
Abstract
Objective:
To evaluate the immediate effects of traditional local thermal therapy with indirect moxibustion on renal hemodynamics in patients with chronic kidney disease (CKD) by using Doppler ultrasonography (US).
Design:
Examiner-blinded crossover study.
Participants:
Forty-three participants with CKD (mean age ± standard deviation [SD], 44 ± 15 years; estimated glomerular filtration rate, 69.5 ± 25.5 mL/min per 1.73 m2; 20 men and 23 women).
Intervention:
Participants received three successive treatment sessions of indirect moxibustion bilaterally at BL 23, a crucial acupuncture point, in the session. In the control session, the examiner was blinded by using smoke and aroma produced by moxibustion performed in an ashtray placed near the patient's body.
Outcome measures:
The main outcome measure was resistive index (RI) in the renal segmental arteries. Blood flow parameters, including RI, were measured for six renal segmental arteries by using Doppler US at rest (baseline), immediately after completion of moxibustion (post 1), and 10 minutes later (post 2). Adverse events were monitored during intervention.
Results:
In the control session, RI at post 1 (median [first, third quartile]: 0.587 [0.562, 0.626]) and post 2 (0.583 [0.567, 0.629]) did not change significantly compared with baseline (0.592 [0.563, 0.636]), while in the treatment session, RI at post 1 (0.565 [0.530, 0.618]) and post 2 (0.561 [0.533, 0.614]) decreased significantly compared with baseline (0.590 [0.550, 0.652]) (p < 0.001 and p < 0.001, respectively). The reduction in RI from baseline to post 2 in treatment session was significantly greater than in control session (mean ± SD, −0.026 ± 0.028 versus −0.003 ± 0.028; mean difference, −0.023 [95% confidence interval, −0.036 to −0.010]; p = 0.001]. No adverse events, such as burns, were observed during the study period.
Conclusion:
Renal vascular resistance was decreased after indirect moxibustion therapy in patients with CKD.
Introduction
“C
Doppler ultrasonography (US) provides noninvasive, morphologic, real-time information about renal vasculature. The intrarenal resistive index (RI) is a parameter of renal vascular resistance measured by US, and a high value helps predict CKD progression 4,5 and cardiovascular damage. 6 This parameter has also been used to study the therapeutic effects of various medical treatments on the kidney. 7 –11 The peak systolic velocity (PSV), also measured by US, has been reported to increase with CKD stage and is correlated with several renal histologic changes. 12 Doppler US has also been used to evaluate the effects of complementary medicines, such as acupuncture and local thermal stimulation, including moxibustion. 13 –18
Moxibustion is a traditional local thermal therapy involving burning moxa, made from a medicinal herb called mugwort, at acupuncture points. Like acupuncture, moxibustion is an element of East Asian medicine and has been used to alleviate various symptoms. These treatments have also been found to alter renal function. 19 –23 Traditional Chinese Medicine theory focuses largely on BL 23, a crucial acupuncture point, for treatment of various symptoms of renal diseases. It has been previously reported that indirect moxibustion, a type of moxibustion, at BL 23 brought about renal hemodynamic changes in healthy individuals. 13 However, its effect on renal hemodynamics in patients with kidney diseases still remains unclear.
To the best of the authors' knowledge, US has not been used to assess renal hemodynamics after moxibustion treatment in patients with CKD. The study hypothesis was that moxibustion would decrease renal arterial RI in patients with CKD. The study's aim was to evaluate the short-term effects of traditional moxibustion thermal therapy on renal hemodynamics using US in patients with CKD.
Materials and Methods
Study design
An examiner-blinded crossover study design was used to compare various parameters between the treatment (indirect moxibustion) and control sessions. Participants were randomly assigned to two groups by using a computer-generated random sequence. The first group received treatment sessions, and the second group received control sessions. Both groups received crossover intervention after 1 month.
Participants
Participants were recruited from the outpatient Department of Nephrology at the Gifu University Hospital, Japan. Patients who had stage 1–5 CKD and were not undergoing dialysis were included in this study. CKD was diagnosed according to the National Kidney Foundation practice guidelines, 2,24 and stage was classified by using the estimated GFR. 24 Exclusion criteria included inability to maintain resting position, skin burn caused by inability to feel heat sensation due to any reason, receipt of ≥40 mg of prednisolone per day, history of skin conditions, skin fragility, and renal artery stenosis. Patients were also excluded if medication doses were increased, conditions worsened, or other medications were required during the study period.
Moxibustion
An indirect moxibustion preparation (Senefa, Shiga, Japan) commercially available in Japan was used, similar to a previous report. 13 This moxibustion type avoids direct contact with the skin because of a paper pulp base (Fig. 1), and the patients feel only a warm, comfortable sensation. The peak temperature on the contact surface is approximately 48°C–49°C and is reached within 4 minutes of ignition. 25,26 If patients reported excessive heat, the device was removed immediately to avoid burns.

Image and structure of indirect moxibustion. This form of moxibustion avoids direct contact with the skin because of its paper pulp base.
In the treatment session, indirect moxibustion was applied bilaterally at point BL 23 (Shenshu). This point is located in the lumbar region at the level of the inferior border of the spinous process of L2 and is 1.5 B-cun lateral to the posterior median line, according to the World Health Organization standard textbook 27 (B-cun is a standard measuring unit used in the textbook). Moxibustion treatment was applied three times in succession, and the average time between ignition and removal was approximately 4 minutes. Thus, the total moxibustion therapy duration was approximately 12 minutes. All treatments were administered by a nephrologist.
In the control session, the examiner was blinded by using the smoke and aroma produced by carrying out moxibustion in an ashtray placed near the patient's body.
Outcome measures
The primary outcome measurement was RI in the renal segmental arteries. Blood flow parameters, including PSV and end-diastolic velocity (EDV), were measured for six renal segmental arteries (three from each kidney) using real-time Doppler US with a 3.5-MHz convex-type probe (Prosound α7; Aloka Co. Ltd, Tokyo, Japan). The scan showing the maximum longitudinal dimension was chosen for measurement. After color Doppler US observation, the blood od-flow velocities in segmental arteries were measured using pulsed Doppler US (Fig. 2). The segmental arteries were chosen because previous studies have reported that clear signals can be reliably obtained from these vessels. 4,5,13,28 The measurements were taken by a well-trained nephrologist with >5 years of experience. The examiner was not present in the treatment room except during measurement for blinding regarding intervention type. RI was calculated as follows: [(PSV – EDV)/PSV].
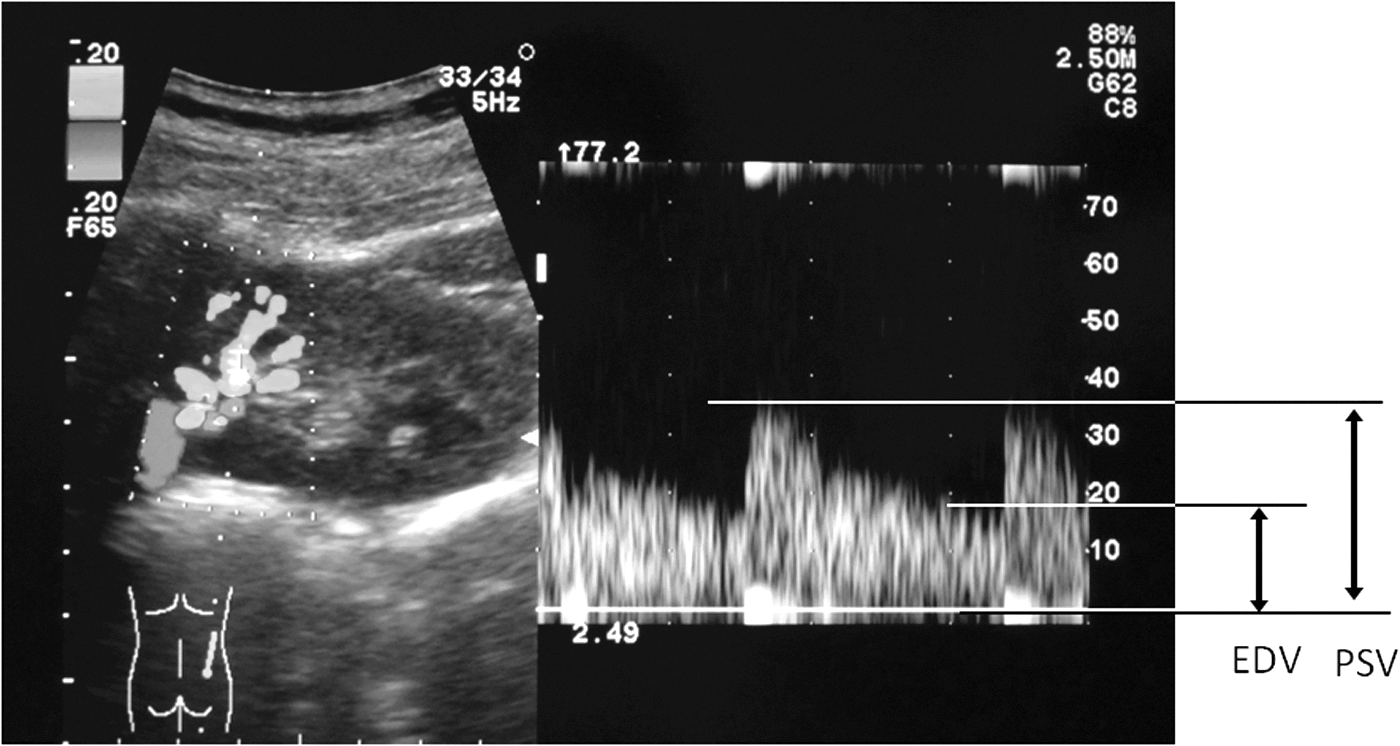
Renal Doppler ultrasonography (US) image for the evaluation of the renal hemodynamics. (Left) Two-dimensional Doppler US image. (Right) Doppler US spectrum image. EDV, end-diastolic velocity; PSV, peak systolic velocity.
The timeline of the present study is shown in Figure 3. Before moxibustion, participants were asked to rest in a prone position in a quiet, air-conditioned treatment room for 10 minutes. US was performed before moxibustion (baseline), immediately after moxibustion (post 1), and 10 minutes after moxibustion (post 2).
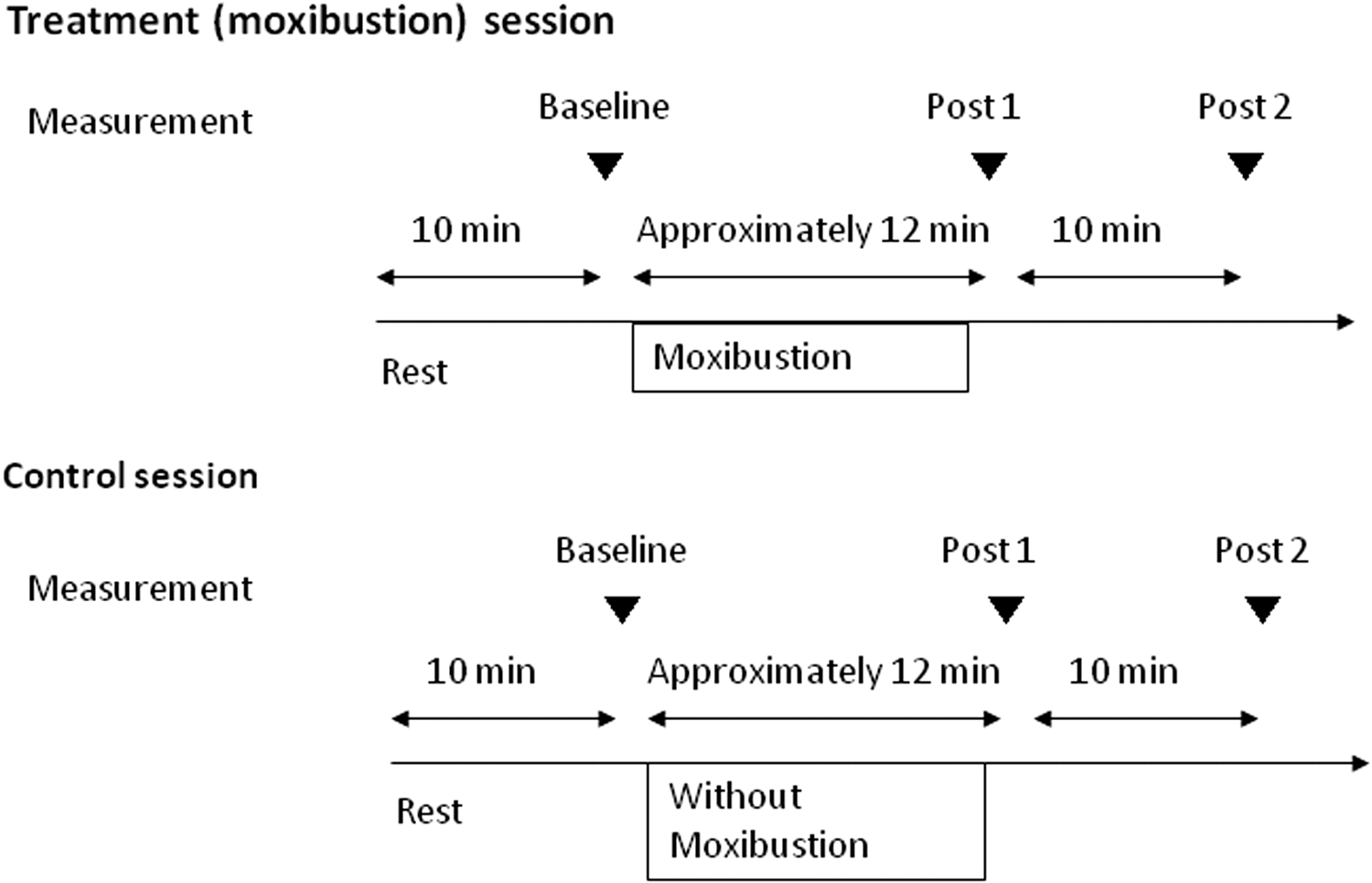
Time course of the study. Rest: participants remained in the resting state in prone position. Without moxibustion: ignition of moxibustion on ashtray near the patient's body. Post 1, immediately after completion of moxibustion; post 2, 10 minutes after completion of moxibusion.
Blood pressure (BP), heart rate (HR), and body temperature (BT) were measured at the same time points. BP and HR were measured by using an automatic sphygmomanometer (H55 Terumo, Tokyo, Japan), whereas BT was assessed with an electronic thermometer (EM-30CPLB, Terumo, Tokyo, Japan). The presence of adverse effects, such as burning or pain, was monitored throughout the treatment. After completion of all measurements in the moxibustion session, information on the patients' impressions of the levels of heat sensation and comfort associated with treatment was collected by using ordinal categorical scores. The heat sensation was scored as 1: no sensation, 2: not very hot, 3: warm, 4: intermediately hot, and 5: extremely hot, whereas comfort was scored as 1: very pleasant, 2: somewhat pleasant, 3: mild, 4: somewhat unpleasant but endurable, and 5: unpleasant.
The study protocol was approved by the Ethics Committee of Gifu University Graduate School of Medicine and was in accordance with the Helsinki Declaration. All participants provided written informed consent.
Statistical analysis
The primary variable was change in RI from baseline to post 2 in the treatment and control sessions. The required sample size was calculated to be 52 patients, based on a significance level of 0.05 (two-tailed t test), a power level of 0.8, and an anticipated effect size d of 0.40. With the addition of a 15 % dropout rate, the number of patient was required to be ≥60. The Shapiro–Wilk test was used to assess normal distribution. Parametric variables were expressed as mean and standard deviation (SD) or 95% confidence interval (CI), whereas nonparametric data was reported as median and quartile (first and third). When the value at each time point (baseline, post 1, and post 2) for the two groups was parametric in nature, two-way repeated-measures analysis of variance with post hoc Dunnett test was used to compare baseline values to either posts. When the data were nonparametric in nature, the Friedman test with post hoc Wilcoxon signed rank test was used for comparison (two comparisons: baseline versus post 1 and post 2) in each session.
The changes from baseline to post 2 were compared between treatment and control sessions using a paired t test for parametric variables or Wilcoxon signed-rank test for nonparametric variables. For subgroup analysis, an unpaired t test or Mann–Whitney U test was used to compare the changes in RI at post 2 between patients with and without renin–angiotensin system inhibitor (RASI), patients with CKD higher stage (stage 3, 4) and lower stage (stage 1, 2). To test for period and carryover effects, an independent sample t test was used on the difference and the sums, respectively, of the summary scores of the changes from baseline in RI for the first and second interventions. The Spearman rank correlation test was used to test for association between the patients' impression (heat and comfort levels) and the changes in RI from baseline to post 2 of the treatment session.
The significance level was fixed at 0.05/n for the Bonferroni correction, where n is the number of comparisons made in the post hoc Wilcoxon test. For the other statistical tests, p values <0.05 were considered to represent statistically significant differences. All statistical analyses in the present study were performed using by SPSS for Windows, version 22 (IBM, Armonk, NY).
Results
Although 60 patients provided written informed consent, only 43 finished all procedures; their data were statistically analyzed. Twenty-four patients received treatment sessions first, and 19 received control sessions first. The patient's characteristics are shown in Table 1. Good US images were not available for 10 patients because of technical difficulties, 2 patients could not maintain resting positions while being prone during measurement because of urinary urgency, and 1 patient was unable to breath-hold during the US measurements. One patient did not provide consent. Examiner blinding was not possible for 1 patient because he revealed his allocation. One patient increased medication for steroid pulse treatment during the study period, and measurement was stopped in another because of hypotension on the day. All these 17 patients were excluded from the statistical analysis.
Data are shown as a number or mean ± standard deviation.
eGFR, estimated glomerular filtration rate; BMI, body–mass index; BP, blood pressure; RASI, renin–angiotensin system inhibitor; ARB, angiotensin-receptor blocker; ACEI, angiotensin-converting enzyme inhibitor; CKD, chronic kidney disease.
Changes in RI and other renal hemodynamics parameters are shown in Figures 4 and 5 and Table 2. There were no significant differences in baseline RI values between the two sessions. The median (first, third quartile) RI values in the control session were 0.592 (0.563, 0.636) at baseline; 0.587 (0.562, 0.626) at post 1, and 0.583 (0.567, 0.629) at post 2, whereas those in the treatment session were 0.590 (0.550, 0.652), 0.565 (0.530, 0.618), and 0.561(0.533, 0.614), respectively. There were no statistically significant differences in RI values in the control session (p = 0.239), whereas the RI at post 1 (p < 0.001) and post 2 (p < 0.001) were significantly decreased from the baseline value in the treatment session. The reduction in RI from baseline to post 2 was significantly greater in the treatment session than in the control session (mean ± SD, −0.026 ± 0.028 versus −0.003 ± 0.028; mean difference, −0.023 [95% CI, −0.036 to −0.010]; p = 0.001) (Fig. 5). The changes in RI values from baseline to post 2 in the control-first group and treatment-first group are shown in Table 3. There were no significant period effects (p = 0.848) or carryover effects (p = 0.725).

Resistive index (RI) change in the control and treatment (moxibustion) sessions. The bottom and top of the box represent the 25th and 75th percentiles, and the line in the middle represents the 50th percentile (median). The whiskers (the lines that extend out the top and bottom of the box) represent the highest and lowest values within 1.5 times the interquartile range. The circles represent outliers. *p < 0.001 versus baseline.

Changes in RI from baseline to post 2 (10 minutes after end of moxibustion). Error bars indicate standard error. *p = 0.001 versus control.
Data are shown as median (first, third quartile) or mean ± standard deviation according to the distribution.
p = 0.001 versus baseline.
p = 0.002 versus baseline.
Post 1, immediately after completion of moxibustion; post 2, 10 minutes after completion of moxibustion; PSV, peak systolic velocity; EDV, end-diastolic velocity; MV, mean velocity.
Data expressed with a plus/minus sign are shown as mean ± standard deviation.
The changes in RI in treatment session according to subgroups (CKD stage and prescription of RASI) are shown in Figure 6A and 6B. RI at baseline in stage 3 and 4 was greater than that in stage 1 and 2. RI was significantly reduced from baseline to post 1 and post 2 in patients with all CKD stages. RI at baseline in patients with and without RASI was not significantly different. Moreover, a significant reduction in RI from baseline to post 1 and post 2 was also observed in both groups. The changes in RI from baseline to post 2 in treatment session by subgroup (prescription of RASI and CKD stage) are shown in Table 4. There were no significant differences in reduction of RI from baseline to post 2 between groups with RASI and without RASI (p = 0.542). There were also no significant differences between groups with CKD stage 1 or 2 and CKD stage 3 or 4 (p = 0.213).

Changes in RI in the treatment session.
Data are shown as mean ± standard deviation or median (first, third quartile) according to the distribution. The p-values are for between “RASI yes” and “RASI no” groups or between CKD stages 1 and 2 and stages 3 and 4.
PSV in the treatment session was slightly but significantly decreased from baseline to post 1 (p = 0.001) and post 2 (p = 0.002), whereas PSV in control session did not show any significant changes (Table 2). The changes in PSV from baseline to post 2 did not significantly differ between the two sessions (p = 0.360). Moreover, there were no significant differences in change in EDV and mean velocity from baseline to post 2 between the two sessions (p = 0.800 and p = 0.566, respectively).
Changes in physiologic variables are shown in Table 5. There were no significant differences in the values of systolic BP, diastolic BP, and mean BP at baseline, post 1, and post 2 between the two sessions. There were also no significant differences in changes from baseline to post 2 in systolic BP (95% CI, −3.6 to 4.0 mm Hg; p = 0.922), diastolic BP (95% CI, −4.7 to 4.2 mm Hg; p = 0.900), and mean BP (95% CI, −4.0 to 3.7 mm Hg; p = 0.950) between the two sessions. No statistically significant differences were detected in BT at baseline, post 1, and post 2 in both sessions or in BT changes from baseline to post 2 between two sessions (p = 0.379). HR was significantly decreased from baseline to post 1 and post 2 in both sessions, but the differences between the 2 sessions were not statistically significant (p = 0.238). There was also no significant difference in changes in HR from baseline to post 2 between the two sessions (95% CI, −5.2 to 1.3 beats/min; p = 0.231).
Data are shown as mean ± standard deviation or median (first, third quartile).
p = 0.002 versus baseline.
p < 0.001 versus baseline.
p = 0.026 versus baseline.
p = 0.004 versus baseline.
HR, heart rate; BT, body temperature.
Numbers of patients in each score of heat sensation were as follows: score 1, 0 patients; score 2, 9 patients; score 4, 15 patients; and score 5, 17 patients. Furthermore, numbers of patients in each score of comfort level were as follows: score 1, 5 patients; score 2, 13 patients; score 3, 7 patients; score 4, 15 patients; and score 5, 3 patients (Fig. 7A). A significant correlation between heat sensation and comfort level was observed (ρ = 0.652; p < 0.001). There was a significant negative correlation between heat sensation and changes in RI from baseline to post 2 (ρ = –0.40; p = 0.008) (Fig. 7B), but no such significant correlation between comfort level and RI change (ρ = −0.06; p = 0.695) was observed.

No adverse events, such as burn, pain, discomfort, or other problems requiring medical treatment or discontinuation of measurements, were observed during the study period.
Discussion
To the best of the authors' knowledge, this is the first report to use US to assess changes in intrarenal hemodynamics caused by indirect moxibustion in patients with CKD. The effects of indirect moxibustion are thought to be associated with hemodynamic changes in the kidney as vessel resistance in the renal segmental arteries was seen to decrease immediately and 10 minutes after the procedure in these patients.
Renal RI has been found to be a clinically important marker in renal disease. In the current study, RI in patients with severe CKD (stage 3 and 4) was higher than that in less severe CKD (stage 1 and 2). A high RI has been reported as a risk factor for progression of CKD, 4,5 and it was decreased by medical treatment in patients with chronic nephropathy or hypertension. 7 –10 Additionally, a high RI, proteinuria, low GFR, and hypertension were also reported as independent risk factors for CKD progression over 2- to 4-year follow-up periods. 4,5 Hemodynamic changes caused by RAS inhibitors have been reported to contribute partially to the antiproteinuric effect in patients with chronic proteinuria. 8 In these reports, the reduction in proteinuria was directly correlated with decrease in RI.
Leoncini et al. reported that angiotensin-converting enzyme inhibitors (ACEIs) decreased RI and urinary albumin excretion in patients with primary hypertension, but calcium-channel blockers did not have the same effects. 9 Delic-Brkljacic et al. reported that although both angiotensin II blockers and calcium-channel blockers decreased blood pressure, RI was decreased more significantly by the angiotensin II blocker (ARB). 10 They also suggested that RI measured in intrarenal arteries is the best parameter of the Doppler spectrum for evaluation of the effects of antihypertensive therapy on the kidney. It has been reported that RI was significantly improved by an ARB in the responder group of hypertensive patients whose microalbuminuria or proteinuria was decreased. 7 This suggested that an improvement in intrarenal hemodynamics may play an important role in the mechanisms underlying the renoprotective effect of ARBs. These reports suggest that changes in RI are associated with improvements in the functioning of the renin–angiotensin system and indicate that RI is an important parameter in assessing various treatments for renal disease.
Given these findings, intrarenal RI is a potential indicator for monitoring CKD progression, and a decrease in its value may be associated with therapeutic effects on kidney disease. In the current study, RI was decreased significantly 10 minutes after moxibustion. Therefore, indirect moxibustion treatment at BL 23 may have therapeutic effects in patients with renal disease by reversing harmful renal hemodynamic changes.
The present study demonstrated an RI reduction of 0.026 because of only short-term effects of indirect moxibustion. Some studies have reported approximately an RI reduction of 0.04–0.05 by repetitive RASI prescription, but these effects were due to long-term administration from approximately 1 week to 24 month. 7,9,10 There were few reports regarding short-term effects of RASI. Taniwaki et al demonstrated a RI reduction of approximately 0.01 at 1 hr after oral ACEI administration in diabetic patients. 29 The change of RI after moxibustion in the present study was greater than that by ACEIs in their report. However, to elucidate the clinical significance of the change in RI by indirect moxibustion, further study with long-term observation and measurements of clinical markers such as proteinuria must be performed.
Moreover, RI reduction in patients who underwent RASI administration suggests that indirect moxibustion therapy might be beneficial as an adjunctive therapy for conventional medication, such as RASI. 7 Renal hemodynamic changes following moxibustion are not associated with CKD severity because reduction in RI was observed irrespective of CKD stage in the current study.
Some reports have also demonstrated the effects of acupuncture and moxibustion on the blood flow in various organs using US. Local thermal stimulation of the abdomen was reported to increase superior mesenteric artery blood flow volume and decrease brachial artery blood flow volume. 15 Superior mesenteric artery blood flow volume was also increased by acupuncture stimulation at ST 36, which is used for abdominal symptoms in Traditional Chinese Medicine theory. 16,18 These changes in blood flow were suggested to result from changes in autonomic nervous activity. 15,16,30
Acupuncture and moxibustion treatment have been reported to alter renal function. 19 –23 Treatment using a combination of moxibustion at BL 23 and electric acupuncture stimulation at KI 3 and ST 36 was reported to improve functional and histopathological parameters, including renal sympathetic nerve activity in CKD model rats. 22,23 These findings suggest that these treatment measures have beneficial effects on renal disease by modulating renal sympathetic nerve activity, leading to decreased blood pressure, which, in turn, results in decreased proteinuria. The reduction in RI observed in this study may be due to autonomic nervous system modulation, although renal sympathetic nerve activity was not evaluated directly.
The significant correlation between heat sensation and changes in RI value suggest that heat sensation intensity may be associated with effect of moxibustion on renal hemodynamics.
Some limitations of this study must be considered. First, only short-term effects were observed in the current study, and long-term changes in RI and clinical effectiveness still remain unclear. Second, the specificity of the acupuncture point (BL 23) used in this study was also unclear, and stimulation of other acupuncture points or nonacupuncture points may have the same effect. Third, patients with diabetic nephropathy were not included in this study even though it is a common CKD type. Fourth, US measurements were not completed in all patients because of technical difficulties. Therefore, further studies with a longer observation period, measurement of clinical effect using biochemical marker (such as proteinuria) in patients with CKD, and a greater sample size that includes patients with various diseases is required.
Conclusion
This study measured the immediate effects of indirect moxibustion on renal hemodynamics using Doppler US. Renal vascular resistance was decreased after moxibustion treatment in patients with CKD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.