
Abstract
Objectives:
During intensity-modulated radiation therapy (IMRT) for prostate cancer, the target, bladder, and rectum positions should be kept constant to reduce adverse events, such as radiation proctitis, and to increase local tumor control. For this purpose, decreasing the rectal contents as much as possible is important. Daisaikoto (DST) and bukuryoingohangekobokuto (BIHKT) are traditional Japanese herbal (Kampo) formulas that have been used to treat patients with abdominal bloating or constipation.
Materials and Methods:
This study investigated the effect of DST and BIHKT on the rectal gas volume during prostate IMRT according to Kampo diagnosis. Five patients were treated with DST or BIHKT at a dose of 5.0 or 7.5 g/d. The volume of rectal gas in 189 megavoltage computed tomographic images taken before each treatment session and the frequency of rectal gas drainage were evaluated before and after DST or BIHKT administration.
Results:
After DST or BIHKT treatment, the mean volume of rectal gas was reduced from 6.4 to 2.1 mL, and the mean frequency of gas drainage decreased from 43% to 9%.
Conclusions:
DST and BIHKT appear to be useful in reducing rectal gas, which would help prevent radiation proctitis and improve the local control of prostate cancer with IMRT.
Introduction
I
According to a recent report, the intrafraction motion of the prostate is caused by rectal filling and, to a lesser degree, by bladder filling. 2 Increasing volumes of rectal stool and gas would result in higher doses delivered to the rectum wall and lower doses delivered to the prostate and seminal vesicles, which could lead to increased adverse events, such as radiation proctitis and decreased local control of prostate cancer. Therefore, control of the intravesical urine volume and the volume of rectal stool and gas is needed. Several methods have been investigated to minimize prostate motion due to bowel distension; these include dietary guidelines, Western medicines, such as laxatives (magnesium oxide), deflatulents (simethicone, dimethicone), antiperistaltics (mosapride), fixed treatment times (after 10 a.m.), and rectal gas removal by the insertion of a finger or a rectal balloon. 3 –5 However, not all patients respond to these methods.
Therefore, the current study tested Japanese traditional herbal (Kampo) medicine that might be effective in reducing rectal gas. Kampo medicine is playing an increasingly important role in cancer care. 6,7 For example, hangeshashinto is effective for postoperative sore throat, and goreisan reduces postoperative nausea and vomitting. 8,9 The Kampo medicine daisaikoto (DST) is especially used in patients with constipation, 10 and bukuryoingohangekobokuto (BIHKT) is used in those with abdominal bloating. 11 DST is composed of 8 crude drugs in fixed proportions, and BIHKT is composed of 9 (Table 1). The effectiveness of DST and BIHKT in reducing rectal gas has never been reported in the English-language literature. These crude drugs derived from DST and BIHKT exhibit accelerated intestinal propulsion 12 –19 and cathartic action. 20 In light of these pharmacologic actions, the current study investigated whether DST and BIHKT were effective in reducing rectal gas in patients with prostate cancer undergoing IMRT.
DST, daisaikoto; BIHKT, bukuryoingohangekobokuto.
Materials and Methods
Patients
Between November 2013 and November 2014, DST or BIHKT (Tsumura Co., Tokyo, Japan) 21 was prescribed to five patients in whom the amount of rectal gas was considered to be excessive during IMRT. They had already been prescribed mosapride and dimeticone before undergoing planning CT, and they had to undergo gas drainage using a catheter numerous times. Extracts of DST or BIHKT, 2.5 g, were administered orally two or three times daily immediately before meals according to Kampo diagnosis during radiotherapy. Only one patient received a cathartic drug during the study. Kampo treatment was a second-line therapy following conventional cathartic drugs. Physical examination, interview, and blood test were carried out during administration to check for adverse events using the Common Terminology Criteria for Adverse Events version 4.0.
MVCT Images
With HT, MVCT images of the patient can be obtained in the treatment position before each treatment. These images are acquired in order to check and correct, if necessary, the patient position for treatment. Inaccurate patient positioning results in geographic misplacement of the dose distribution. Radiation beams used for imaging on the HT unit are generated by the linear accelerator that generates treatment beams. Therefore, the beam energy is in the megavoltage range. 22
Evaluation
The frequency of gas drainage using a 26-Fr SAFEED Nelaton catheter (Terumo, Tokyo, Japan) with lubricating jelly (C.R. Bard, Inc., Murray Hill, NJ) was evaluated before and after DST or BIHKT administration. The frequency of gas drainage (percentage) was the number of gas drainage sessions/total IMRT sessions before and after DST or BIHKT treatment × 100.
The volume of rectal gas was measured with the following procedures. First, initial MVCT data from the HT planning software were sent to the Pinnacle 3 workstation (Philips Medical Systems, Madison, WI), and MVCT images were fused with initial planning CT images. In the next step, the images were threshold-filtered between 100 and 800 Hounsfield units to separate gas from tissues. The MVCT threshold is different from the CT threshold. Therefore, the air existing outside the body was used. Finally, the volume of rectal gas from the top to the bottom of the pubis was measured. A total of 189 MVCT images (33 MVCT images in one postoperative patient and 39 MVCT images in the other four patients) were analyzed.
Results
Preliminary results
Table 2 shows the patient characteristics. The mean age of the five patients was 72 years (range, 67–81 years). The daily dose was 2 Gy, and the total doses were 66 Gy in the postoperative patient and 78 Gy in the other patients. After 7 days of BIHKT or DST treatment, the volume of rectal gas decreased in all patients, and the frequency of gas drainage was also reduced (Table 3). Adherence to the Kampo formulas was good in all patients. No grade 2 or higher acute adverse events occurred.
PC, prostate cancer.
Case report
In December 2013, a 75-year-old man (patient 3) visited a local doctor and had elevated prostate-specific antigen (PSA) levels. He visited Fukui Saiseikai Hospital in January 2014 and was diagnosed with high-risk prostate cancer according to the D'Amico classification (T3bN0M0, Gleason score 9, and initial PSA level of 83.941 ng/mL). At first, he was treated with neoadjuvant hormone therapy for 5 months. Then, he underwent IMRT using HT. Mosapride and dimeticone were prescribed for exhausting rectal gas. His stool remained hard during IMRT for 2 weeks, so he was also prescribed mashiningan as a cathartic drug. His stool became soft, but the frequency of gas drainage did not change. Therefore, mashiningan was switched to DST after 26 fractions of IMRT. The frequency of gas drainage then decreased. Figure 1 shows the change in rectal gas volume and the frequency of gas drainage, and Figure 2 shows MVCT images indicating the improvement of rectal gas.
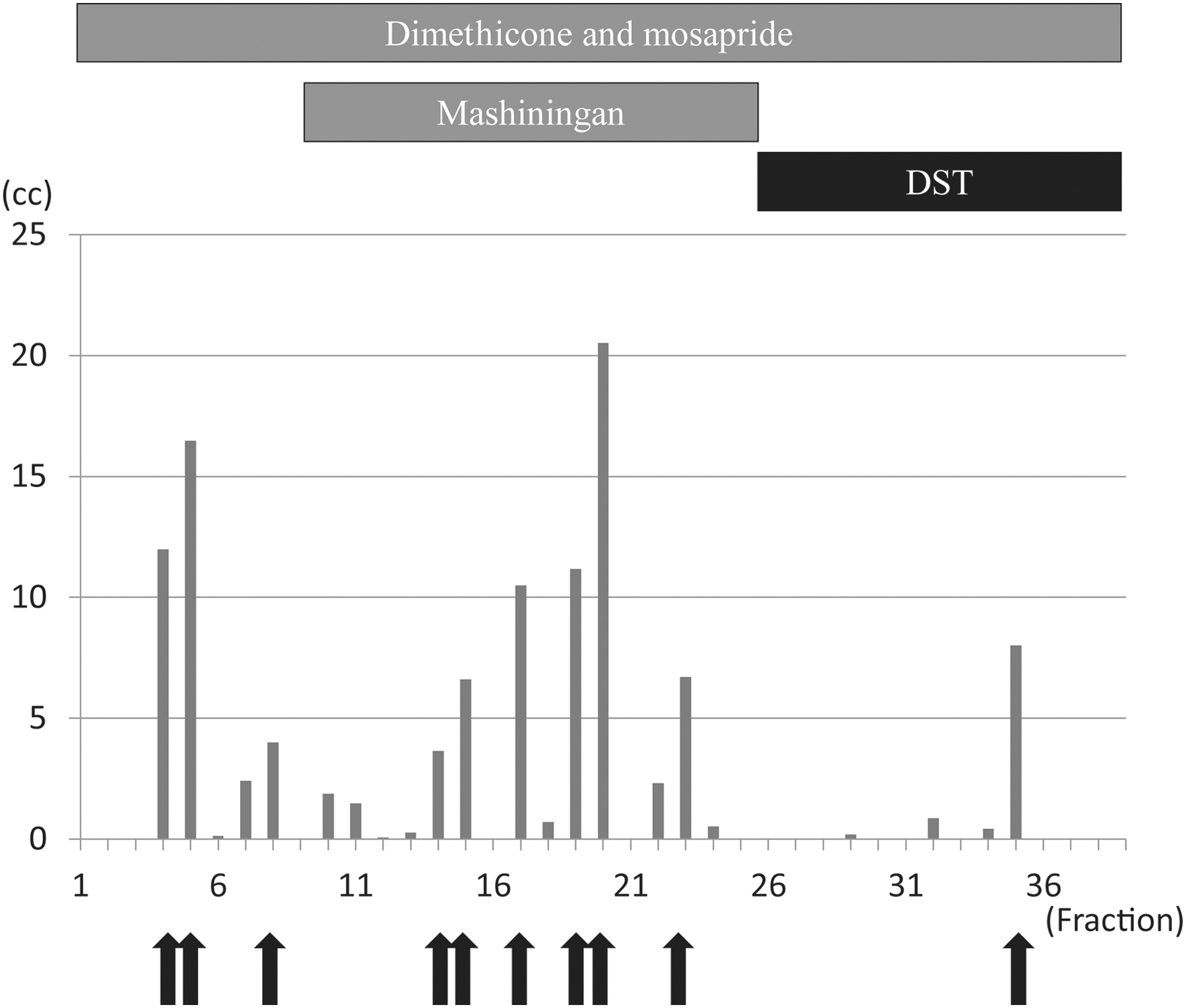
Volume of rectal gas at respective treatment sessions. Arrows indicate gas drainage. Mashiningan softened the patient's stool, but the frequency of gas drainage did not change. After administration of Daisaikoto (DST), the volume of rectal gas was apparently reduced and the frequency of gas drainage also decreased.
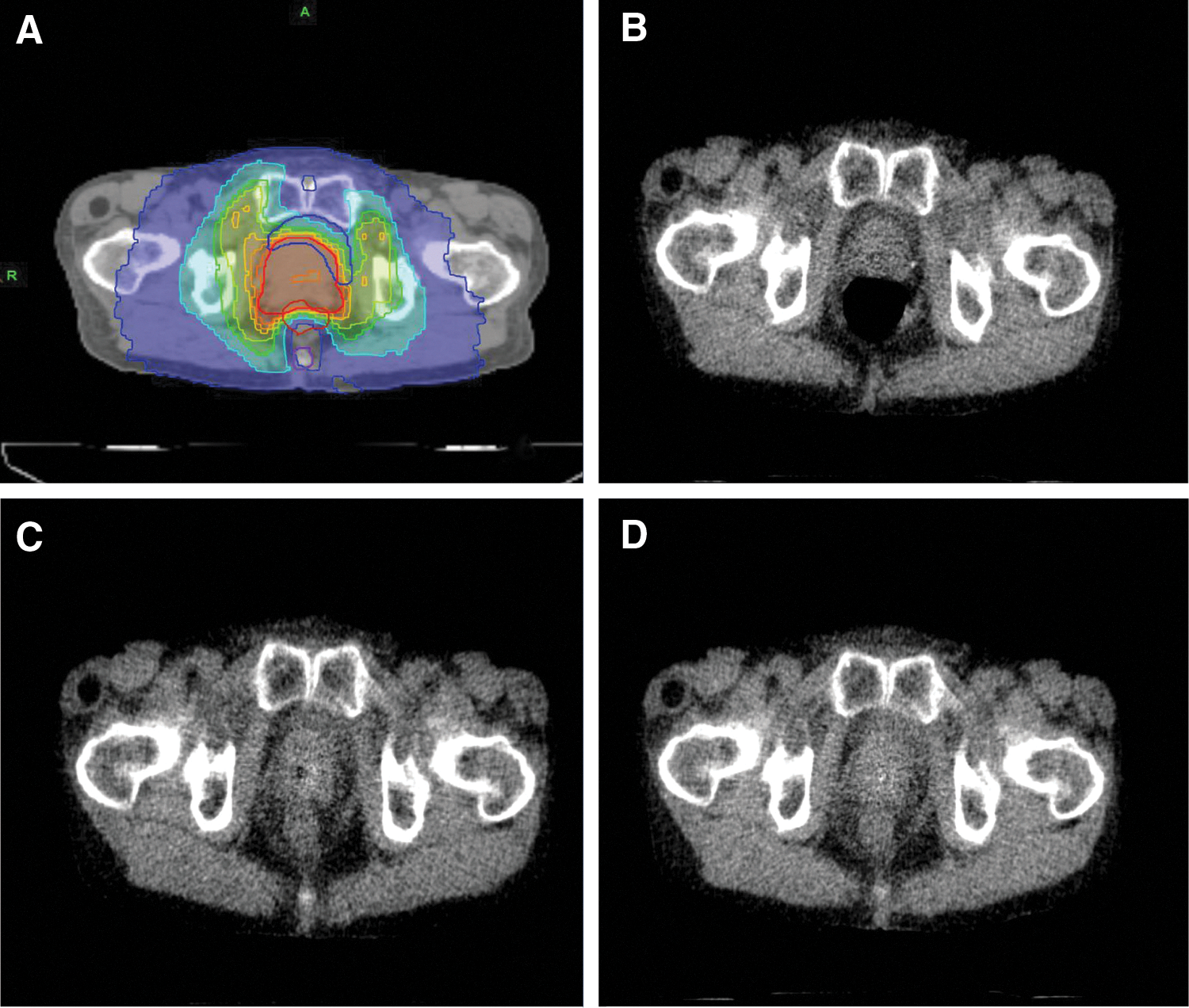
Imaging findings in patient 3.
Discussion
This study has suggested that both BIHKT and DST are useful for decreasing rectal gas with minimal toxicities. Acceleration of intestinal motility or catharsis by BIHKT and DST might be major factors for reducing rectal gas. Other methods to decrease rectal filling are not always successful. Deflatulents and antiperistaltics are sometimes ineffective, and it is often difficult to remove gas with laxatives because only stools are expelled. Many patients with prostate cancer receive radiation therapy while maintaining a job, so not all patients can receive radiation therapy after 10 a.m. The dietary guidelines used in the United States consist of avoiding flatulogenic foodstuffs and swallowing air, magnesium oxide tablets, and fixed treatment times. 4 In fact, gas production is influenced by two major factors: the amount of fermentable foodstuffs that escape from small bowel absorption and enter the colon and the composition of the colonic flora. Thus, bloating may be a clinical feature of malabsorption disorders, in which excessive amounts of unabsorbed substrates are fermented in the colon. 23 Therefore, avoiding flatulogenic foodstuffs appears to be logical. However, a recent study reported that antiflatulent dietary advice for patients undergoing prostate IMRT does not reduce the intrafraction movement of the prostate afterward. 24 It was estimated that, by altering their specific food pattern, their bowel movement might be stimulated, leading to the opposite effect of increased intrafraction motion instead of the intended decrease. Furthermore, the specific dietary guidelines are difficult to manage and check because elderly Japanese people prefer to eat these fibrous vegetables. When rectal gas cannot be controlled by these methods, the gas is usually removed by the insertion of a finger, rectal balloon, or catheter. However, these procedures take time, embarrass patients, and affect the fixed treatment time of other patients.
DST and BIHKT have been empirically used for patients with abdominal bloating or constipation. As shown in Table 1, three crude drugs (Pinelliae tuber, Aurantii fructus immaturus, and Zingiberis rhizoma) of BIHKT are common with DST. Pinelliae tuber, 12 A. fructus immaturus, 13,14 and Zingiberis rhizoma 15 are associated with accelerated intestinal propulsion. [6]-Shogaol and [6]-, [8]-, or [10]-gingerol derived from Zingiberis rhizoma enhance the intestinal transport of a charcoal meal. 15 Besides the three common crude drugs, BIHKT is composed of Atractylodis lanceae rhizoma, 16 Magnoliae cortex, 14 Perillae herba, 17 Ginseng radix, 18 Aurantii nobilis pericarpium, and Hoelen. β-Eudesmol and hinesol, belonging to the sesquiterpenoids derived from A. lanceae rhizoma, also clearly enhanced intestinal charcoal transport in mice. 16 Perillaketone, a monoterpenoid component of essential oil, was isolated from the leaf of Perillae herba as an active principle component of intestinal propulsion in mice. 17 Besides the three common crude drugs, DST is composed of Bupleuri radix, 19 Paeoniae radix, 13 Scutellariae radix, Zizyphi fructus, and Rhei rhizoma. 20 Saikosaides of Bupleuri radix have a strong stimulatory effect in the intestinal propulsion test in mice. 19 Hesperidin of Paeoniae radix stimulates gastrointestinal movement. The effect of hesperidin is mediated via the H1 histamine receptor. 13 DST contains Rhei rhizoma, which shows accelerated intestinal propulsion 14 and cathartic action. 20 Sennoside A is the main cause of the diarrheal activity of Rhei rhizoma. 20 According to these results, DST is considered to have stronger cathartic action than BIHKT.
DST and BIHKT are formulas from Japanese traditional medicine, Kampo medicine. Traditional Chinese Medicine (TCM) was adopted in Japan as orthodox medicine in the sixth century, 25,26 and since then, Kampo has developed uniquely from TCM, although they share many of the same basic theories and formulas. Modern medicine took over from Kampo medicine more than a century ago, but some Kampo formulas are still officially registered by the Japanese Ministry of Health, Labor and Welfare and covered by the National Health Insurance. 25 Kampo formulas are prescribed according to the collection of subjective and objective symptoms, namely, the exhibited pattern. They are prescribed in accordance with the patients' pathophysiology, which is thought to be reflected in this pattern. 26 –28 Intestinal stagnation, including gas and stool in the rectum, generally affects the lungs and intestines. It is attributed to heat and constraint, which allow the formation of qi stagnation. Appropriate strategies are to unblock the stagnation of qi, eliminate the phlegm, clear the heat, and remove the constraint. If there is also clumping of heat with stasis and stagnation, herbs such as Rhei rhizoma and Scutellariae radix should be added to drain heat and dispel stasis. In this regard, DST is one of the most suitable formulas for the treatment of constipation with stagnation of qi and heat. If internal heat does not exist and stagnation of phlegm is the main cause of patient conditions, BIHKT would be a better choice.
As patient 3 shows, it is difficult to reduce rectal gas with Western medicine alone, such as laxatives, deflatulents, and antiperistaltics. In this study, the mean volume of rectal gas decreased by 3.4 mL in patient 3. This decrease of rectal gas would have been caused by the pharmacologic actions of the crude drugs mentioned above. Without use of DST, the rectal gas would have to be drained numerous times by using a catheter, so the treatment time would be extended and the patient would be troubled with gas during a long treatment time. Management of rectal gas during IMRT is indispensable for prostate cancer because increasing volumes of rectal gas would result in higher doses delivered to the rectum wall and lower doses delivered to the prostate and seminal vesicles, which could lead to increased adverse events, such as radiation proctitis, and decreased local control of prostate cancer.
In conclusion, both BIHKT and DST might be useful for the management of rectal gas with minimal toxicities. BIHKT and DST have pharmacologic actions in patients with accelerating intestinal motility or catharsis. Because this study investigated the usefulness of BIHKT or DST in only five cases, further studies with more patients and, preferably, prospective randomized studies are warranted to confirm the findings.
Footnotes
Acknowledgments
The authors are grateful to Ms. Fumiyo Yamagishi for her valuable help in this research.
Author Disclosure Statement
No competing financial interests exist.