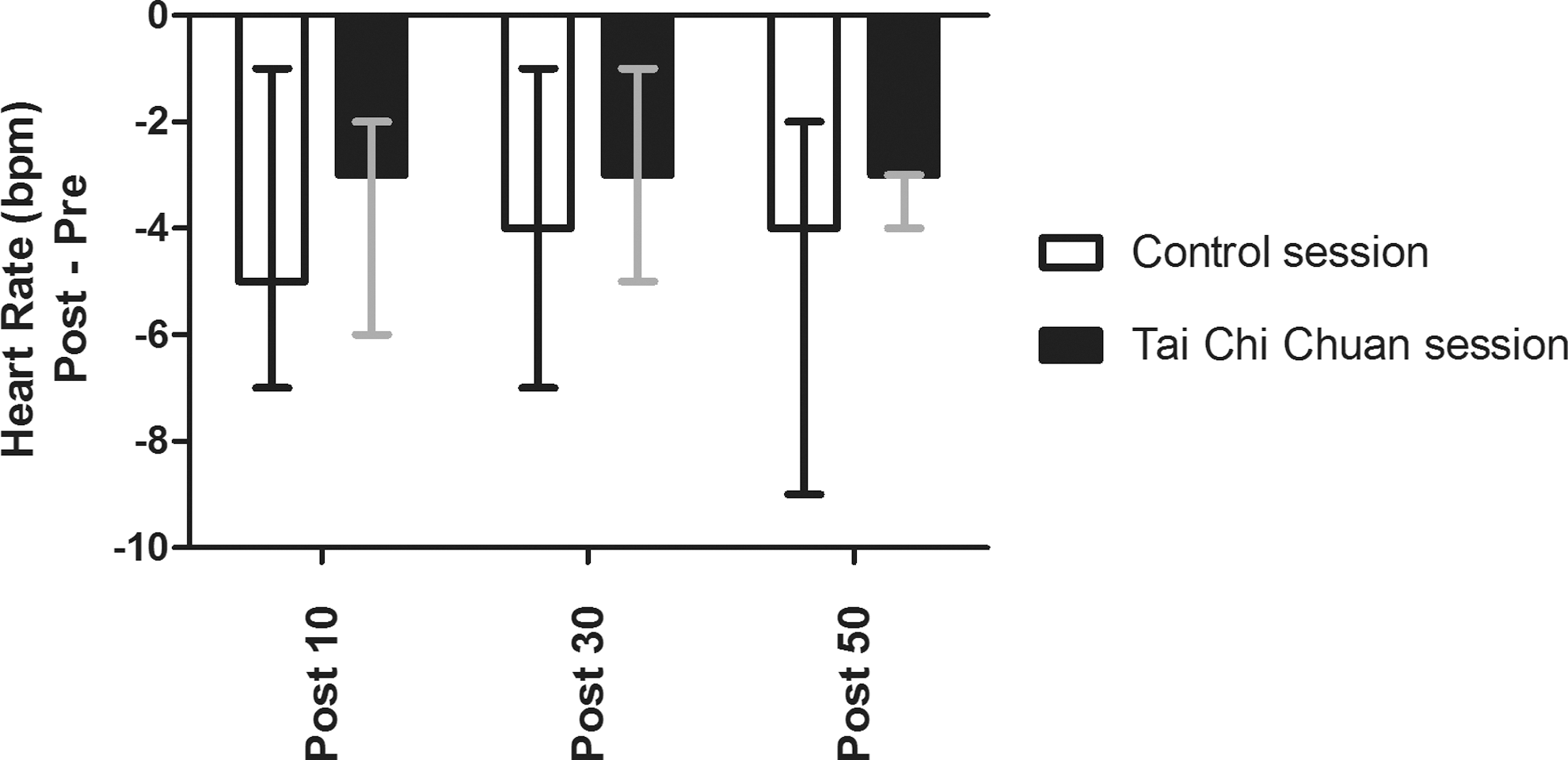
Postintervention acute response of heart rate. The values are presented as median and interquartile range.
Discussion
The results of this study indicated that a single session of TCC exercise decreases systolic BP and did not change HR in a recovery period, suggesting that TCC could be incorporated as an alternative exercise strategy to reduce acute cardiovascular load in patients with PAD.
This is the first study to analyze the acute cardiovascular effects of TCC exercise in patients with PAD. The results showed that TCC decreased systolic BP at 10, 30, and 50 minutes after exercise, although statistical significance was reached only at 30 minutes after exercise. The net reductions of systolic BP calculated by ([post-TCC − pre-TCC] − [post-control − pre-control]) were −7.4 ± 7.3 mmHg. This magnitude of reduction was similar to those observed after resistance and walking exercises in these patients. 12 Furthermore, it is known that reductions of about 5 mmHg in BP decrease mortality from coronary heart disease in 9% and stroke in 14%. 27 Thus, the magnitude of reduction in systolic BP obtained by TCC can be considered clinically relevant for these patients.
In the present study, TCC session increased diastolic BP at 50 minutes. Given that systolic BP is mainly influenced by cardiac output, whereas diastolic BP is mainly influenced by peripheral vascular resistance, the increases in systemic vascular resistance may have occurred to compensate for the decreases in cardiac output. The divergent responses between systolic and diastolic BP has already been observed in other types of exercise and different populations 28 –31 and may reflect the orthostatic stress produced by the prolonged time in a sitting position. 30 These responses are probably potentiated in patients with PAD evaluated in this study because these patients are known to have endothelial dysfunction and increased arterial stiffness. 21,22 Future studies should examine the effects of TCC session in systemic vascular resistance, arterial stiffness, and endothelial function in order to clarify the mechanisms involved in the increased diastolic BP after a TCC session.
Previous studies have frequently demonstrated an increase in HR during the recovery period after different modalities of exercise, 29,32 promoted by the increase in sympathetic modulation to the heart. 33 Interestingly, our results indicated maintenance of this variable after a TCC exercise session. A decrease in HR in favor of TCC session was probably not evidenced because of the small sample size. In fact, previous studies have found that a TCC session can alter cardiac autonomic modulation by enhancing the parasympathetic and reducing the sympathetic modulation, consequently reducing the HR in adults. 34
Hypertension is highly prevalent in patients with PAD, 9 and exercise is recommended for the control of cardiovascular risk factors. 1 This study amplifies the current knowledge showing acute benefits on BP in PAD. However, it would be clinically significant if this reduction were also observed over the long term. Some studies in hypertensive and patients with coronary artery disease showed that TCC exercise training decreased BP during a long-term period. Channer et al. 35 showed that an 8-week, low-intensity TCC program was effective for reducing BP in patients with acute myocardial infarction. Lai et al. 36 studied 2-year trends in cardiovascular function among elderly TCC practitioners and sedentary participants and found that regular TCC might delay the decline of cardiovascular function in elderly persons. Thus, the long-term effects of TCC on cardiovascular risk in patient with PAD must be investigated in the future.
This study had some important limitations. First, the statistical power was compromised by the small sample size. Second, patients receiving β-blockers, calcium-channel blockers, or nondihidropiridinic vasodilators were not included in this study, which precludes the applicability of the results to patients receiving these medications. Patients in this study had systolic and diastolic BP lower than 160 mmHg and 105 mmHg, respectively. Thus, the results cannot be extrapolated to patients with PAD at other stages of hypertension. Finally, ambulatory BP monitoring was not included, and it is not possible to state that the reduction in systolic BP observed in this study after TCC exercise would be prorogated during patients' daily activities.
In conclusion, a TCC session promotes a decrease in systolic BP and maintenance of HR after exercise. Thus, TCC could be incorporated as an alternative exercise strategy to reduce acute cardiovascular load in patients with PAD. However, future studies are needed to understand the mechanisms involved in these responses.
Footnotes
Acknowledgments
The authors are thankful for the support provided by public hospitals and private clinics in the city of Recife and the National Counsel of Technological and Scientific Development, and for a grant from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).
Author Disclosure Statement
No competing financial relationships exist.