
Abstract
Objectives:
Chinese medicine is a complex domain of theoretical and practical approaches that is being increasingly put under the research spotlight. The “Chinese Medicine in Australia” research project attempted to capture the clinical features of practitioners of Chinese medicine.
Participants and Interventions:
The project involved a national survey of Chinese medicine professional association members and registered practitioners in the state of Victoria, Australia (n = 655; response rate, 42%–55%) completed in 2012–2013.
Design:
The content and face validated survey was developed using new and previous workforce survey questions.
Results:
This paper reports on the workforce and practice characteristics of the survey respondents. Chinese medicine practitioners are highly educated, come from diverse backgrounds, and have chosen to practice predominantly in sole or multipractitioner private practice settings. An interest in the philosophy of Chinese medicine and previous experiences contributed to practitioners’ decisions to study and practice Chinese medicine. Incorporating a variety of techniques, practitioners describe themselves as practicing predominantly Chinese acupuncture and herbal medicine.
Conclusions:
The results from this survey contribute to the understanding of the nature and description of Chinese medicine practice in Australia.
Introduction
I
CM practice became regulated in the state of Victoria in 2000, making it the first jurisdiction outside China to introduce CM practitioner statutory regulation. This followed years of lobbying and the publication of “Towards a Safer Choice,” a report commissioned by the Victorian Department of Human Services, New South Wales Department of Health, and Queensland Department of Health. 6 In 2007 the establishment of the National Institute of Complementary Medicine followed from the recommendation in 2003 by the Expert Committee on Complementary Medicines in the Australian Health System that, in view of the high use of complementary medicines and therapies in the community, the government has a social responsibility to invest in research on complementary medicines. 7
In Australia, proprietary (manufactured) forms of CM herbal medicine supplies are regulated by the Therapeutic Goods Administration (TGA) in the interests of public health and safety. 8 Raw herbs, in contrast, are not regulated via the TGA. Instead, the Australian Customs and the Australian Quarantine and Inspection Services are the main government bodies that ensure prohibited substances (including materials from endangered species) and contaminated substances are not imported into Australia. The importation of raw Chinese herbs into Australia is mainly regulated via the Customs Act 1901 (and its associated regulations), the Wildlife Protection (Regulation of Exports and Imports) Act 1982, and the Quarantine Act 1908 (and its subordinate legislation). In Australia, registered Chinese herbal medicine (CHM) practitioners or CHM dispensers may not legally prescribe, manufacture or supply any substance which is in Schedules 2, 3, 4 or 8 of the Standard for the Uniform Scheduling of Medicines and Poisons.
Complementary medicines such as proprietary herbal formulas must be registered or listed on the Australian Register of Therapeutic Goods (ARTG) by the TGA with an AUSTL number. CHMs with a higher category of risk are registered on the ARTG with an AUSTR number. Manufactured medicines listed on the ARTG include ingredients that have been assessed as being eligible for use in a listed medicine. Manufacturers of listed products have the responsibility to conform to certain legal requirements, such as labeling under the Therapeutic Goods Act 1989.
Finally, having been in the education system for 30 years, CM is now a registered healthcare profession across Australia, under the Health Practitioner Regulation National Law, as in force in each state and territory (the National Law). With formalization of CM practice via statutory regulation, it is timely to investigate the nature of both the practice and the practitioners, in a manner that respects the perspectives and systems of thought of the discipline. The aim of this project was therefore to characterize the current clinical dynamics of Chinese medicine practice in Australia.
Materials and Methods
Survey
Despite limitations, surveys are useful tools for collecting data in highly characterized domains of human activity. The fact that they depend largely on self-reports and voluntary responses both aids and limits the research. In the present case, the method was chosen because of its inclusiveness, flexibility, convenience, and repeatability. Because this study was the first to attempt to rigorously characterize the CM practitioner population in Australia, a combination of both quantitative and qualitative approaches was incorporated.
The Chinese Medicine in Australia (CM in Australia) survey included questions modified from previous workforce surveys of Chinese medicine practitioners in Australia, with permission, and others developed specifically by the research team. 6,9 Content and face validation of the survey items were carried out with the assistance of six university academics, researchers, educators, and practitioners in Chinese medicine and other disciplines in Australia. On the basis of this feedback, the survey was submitted to the Monash University Human Research Ethics Committee (MUHREC) and ethics approval was received (approval number MUHREC CF10/3438: 2010001818). The survey was translated into Chinese to reach more practitioners and improve representativeness. The use of both English and Chinese languages followed the lead of the Chinese Medicine Registration Board of Victoria (CMRBV) workforce survey and publications at the time.
Invitations to complete the survey and reminders were distributed through email, newsletters, and links on members’ websites of the main professional associations: Australian Acupuncture and Chinese Medicine Association (AACMA), Federation of Chinese Medicine Associations, Australian Traditional Medicine Society, Australian Natural Therapists Association, and the CMRBV. The survey was offered using the online Qualtrics survey distribution and analysis software tool. Participants could also ask to have a paper copy of the survey and a reply envelope sent to them, in English or Chinese. It was expected that the use of email distribution and the online survey tool would improve the response rate by making it easier to invite participants and for them to complete the survey. Support from the distributing professional associations combined with assurances of confidentiality and anonymity for survey responders, as well the exclusion of sensitive questions (i.e., income), was also expected to improve the response rate. 10
Strenuous efforts were made to establish communication with the professional associations and the CMRBV through emails, phone contact, face-to-face meetings, personal connections, and networking at industry seminars and events. A presentation was made to the CMRBV, after which the project received the board's endorsement as well as their agreement to assist with the promotion and dissemination of the survey. The research aims were also presented at the Australian Chinese medicine conference, held in May 2011 by the AACMA, the largest CM professional association in Australia. These and other efforts were undertaken to increase awareness of the study and to encourage responses. It was widely considered that at the time of survey preparation and distribution, apprehensions had developed among practitioners regarding the upcoming national regulation. While a nominal target for the response rate was set at 30%, because the exact number of people practicing CM in Australia was unclear, and with a lack of structural accountability nationally, it was recognized that the ability to access the population was largely limited to the professional associations and CMRBV.
Other challenges included a protracted time required to undertake content validation, the logistics associated with translation and validation of the Chinese version of the survey, and the time and energy required to promote and distribute the survey, which itself necessitated repeat mailings and reminders, presentations at seminars, distribution of copies through industry bookstores, and a hard-copy mailings to the 1179 registered practitioners on the CMRBV database. This effort improved the response rate and was therefore well worth it.
According to the Australian Bureau of Statistics, there were around 1500 CM practitioners in Australia in 2006. 4 AACMA reported having 1560 practicing CM members in 2011. 11 The present survey provides an accurate and complete description of the CM workforce immediately before the introduction of national registration. This initial analysis will enable this survey to be applied as a longitudinal tool to help further refine the understanding of the clinical practice and of CM practitioners in Australia over time, as well to as to contribute to the ongoing development of the CM workforce.
Statistical analysis
Because this is a baseline survey of the CM primary practitioner population in Australia, descriptive statistics were analyzed using SPSS.21 and Excel in Microsoft Office Professional Plus 2010. In particular, frequencies and percentages, including means and standard deviations, were obtained from the quantitative data. Qualitative data found in the “other” section of questions were open-coded using key words and quantified using Excel software, an acceptable method of analysis for some qualitative data. 12 Most of the survey questions use the common Likert response scale format, enabling easy descriptive analysis within individual data and between the responses received in the eight survey areas.
Results
The survey closed January 31, 2012, with 655 responses having been received (Table 1). The sampling frame was determined by adding the members of the four professional associations and the CMRBV registrant list (n = 4774). 10 The number of CMRBV registrants who had insufficient mailing details (n = 116), the surveys returned to sender (n = 27), and the number of paper copies sent to CMRBV members (n = 1179) were then subtracted (the latter in response to the fact that 98% of the CMRBV respondents revealed that they also had at least one professional association membership), bringing the sample population number to 3737. This was then further adjusted to include the percentage who indicated they were a member of more than one professional group in their survey response (42%), giving the final calculated sample population of 1570. Adjusting for nonpracticing and professional association members who did not receive the survey invitation, and therefore as an exploratory and descriptive survey of a count unknown population at the time undertaken, the response rate of primary CM practitioners was therefore approximately between 42% and 55%.
Demographic characteristics
Roughly in line with CMRBV workforce data, more than half of CM practitioners surveyed were female (56.4%) and less than half were male (43.6%) (Table 1). 9 Survey participants were relatively young, although seven respondents reported being over 70 years old.
Place of birth
More than half of CM practitioners were born in Australia or New Zealand, with a significant percentage, just over 20%, naming China as their country of birth. This is in line with previous CMRBV workforce data (Fig. 1). 9

Respondents by country of birth. NZ, New Zealand.
Place of residence and practice
Although the largest proportion of respondents came from the Australian state of Victoria (nearly 50% [n = 203]), one quarter came from New South Wales (n = 100). The next highest responding state was Queensland (n = 63), and then South Australia (n = 17) and the Australian Capital Territory (n = 9). All Australian states and territories were represented, including Tasmania (n = 7), Western Australia (n = 7), and the Northern Territory (n = 3). As expected, nearly all respondents reported practicing in the state in which they resided.
Language
Although English was not the first language for one third of the CM practitioners who completed the survey, as shown in Figure 2, English was the language used professionally by most practitioners. Some of the other languages used in clinical practice include Korean (n = 6), Greek (n = 4), Italian (n = 3), Japanese (n = 3), and Vietnamese (n = 3).
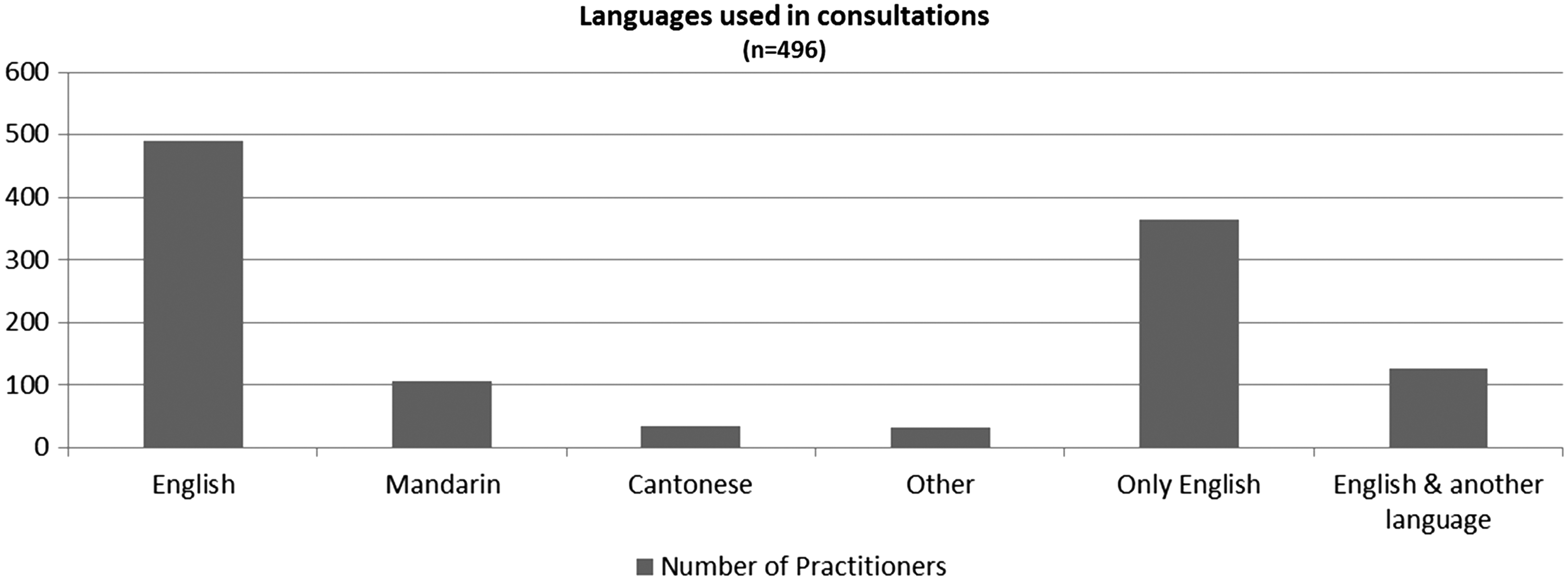
Languages used in clinical consultations.
Education
Of the total number of respondents to the survey, 34% (n = 223) had undertaken education in other areas apart from CM. One hundred and thirty-five had one other qualification, 60 respondents had two, and 28 had three. Of these respondents, 39% had two or more other qualifications. Most respondents had a bachelor degree level or higher in another field apart from CM.
As can be seen in Table 2, the areas of other qualifications included massage and shiatsu (n = 48); nursing (n = 36); and commerce, business, and management (n = 25).
CM qualifications
More than three quarters of CM practitioners said that they had a degree level education or higher in CM (Fig. 3).
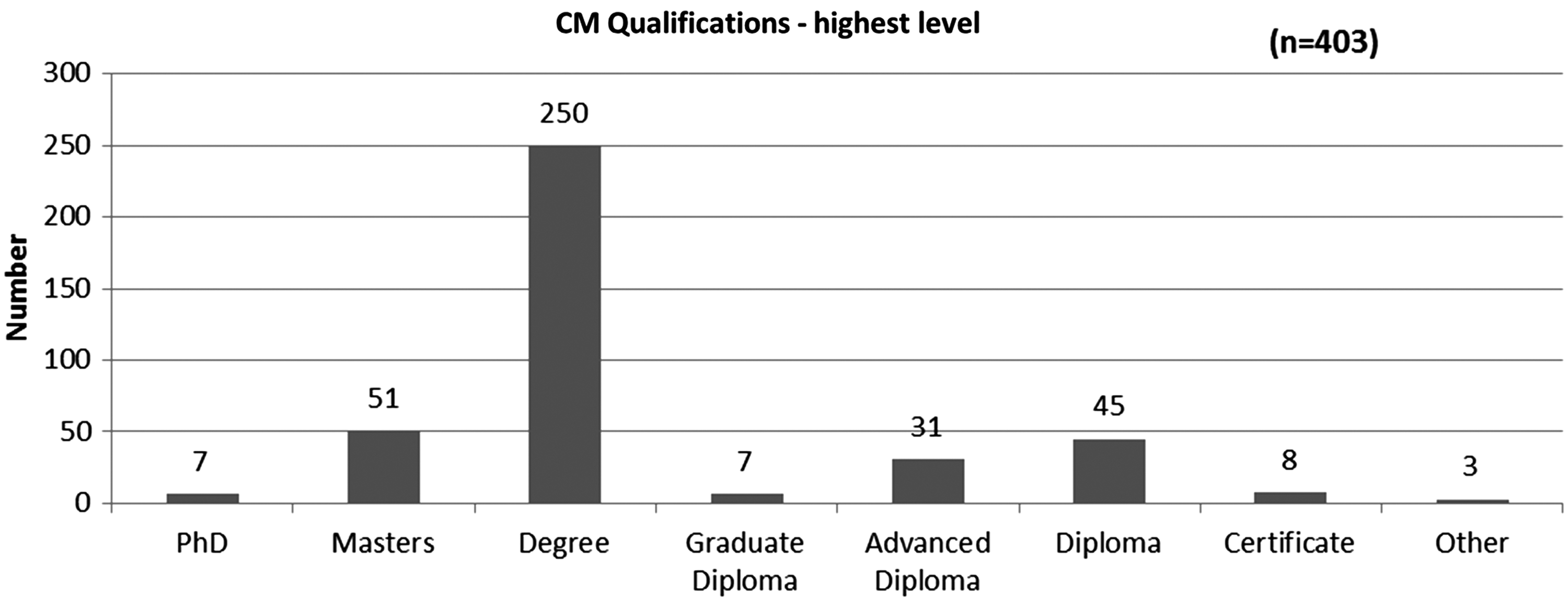
Highest level of Chinese medicine (CM) qualifications attained.
Years of clinical experience
Although a small proportion of respondents had more than 30 years of clinical practice in CM, about half of CM practitioners had less than 10 years of experience in CM. Because most are older than age 30 years (93%;see Table 1) and may therefore have some previous life experience, this suggests that the largest proportion of the workforce of CM practitioners in Australia is also relatively new to clinical practice, with 52% having less than 10 years' clinical experience in CM.
Reason for choosing CM as a career
By far most participants indicated that they had had an interest in the philosophy of CM and felt that experience with CM contributed to their decision to study and practice CM. Experiences in related practices, such as t'ai chi and martial arts, also affected the decision to enter into CM. Although a fair proportion of respondents were interested in the flexible work options available, interestingly, relatively few practitioners had chosen to practice CM for reasons associated with income (Fig. 4).
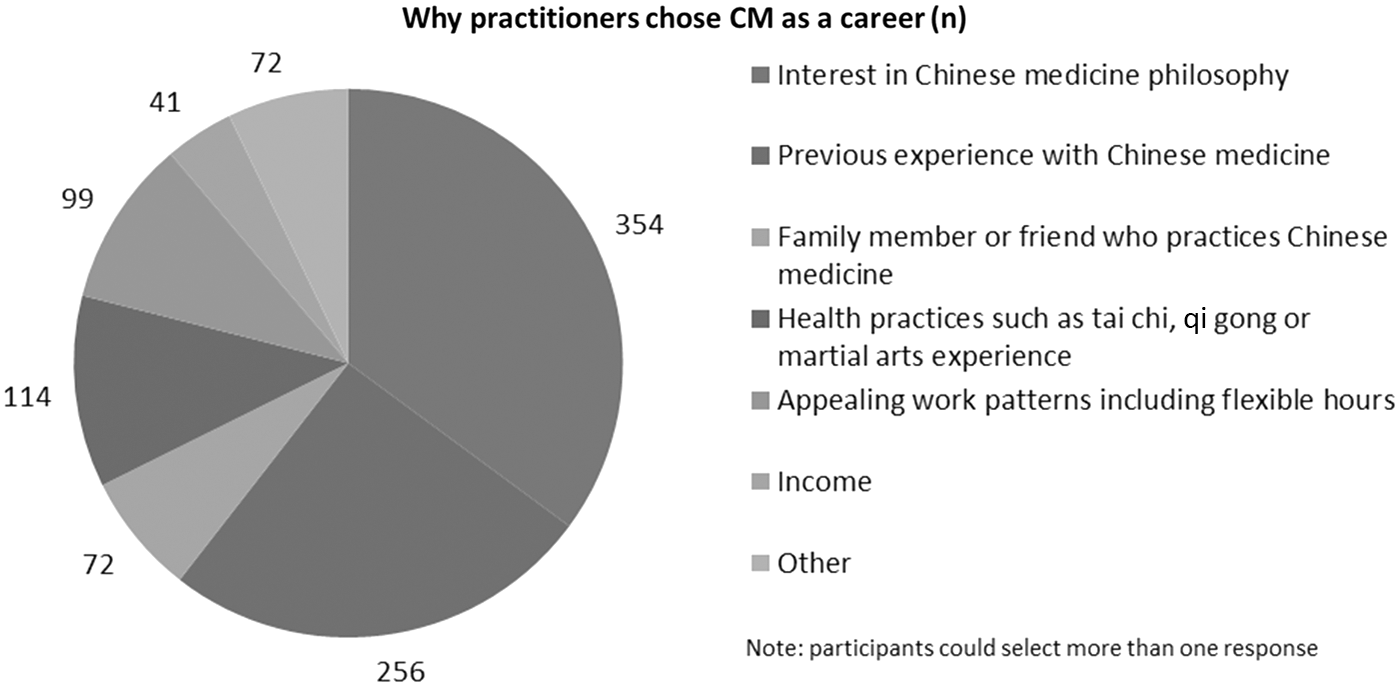
Reasons for choosing CM as a career.
Clinical practice
Most practitioners (83.1%) said that CM made up more than 70% of their clinical practice (Fig. 5). Most practitioners described their practices as combining acupuncture and CHM, or predominantly acupuncture.
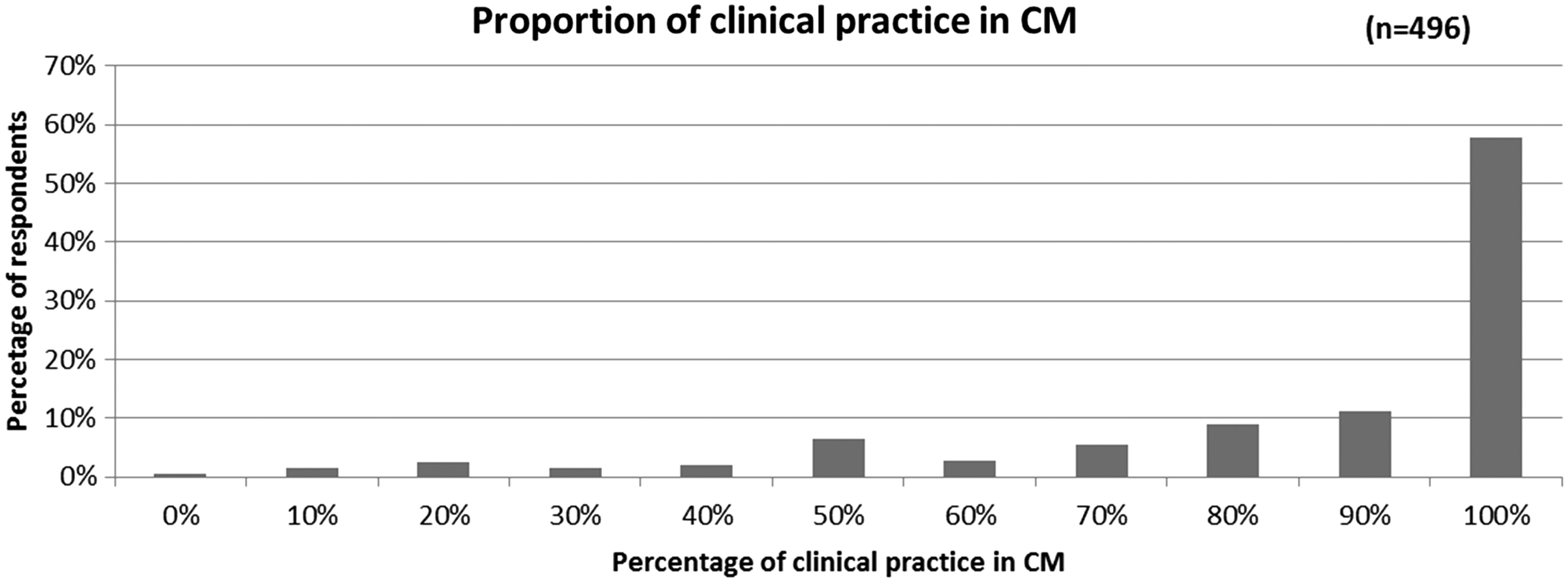
Proportion of clinical practice practicing primarily in CM.
CM modalities used in clinic
Acupuncture was the most frequently used CM modality in the clinic, with nearly all respondents (93%) reporting that they “frequently to always/almost always” used the technique with their patients in clinic. Chinese dietary and lifestyle advice was also “frequently to always/almost always” used, and Chinese herbal medicine in some form was also frequently used. Electroacupuncture, CM massage, nonscarring moxibustion, exercise advice, dermal hammer, gua sha, imbedding needles, and bleeding techniques were occasionally used. On the other hand, laser acupuncture, raw herbal decoctions, point injection therapy, and scarring moxibustion were generally reported as “never/almost never” used (Table 3). The main CM modalities reportedly used in the “other” category included ear seeds (n = 5), ear acupuncture (n = 3), Japanese therapies (n = 3), shiatsu (n = 2), and exercise therapy including qi gong (n = 2).
CHM, Chinese herbal medicine.
Techniques and practices generally regarded not to be primarily CM modalities are “never/almost never used” or used “occasionally” by CM practitioners. Bodywork techniques, including massage, were used the most, with one third of respondents using them at least half of the time. Practitioners reported that they use vitamin and mineral therapy, counseling, and nutritional advice only “occasionally” (Table 4). Other modalities used included Bowen therapy (n = 3), counseling (n = 3), exercise therapy including stretching (n = 2), Reiki (n = 2), birth preparation and hypnobirthing (n = 2), and meditation advice (n = 2).
Styles of acupuncture
When asked which forms of acupuncture they most used, most practitioners said they “always/almost always” used Chinese acupuncture techniques (n = 351). Ear acupuncture, five-element acupuncture, and eight-principles acupuncture styles were used “occasionally” or “frequently,” while Korean and Japanese styles were “never/almost never” used by most respondents (Fig. 6).

Styles of acupuncture practiced.
Most CM practitioners reported practicing out of one location (65.7 %), 26.8% said they practiced in two locations, and the remainder practiced out of three (5.7%) or four (1.8%) locations.
As can be seen in Figure 7, the largest number of practitioners indicated working in a solo practice, whether from home or in a public or commercial setting (n = 314). A roughly equal number again reported practicing in a shared CM practice or multidisciplinary practice with other practitioners (n = 302) (Fig. 7). These findings suggest that although many CM practitioners work in solo practice, many also work in shared clinical settings.

CM work arrangements.
A small number of practitioners reported doing work related to CM in a variety of other settings, most notably educational colleges and schools (n = 41), nongovernment/nonprofit settings (n = 38), and sports clinics/fitness centers (n = 32). Other locations included medical clinics, day spas and health retreats, herbal and health shops, yoga centers, and home visits.
The responses to the question asking how CM practitioners spend their work time each week (Fig. 8) show that on average practitioners spend most of their time—an average of 22 hours—in the clinic with patients. However, as can also be seen from Figure 8, they also spend many hours engaged in other professional activities.
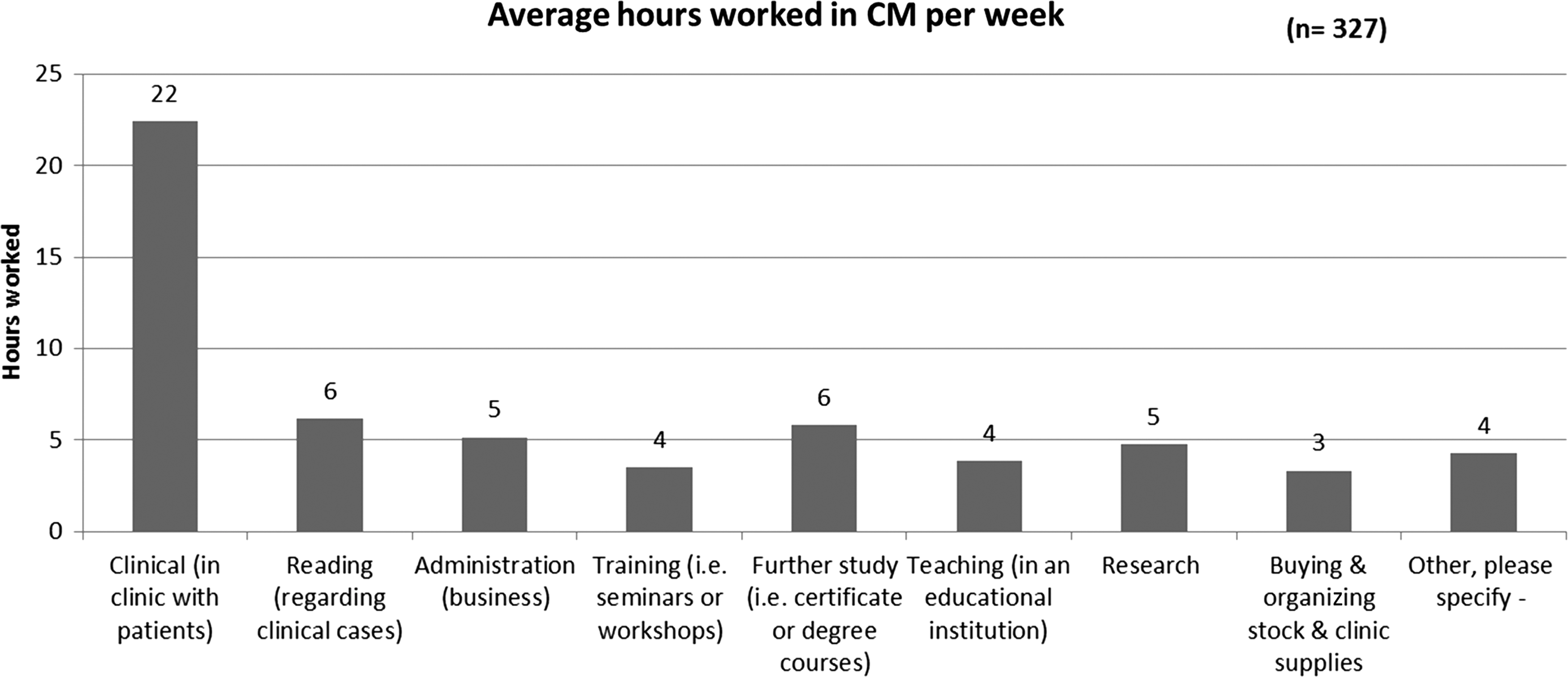
Average hours worked in CM per week.
When the number of patients per week that practitioners reported seeing in the clinic was compared with their average number of hours in the clinic, the number of clients seen by practitioners on average was found to be proportional to their hours worked in the clinic (Table 5).
Characteristics of CM consultations
Thirty percent of participants said that they saw on average between 11 and 20 patients per week (n = 149). Twenty-five percent reported seeing on average 10 or fewer patients per week (25%; n = 123), suggesting perhaps a part-time workforce or one in development. The mean number of patients seen each week by CM practitioners was 20. Eighty-six percent of practitioners spent 40 minutes or longer with new patients, and in subsequent consultations 65% continued to see patients for at least 40 minutes (Fig 9).
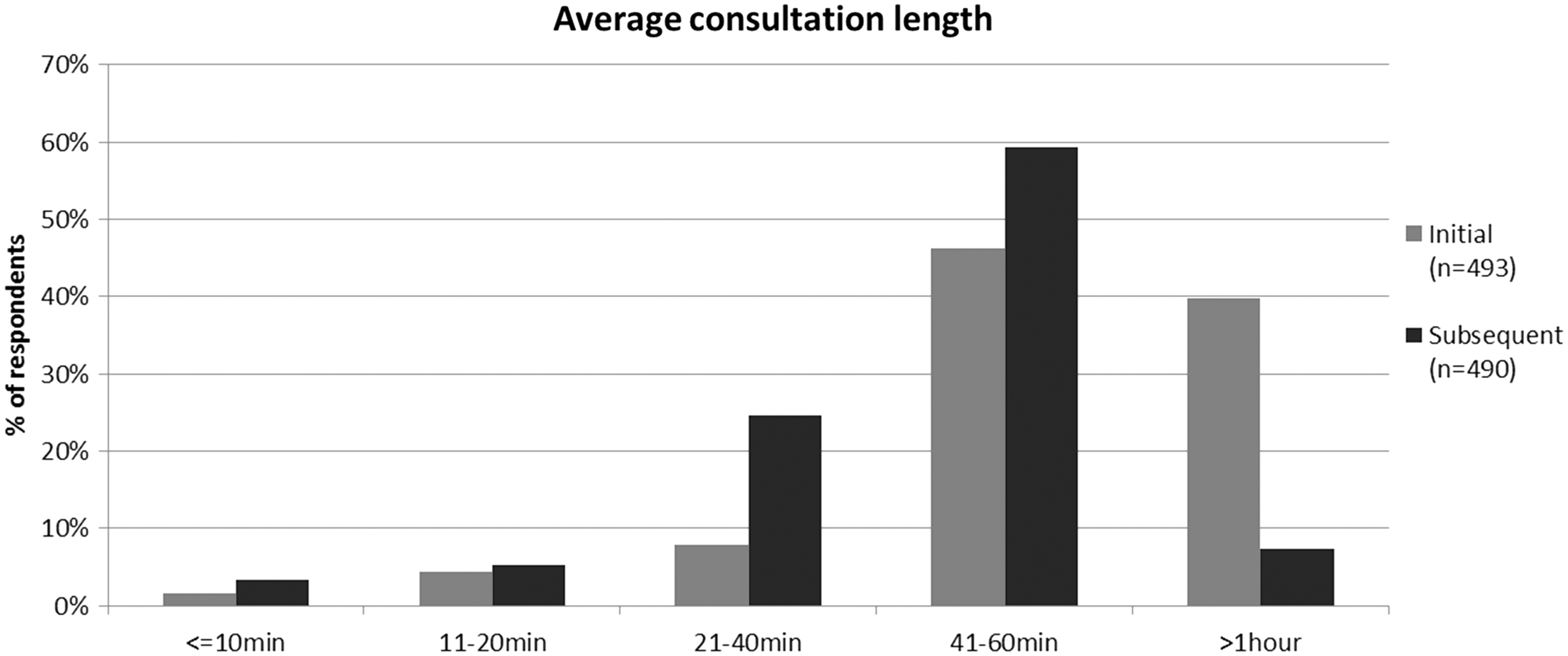
Average and initial consultation lengths.
CM consultation fees and payments
Practitioners charged a wide range of fees for their services (Fig. 10). Most charged more for the initial consultation, with the average initial consultation fee being $81–$90 and the average subsequent consultation fee $61–$70, and 82% charged between $41 and $80 for subsequent consultations. A variety of payment methods are offered by CM practitioners, with cash being the most common (n = 483) (Fig. 11).
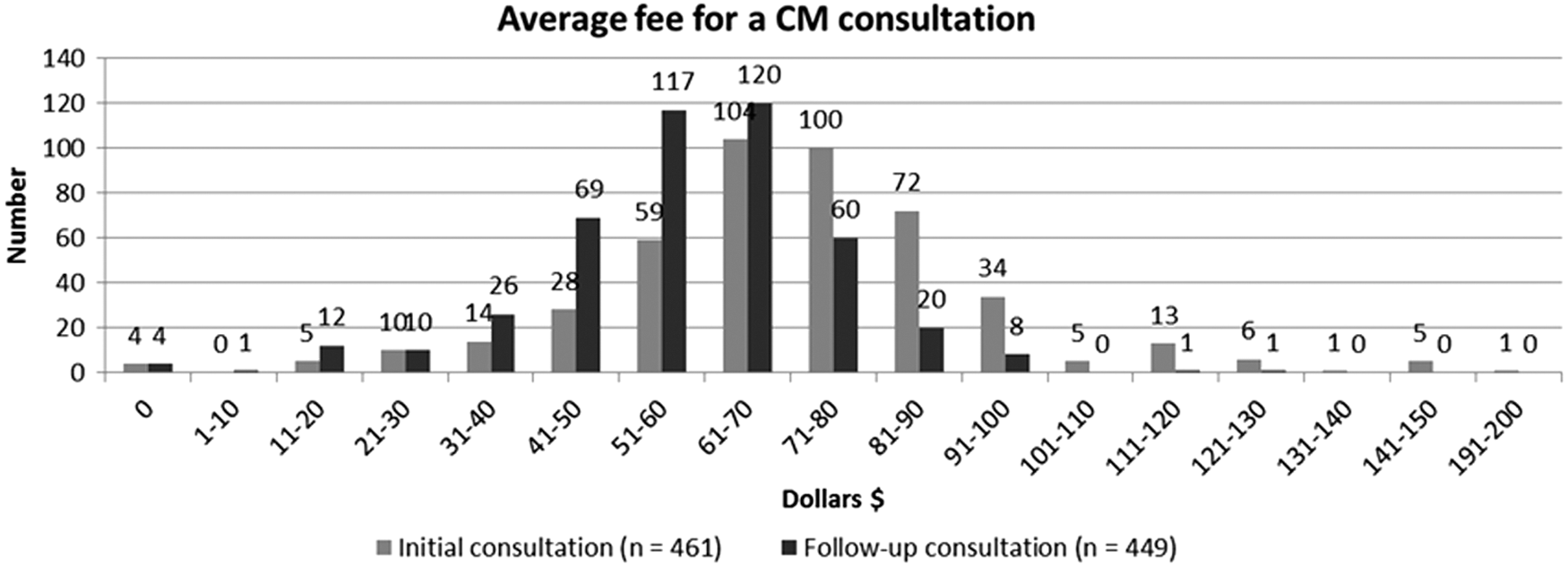
Average fee for a CM consultation.
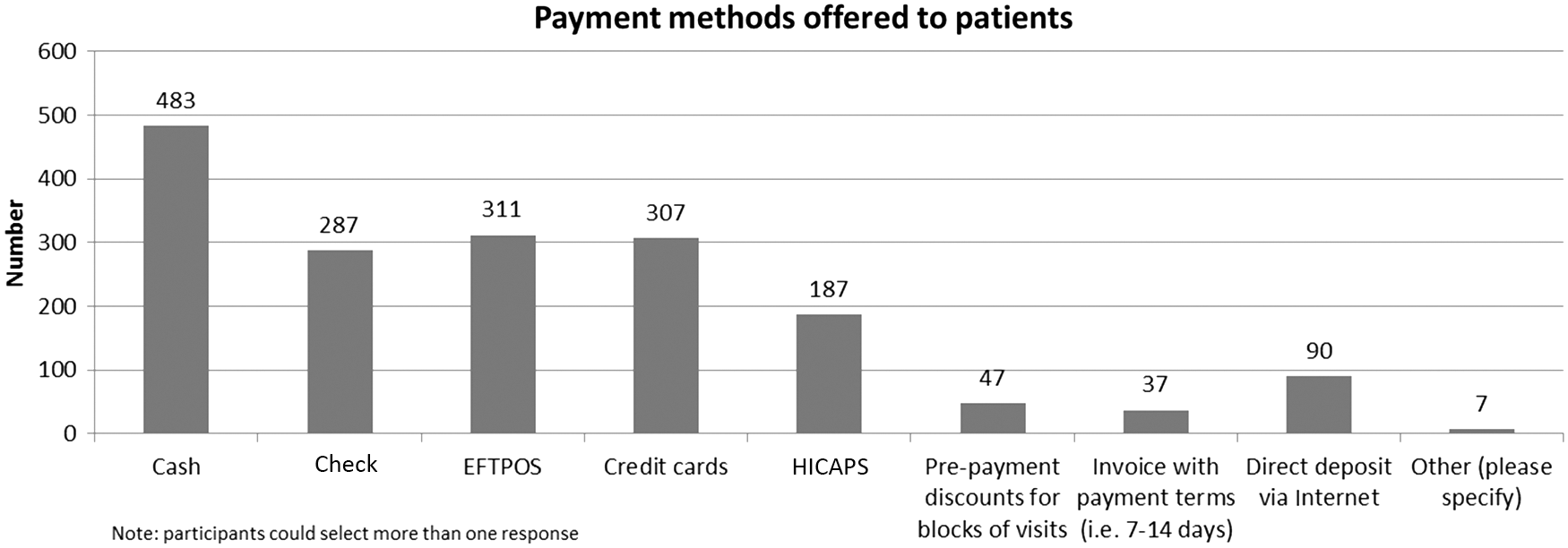
Payment methods. EFTPOS, electronic funds transfer at point of sale; HICAPS, Health Industry Claims and Payments Service.
At least 88% of practitioners “always or almost always” kept notes of patient consultations.
Most often, patient notes were in the form of paper or on cards (n = 365), although a small number did report using computerized records also (n = 157) (Fig. 12).

Forms of clinical records.
Discussion
CM practice in Australia has a complex and diverse nature. With 53.7% of practitioners born in Australia and New Zealand, 20.3% born in China and the rest from many other places in the world, they bring a range of previous life and employment experiences. Their education levels are high, predominantly being degree level, no doubt reflecting that in Australia CM has been offered at tertiary level, with a curriculum close to that in China with the addition of a large biomedical component, for the past 20 years. Mostly practitioners choose careers in CM because they are attracted to the philosophy and worldview it embodies. They also indicate that their experiences with CM—in relation to themselves or to a family member—had affected the decision to study and practice CM. The results presented here show that CM practitioners in Australia are roughly balanced between the sexes, mainly work in solo practice or multidisciplinary clinics, and practice predominantly in both acupuncture and CHM.
Some questions repeated (with permission) those used in previous workforce surveys carried out in Australia. This was intended to enhance comparisons with previous data, to facilitate reliability testing of survey results, and to enable ongoing longitudinal analysis of the CM workforce, as more studies are also carried out in the future. The results presented here reflect those results found previously, with some important additions and differences. 6,9 The primary CM practitioners surveyed here describe the nature of their practices in ways similar to those surveyed in the 1997 “Toward a Safer Choice” study, with the highest number of participants reporting that they practiced a combination of acupuncture and CHM. 6 In line with the 2009 CMRBV workforce report, in which 27% of CM practitioners reported seeing 11–20 patients per week, the largest group (30%) of practitioners in the current sample reported seeing exactly the same number. 9 Similar distributions in work arrangements and practitioner age groups were also found, aligning closely with 2009 CMRBV findings.
As expected, fees for follow-up consultations have risen since 1997, when the average follow-up fee was $32 for primary CM practitioners. 6 However, practitioners are spending about the same amount of time on average with their clients, with 60% spending 41–60 minutes, compared with 42 minutes on average in 1997. 6 This finding can be compared to studies of time spent with Australian patients in Western medicine, where the average general practice consultation length is 14.8 minutes. 13 Compared with “Towards a Safer Choice,” in which 97% of respondents made notes on consultations, in this study 95% of practitioners said they make patient notes “frequently or always/almost always.” 6 Also similar to the 1997 study, where 90% said they relied on a Traditional Chinese Medicine philosophy and theoretical framework in making their diagnosis and guiding their treatment decisions, 89% of the practitioners in the current study do this frequently to always/almost always. 6 The closeness of these results suggests that the survey is valid and may improve confidence in the original findings presented here.
This study adds to the documented evidence of an increase in the education levels achieved by CM practitioners over the last few decades. This has also been shown by the CMRBV workforce surveys, which indicated that degree level or higher qualifications have increased from 45% before 1989 to 87% in 2009. 9 Although the current study did not solely investigate registered practitioners, it nonetheless found that 78% of respondents across the country had a bachelor's level degree or a higher qualification in CM. It also emerged that CM practitioners often have degree level or higher qualifications in another field, suggesting that many practitioners come into CM with other skills and professional and life experience. Although a third of practitioners in the survey reported a language other than English as being their first language, the majority (nearly 99%) said that they practiced in English. Although this was a significant concern for the CM community in the transition to national regulation in 2012, these results suggest that overall, wherever the practitioners came from they acculturated to Australian professional expectations. At the same time, a substantial proportion also reported practicing in languages other than English, indicating a diverse workforce and patient demographic.
This study has several limitations, including the fact self-selection of participants and possible response biases; the lack of a comprehensive distribution network (as a result of which it was impossible to ensure that the survey was received by all primary CM practitioners); and use of the CMRBV database as part of the recruitment, which potentially affected the generalizability of the results. The fact that the distribution and replies were initially often Internet based—despite the availability of a paper option—suggested the possibility that the survey may not have reached all practitioners who were not on the Internet. Additional factors, such as the substantial survey length of 66 questions, and the fact that the survey was offered only in English and Chinese, while aiming to include the majority of the CM practitioner population, may have discouraged practitioners whose primary language is not English or Chinese. Despite these logistic and methodologic challenges, the survey likely provides the most complete and accurate account of CM practitioners and practice to the present time.
Conclusion
The results presented here contribute to a developing picture of CM practice in Australia. Where comparisons can be made, demographic and workforce data obtained are broadly consistent with those obtained in previous workforce surveys, supporting the validity of the findings.
This study has shown that CM practitioners in Australia come from a diverse range of backgrounds, are in general highly educated, and use many CM theoretical and practical approaches in their practices. They use multiple CM techniques and demonstrate high levels of professional practice standards in relation to receipting and note taking. A large proportion practice a combination of acupuncture and Chinese herbal medicine, and they practice in a variety of organizational settings, including solo practices and multidisciplinary clinics.
Data such as those presented in this study are important for the regulation and auditing of the profession and for assisting with the development of social policies, including those concerned with the distribution of health policy resources. CM already makes a substantial contribution to the provision of healthcare in the Australian community. As the latter continues to grow in both size and complexity, demands on the CM practitioner community will change and develop. It is hoped that the present study will provide a useful basis to assist both the profession itself and those involved in forming social policy to ensure that the needs of the wider Australian community are most effectively met.
Footnotes
Author Disclosure Statement
No competing financial interests exist.