
Abstract
Objectives:
Nearly 9 million Americans use prescription sleep aids to induce or maintain sleep; however, the long-term effects of these medications are unknown. Considering the number of individuals reporting insufficient sleep, nonpharmacologic methods for improving sleep are needed.
Design:
A systematic review of published studies was conducted to determine the efficacy of nutritional intake as a modality for improving sleep behavior. Inclusion criteria for the review were interventions (both in vivo and in natura), using any quantitative design, employing a dietary intervention as the primary treatment variable, targeting sleep behavior, in nonclinical human populations age 18–50 years.
Results:
A total of 21 studies (17 in vivo and 4 in natura) met the inclusion criteria and were included in the systematic review.
Conclusions:
The evidence for nutrition as treatment modality for improving sleep is mixed. Nearly half of the in vivo trials suggested a significant change in a primary sleep variable of interest. However, a majority of these trials relied on small sample sizes of healthy sleepers and manipulated nutrition in an acute fashion. Among the in natura studies, macronutrient composition appeared to have no effect. However, the small number of studies mainly recruited healthy sleepers, and most had limited control of the diet of participants.
Introduction
A
Prescription sleep aids are a common treatment options for troubles initiating and/or maintaining sleep. 19 The Centers for Disease Control and Prevention estimates 4% of the adult population (9 million people) use prescription sleep aids. 19 However, long-term use of sleep aids has been linked to adverse outcomes in health, 20 and much is unknown about the safety and effectiveness of prescription sleep aids over the long term. Other nonpharmacologic treatment options include cognitive-behavioral therapy, 21 mindfulness, 22 sleep hygiene/psychoeducation, 23 herbal extracts, 24 and physical activity. 25 Nutritional interventions are a potential alternative and complementary treatment for improving sleep. 26 Dietary precursors have been hypothesized to influence neurotransmitters, such as serotonin, involved in the sleep-wake cycle. 27 However, the efficacy of nutrition for improving sleep is relatively unexplored. Thus, the purpose of this study was to evaluate dietary interventions targeting sleep behavior in humans age 18–50 years conducted between January 1965 and August 2015 (50 years).
Materials and Methods
Criteria for including studies in this review were (1) interventions (both in vivo and in natura), (2) use of any quantitative design, (3) use of a dietary intervention as the primary treatment variable, (4) targeting of sleep behavior in humans, and (5) recruitment of a nonclinical, adult population age 18–50 years. Literature searches were delimited to: peer-reviewed articles that were published between January 1965 and August 2015 (50 years) in English and were indexed in MEDLINE, the Cochrane Library (CENTRAL), and Web of Science (WOS) electronic databases. 28 Free text and the Medical Subjects Headings terms “meal,” “food,” “nutrition,” “diet,” “carbohydrate,” “protein,” “fat,” and “sleep*” were applied to conduct the systematic search in the selected databases.
Interventions satisfying the inclusion criteria were subjected to a methodological critique using a modified augmented version of the Jadad scale, 29 developed by Sarris and Byrne. 30 Their scale provided a total quality score ranging from 0 to 10, with higher scores indicating a higher level of methodological quality. 30 Methodological factors assessed by the scale included randomization, blinding, withdrawals, exclusion criteria, intervention used, control used, and data reporting. 30 For reviewed studies applying parallel designs, the modified version of the scale developed by Sarris and Byrne was applied. For reviewed studies applying crossover designs, two items from the modified scale were revised to account for differences between design types. Scale scores were based on information reported in the reviewed articles. Table 1 presents an overview of the quality assessment scoring system applied in this study. Figure 1 illustrates the data extraction process.
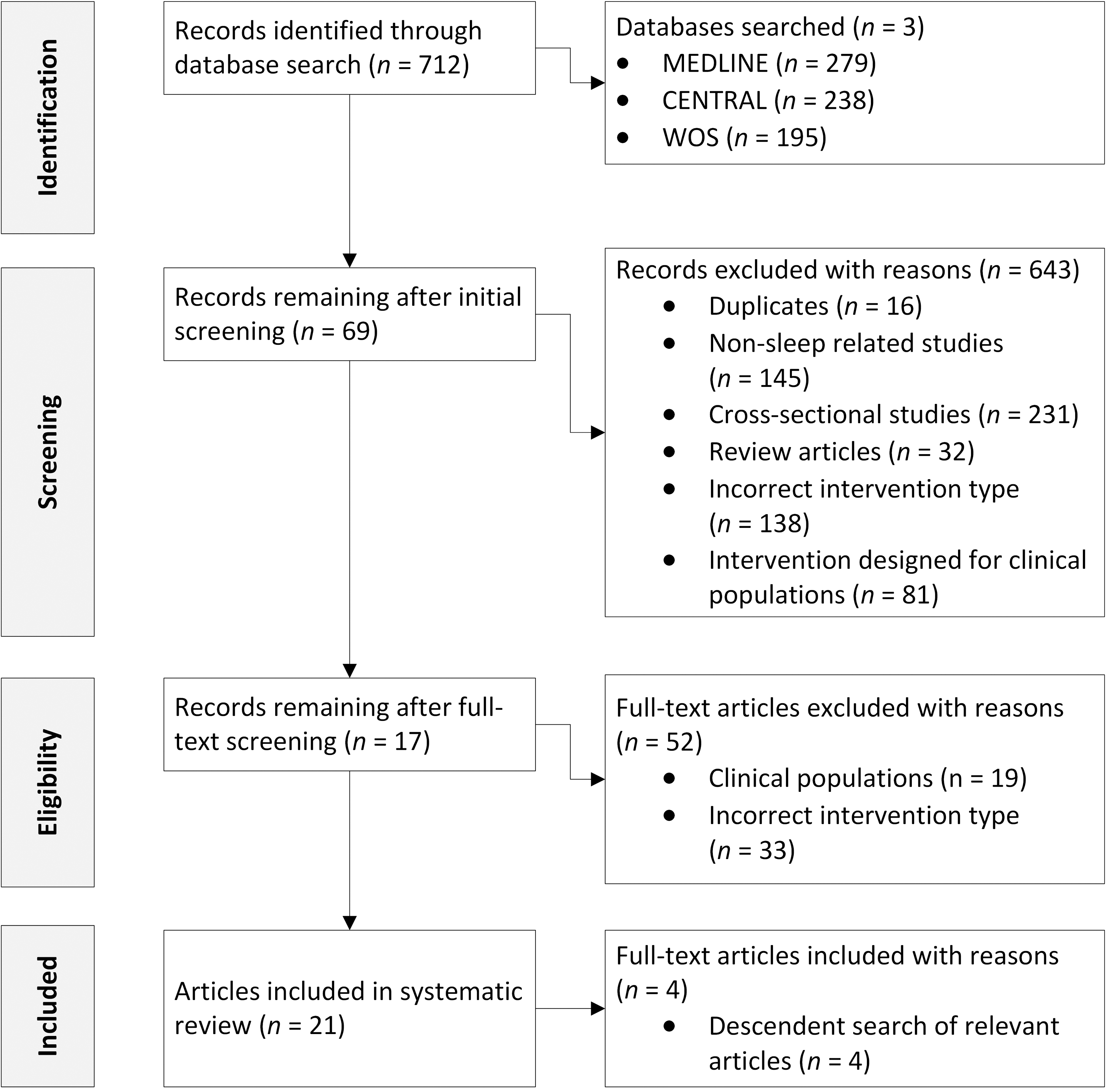
Flow diagram of the data extraction process. CENTRAL, Cochrane Library; WOS, Web of Science.
Yes = 1 point; no = 0 point; total/10. 29
P, item applied to parallel designs; C, item applied to crossover designs.
As no human subjects were involved, this study did not require institutional review board approval.
Results
The search strategy returned 712 hits from the MEDLINE (n = 279), CENTRAL (n = 238), and WOS (n = 195) databases. Initial screening removed duplicates (n = 16), irrelevant studies (n = 145), cross-sectional studies exploring sleep and nutrition (n = 231), review articles (n = 32), studies that did not test the intervention effect of nutrition on sleep (n = 138), and interventions designed for clinical populations (n = 81). Full text of the parsed list of articles was assessed for eligibility, removing studies that targeted clinical populations (n = 19) and further removal of studies that did not test the intervention effect of nutrition on sleep (n = 33). Next, a descendent search was conducted on the eligible studies. An additional 4 studies were identified through this process and included in the final tally of reviewed articles. In total, 21 studies were included in the systematic review. Figure 1 illustrates the data extraction process applying Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Table 2 provides descriptive results of the included studies.
CHO, carbohydrate; Tx, treatment group; Cnt, control or comparison group; FAT, fat; PRO, protein; EEG, electroencephalography; REM, rapid eye movement; PSG, polysomnography; Ex, experiment; NREM, non-rapid eye movement sleep; BMI, body mass index; EOG, electro-oculography; A-LAC, α-lactalbumin; Trp:LNAA, ratio of plasma tryptophan to large neutral amino acids; GI, glycemic index; VL CHO, very low carbohydrate; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid.
Discussion
The purpose of this study was to evaluate dietary interventions targeting sleep behavior in humans. Sleep is a significant health issue, 31 yet only 21 interventions meeting inclusion criteria were identified during a 50-year time span. Furthermore, most interventions were conducted in the United Kingdom, 32 –37 United States, 38 –41 and Sweden. 42 –44 Given that inadequate sleep is a health problem found around the world, 31 along with the limited interventions that have been conducted, it would be advantageous to implement more interventions from a variety of cultural contexts. The results of the data extraction suggest that interventions targeting diet for improving sleep primarily fell into two categories: A total of 17 in vivo (“within the living”/laboratory, strictly controlled) interventions 32 –39,43 –51 and a total of 4 in natura (“in nature”/nonlaboratory, free-living) interventions. 40 –42,52
In vivo trials
Of the 17 in vivo trials, 8 (47%) suggested improvement in at least one primary outcome of interest. 32,38,39,47 –51 Of interventions producing significant effects, 4 applied mixed composition meals, 32,38,39,51 2 focused on manipulating carbohydrates, 49,50 and 2 focused on manipulating protein. 47,48 The studies reviewed in this paper suggest that mixed-composition meals decrease time in slow-wave sleep, 32,51 a solid meal shortens sleep latency relative to a liquid meal, and a mixed meal consumed at midday increases postprandial sleep time. 38 In terms of carbohydrates, the limited evidence from this review suggests that a high-glycemic index meal may decrease sleep-onset latency when consumed 4 hours before bed, 49 while a very-low-carbohydrate meal may increase time spent in slow-wave sleep and decrease time in rapid eye movement sleep. 50 Evidence from the protein-focused studies reviewed in this paper suggests that protein source tryptophan combined with carbohydrates improves sleep in insomniacs 47 and tryptophan-rich meals consumed before bed increase morning alertness. 48
Most in vivo trials strictly controlled the timing of the experimental meals to determine their potential effect on sleep. This design feature assists in isolating direct effect of nutritional intake upon sleep. Polysomnography, the gold standard in evaluating sleep, was used in 9 of the in vivo studies. 34,36 –39,45,49 –51 Using rigorous measurement substantiates findings of intervention effects. A possible limitation of in vivo trials was the heavy reliance on crossover designs in most studies (n = 15). 32 –37,39,43 –46,48 –51 Crossover designs entail each participant receiving all treatments of the intervention, as well as acting as their own control. A benefit of this approach is that fewer participants need to be recruited in order to test a variety of intervention protocols. A drawback of this method is that an adequate washout period between treatments is required to prevent carryover effects. 53 For dietary interventions, a 2-week washout period is often recommended. 54 At least 3 interventions met this benchmark. 32,46,48 Future interventions should detail washout periods to rule out contamination. All but 2 of the dietary interventions relied on macronutrient manipulation of diet to improve sleep. 45,46 Other mechanisms by which nutrition may affect sleep, such as chrononutrition, the thermic effect of food, intestinal peptides, and nucleotides, remain relatively unexplored. 26
Most of the studies relied on small samples sizes. Sample sizes from studies using crossover designs ranged from 6 to 28 participants. The study by Zammit et al. used a static-group comparison post-test-only design comprising 21 participants, while Hudson and colleagues' randomized controlled trial recruited 57 participants. 47 Most of the in vivo studies recruited healthy sleepers (e.g., obtaining adequate sleep with no history of sleep problems). 32 –39,43 –46,48 –51 Such an approach is understandable for in vivo trials because the goal of such studies is to understand mechanisms regulating nutrition on sleep. The drawback of such an approach is that the treatment potential of nutrition in those not meeting sleep guidelines is unclear. The duration for most of the interventions (not counting washout and acclimation periods) was relatively short, ranging from 1 day, 39,43,49 2 days, 37,38,48,51 4 days, 44 –46 5 days, 50 6 days, 34 7 days, 33,47 8 days, 32 12 days, 35 to 2 weeks. 36 Subsequently, most interventions were limited to acute manipulation of nutrition. Habitual dietary intake may advance research seeking to identify dose-response relationships between nutrition and sleep.
Healthy samples coupled with acute nutritional experimentation, as well as small sample sizes, may minimize the intervention effect of nutrition on sleep. In contrast, Hudson and colleagues' in vivo intervention 47 was tested on participants with primary insomnia and found improvements in sleep outcomes. This particular study had a larger sample size (n = 57) to detect significant effects and was run for 1 week (not counting acclimation and measurement periods). Future researchers should develop similar studies that test chronic manipulation of diet on larger samples of unhealthy sleepers.
In natura trials
Of the 4 in natura trials, macronutrient composition appeared to have no effect. 40 –42,52 However, some markers of sleep, such as sleep fragmentation 40 and sleep latency, 40,41 did improve. Possible explanations for absence of significant findings include the relatively small effect of nutrition for improving sleep, recruitment of healthy sleepers, and the difficulty of controlling dietary treatments in a free-living environment. For example, the study by Nehme et al. 52 had little control over foods consumed outside of the work setting. Future in natura studies should consider recruiting participants with unhealthy sleep patterns. Lindseth and colleagues' study 40 was rigorous for a free-living intervention and may serve as a good study model for future research in this area. The researchers used a 2-week washout period between treatments, weighed foods consumed by participants, and required that participants consume all meals in a controlled environment. A possible limitation of this study was that although inclusion criteria required participants report sleep problems, baseline Pittsburgh Sleep Quality Index (PSQI) scores (mean ± standard deviation, 4.1 ± 1.9) indicate that the sample had good sleep quality (global PSQI score ≤5 indicates good sleep quality; PSQI score >5 indicates poor sleep quality). If effects of nutritional interventions are small, as is the case with most behavioral interventions, recruiting participants with good sleep may mask the potential of such interventions for improving sleep. Considering that the PSQI is a relatively standardized instrument, it may be advantageous to use this instrument as a screening tool for future free-living interventions. One advantage of the in natura studies was the use of actigraphy in most studies. 14,15,26 Sensor monitors are relatively noninvasive and provide objective sleep data and should be used in future free-living interventions. There has been a paucity of in natura studies, and there is clear need for more such interventions by future researchers.
Limitations
General limitations of nutritional interventions for sleep behavior include smaller samples, short duration of intervention period, recruitment of healthy sleepers, and absence of washout period information to rule out carryover effects between interventions. There are also limitations inherent to the systematic review methods applied in this study, which should be considered upon interpreting the findings of this report. Although the authors sought to identify all articles that met the inclusion criteria, searching was delimited to three databases: MEDLINE, CENTRAL, and WOS. Subsequently, some studies may not have been identified in the search process. Articles were included only if they were published in English, which may have prevented studies published in other languages from being included.
Conclusions
Sleep is critical to optimal health, yet an estimated 35.3% of U.S. adults receive insufficient sleep. 17 Alternative and complementary approaches are needed to combat the inadequate sleep epidemic. 55 This systematic review analyzed nutritional interventions as a potential modality for improving sleep behaviors. Theoretically, diet plays a role in synthesizing neurotransmitters involved in the sleep-wake cycle and should offer a treatment benefit. However, the role of nutrition as a treatment option for sleep has not been clearly demonstrated by intervention research. Nearly half of the in vivo studies reviewed showed improvement on at least one indicator of sleep, while the in natura studies were unable to do so. Several limitations, including paucity of studies, small sample sizes, acute manipulation of nutrition, difficulty in controlling diet, and recruitment of healthy sleepers, may partially explain the lack of results.
Footnotes
Acknowledgments
This work was performed in the offices of Drs. Adam P. Knowlden, Christine L. Hackman, and Manoj Sharma. No specific financial support was provided to conduct this research.
Authors' contributions: All three authors conducted independent searches for articles. A.P.K. conceptualized the study, developed the inclusion criteria, collected the data, developed the tables, analyzed the data, and wrote portions of the manuscript. C.L.H. analyzed the data, developed the tables, and wrote portions of the manuscript. M.S. critiqued the data, developed the tables, and reviewed the final manuscript.
Author Disclosure Statement
No competing financial interests exist.