
Abstract
Objectives:
Equine-assisted activity and training (EAAT) is thought to improve body balance and clinical symptoms in children with attention deficit hyperactivity disorder (ADHD). The study hypostheses were that EAAT would improve the clinical symptoms and gait balance in children with ADHD and that these improvements would be associated with increased brain connectivity within the balance circuit.
Methods:
A total of 12 children with ADHD and 12 age- and sex-matched healthy control children were recruited. EAAT consisted of three training sessions, each 70 minutes long, once a week for 4 weeks. Brain functional connectivity was assessed by using functional magnetic resonance imaging.
Results:
After 4 weeks of EAAT, children with ADHD showed improved scores on the Korean ADHD scale (K-ARS), while the K-ARS scores of healthy children did not change. During the 4 weeks, the plantar pressure difference between the left foot and right foot decreased in both the healthy control group and the ADHD group. After 4 weeks of EAAT, healthy controls showed increased brain connectivity from the cerebellum to the left occipital lingual gyrus, fusiform gyrus, right and left thalami, right caudate, right precentral gyrus, and right superior frontal gyrus. However, children with ADHD showed increased brain connectivity from the cerebellum to the right insular cortex, right middle temporal gyrus, left superior temporal gyrus, and right precentral gyrus. In contrast, children with ADHD exhibited decreased brain connectivity from the cerebellum to the left inferior frontal gyrus.
Conclusion:
EAAT may improve clinical symptoms, gait balance, and brain connectivity, the last of which controls gait balance, in children with ADHD. However, children with ADHD who have deficits in the fronto-cerebellar tract did not exhibit changes in brain connectivity as extensive as those in healthy children in response to EAAT.
Introduction
A
Hippotherapy, a type of equine-assisted activity and therapy (EAAT), has been used to treat children or adults with neuromusculoskeletal or mental dysfunction. The American Hippotherapy Association was formed in 1992 and offers integrated therapy programs for physical therapists, physical therapist assistants, occupational therapists, occupational therapist assistants, and speech-language pathologists. Therapists use the repetitive, rhythmic movements of a horse and the handling and verbal cues to provide precisely graded motor and sensory input with the purpose of improving physical, occupational, and speech functions.
This therapy is thought to increase muscle strength, improve balance and body posture, and increase social and executive function in individuals with cerebral palsy or autism. 11,12 Patients with autism have shown improvement in physical, emotional, and social functions after 9 weeks of equine-assisted activities. 13 In addition, EAAT has also been an effective treatment for other psychiatric disabilities, including intellectual disabilities, 14 anxiety and posttraumatic stress disorder, 15 and language learning disabilities. 16 In addition, EAAT is effective in the sensorimotor, 17 neuromotor, 18 psychological, 19 and social domains. 20 Because horses provide unique neuromuscular stimulation in a rhythmic motion, this treatment promotes strength, balance, coordination, and flexibility by motor learning and sensory integration. 17 As a result of these effects, EAAT has been proposed as an alternative therapy for many other psychiatric diseases, including ADHD, 21 autism, 22 and schizophrenia. 23 In the context of ADHD, EAAT is expected to improve motor proficiency, physical activity, and postural balance by stimulating the sensorimotor domain.
The current study compared the effects of EAAT in children with ADHD and healthy children. The study hypotheses were that therapeutic horseback riding would improve the clinical symptoms and gait balance of children with ADHD and that these improvements in clinical symptoms and gait balance would be associated with increased brain connectivity within the balance circuit.
Materials and Methods
Participants
This study was designed in two phases. First, 13 children with ADHD and 13 age-and sex-matched healthy children were recruited to determine the extent of the correlations between step balance and various brain networks. Results of the analysis of balance from the first phase were previously reported. 24 Among the 13 children with ADHD and 13 healthy children, 7 with ADHD and 8 healthy children agreed to participate in the second phase of the study, which sought to determine whether EAAT improved balance.
During the second phase, 8 new children with ADHD and 6 new healthy children joined the study. Of the 15 children with ADHD, 1 had an intelligence quotient (IQ) less than 80 and one had comorbid depression. During the 4 weeks of EAAT, 1 child with ADHD and 2 control children were excluded because they missed more than 3 training sessions. All children were interviewed according to the Korean Kiddie Schedule for Affective Disorders and Schizophrenia, Present and Lifetime Version, 25 and were diagnosed by a child psychiatrist according to the criteria from the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Inclusion criteria for the ADHD group included (1) being medication-naive or drug-free for 6 months before the study, (2) IQ greater than 80, and (3) right-handedness. Exclusion criteria were (1) other psychiatric comorbidities, including depression, autism spectrum disorder, and tic disorder; (2) history of head trauma or substance abuse; and (3) contraindication for magnetic resonance imaging (MRI), including claustrophobia, metal implants, or cerebrovascular incidents. The same contraindications applied to the control children. Clinical symptoms of ADHD, balance, and brain activity were evaluated using clinical scales, gait balance testing, and resting state functional MRI (fMRI), respectively, at baseline and 4 weeks after EAAT. The research protocol was approved by the Gachon University Hospital Institutional Review Board. Written informed consent was provided by parents, and all children agreed to participate in the study.
EAAT
EAAT was conducted as a 4-week prospective trial. The study team for EAAT consisted of two psychiatrists, three specialists with the Professional Association of Therapeutic Horsemanship International, and four graduate teaching assistants majoring in sports science. The training sessions were 70 minutes each and were held three times per week. Training sessions adhered to the following schedule: 10 minutes to put on the safety harness (protector and helmet) and receive safety education; 10 minutes to care for the horse, including brushing and feeding; 40 minutes of EAAT; and 10 minutes for feedback and cooling down. The 12 sessions (S) of EAAT consisted of the following activities: S1: learning horse walking, S2: riding posture at walk and sitting trot, S3: rhythm of sitting trot, S4: changing direction (including half-volte to wall)/making small (10-m) circles, S5: half-seated posture with hands, S6: half-seated posture without hands, S7: diagonal posting trot in the ring arena, S8: posting and sitting trot in the ring arena, S9: diagonal posting trot in the ring arena, S10: making circles with posting and sitting trot in the small arena, S11: staying straight and changing direction by crossing the long diagonal in the small arena, and S12: figure-eight with posting trot in the small arena.
Brain analysis
Brain scans were obtained from all children by using a 3.0-Tesla Verio MRI scanner (Siemens, Erlangen, Germany). The functional imaging parameters were as follows: a gradient-echo planar sequence sensitive to blood oxygen level–dependent contrast (repetition time], 3000 milliseconds; echo time, 30 millisecond; flip angle, 90°), whole-brain volumes with 3.5-mm-thick transverse slices, a voxel size of 3.5 × 3.5 × 3.5 mm3, no interslice gap, and in-plane resolution of 64 × 64 pixels. Patients were asked to lie in the scanner with their eyes closed and to remain awake. For anatomic imaging, three-dimensional (3D) T1-weighted magnetization-prepared rapid gradient echo data were recorded with the following parameters: repetition time, 1900 milliseconds; echo time, 3.00 milliseconds; field of view, 256 × 256 mm2; 120 slices; and 1.0 × 1.0 × 1.0 mm3 voxel size. Images were realigned to Talairach coordinates by using the anterior and posterior commissures and the sagittal sulcus plane.
Brain Voyager software (BVQX 1.9; Brain Innovation, Maastricht, The Netherlands) was used for functional image analysis. Functional images were coregistered to the anatomic 3D image sets for each child by using the provided multiscale algorithms. The 3D structural images were spatially normalized to the standard Talairach space. 26 A nonlinear transformation was applied to the T2-weighted fMRI time series data. Slice scan time and 3D motion correction were applied, and the functional data were spatially smoothed by using a Gaussian kernel with a full width at half maximum of 6 mm. The smoothed data were temporally filtered using linear trend removal and Fourier analysis high-pass filtering with a cutoff of three cycles of the full time course.
Brain connectivity within the fronto-striatal-cerebellar circuit was measured by functional connectivity (FC) analysis using resting-state fMRI data. FC analysis measures the temporal association between two brain areas that are spatially isolated. In addition, FC analysis reveals neural circuitry by identifying brain regions that share similar functional properties. 27 FC from the vermis (Talairach coordinates 0, −68, −16) of the cerebellum to all other regions of the brain was assessed by drawing a 10-mm cube on each side. To ensure the reliability of the fMRI analysis, data from children with excessive head movement (>3 mm in length along the x, y, or z dimension or >3° rotation around the x, y, or z axis) were to be excluded. However, no children exhibited excessive head movement.
Gait balance
Gait balance was assessed with two scales. The difference in the center of pressure (COP) between the left foot and right foot and the difference in plantar pressure between the left foot and right foot during gait were measured. A MatScan® system floor mat (Tekscan, Boston, MA) was used to measure the pressure exerted by each foot. This mat was 5 mm thick (432 × 368 mm) with 2288 resistive sensors (1.4 sensors/cm2) and had a sampling frequency of 40 Hz. To avoid intentional weight-bearing on the floor mat, children were asked to squat twice for 10 seconds. During these 10 seconds, an estimated COP value was obtained, but only the COP within the last second (50 frames) was recorded for analysis. The smoothness of the COP trajectory in the antero-posterior to mediolateral direction within the foot was quantified using normalized jerk scores during gait. 28
To obtain the dynamic plantar pressure during constant gait velocity, a two-step gait protocol was used. 29 For 5 minutes, children were familiarized with walking over the floor mat. Data were collected at a natural gait pattern with a self-selected speed. The peak pressure (kPa) within seven regions of the foot (lateral heel, medial heel, midfoot, first metatarsophalangeal joint, second to fifth metatarsophalangeal joint, hallux, and lesser toes) 30 was obtained, and the average peak pressure of each foot was obtained. The average peak pressure and the temporal measurements of the pressure-time integrals (kPa·s/cm2) were recorded for analysis.
Statistical analysis
Demographic characteristics of the ADHD group and healthy group were compared with the Mann–Whitney U test and chi-square test. In both groups, the changes in brain connectivity over the 4 weeks were assessed by using a paired t-test. (Statistical Package for the Social Sciences [SPSS] software package version 18.0, IBM, Seoul, Korea). In the brain analyses, associations were regarded as significant when the false discovery rate (FDR) correction was 0.05 or less or the uncorrected p-value was 0.0001 or less. (BVQX 1.9; Brain Innovation, Maastricht, the Netherlands).
Results
Demographic and clinical data
No significant differences were observed between children with ADHD and healthy children in age, sex, education, IQ, or Children's Depressive Inventory score (Table 1). However, the mean K-ARS score for children with ADHD was higher than that for healthy children (z = 4.12; p < 0.01).
Unless otherwise noted, values are expressed as mean ± standard deviation.
Statistically significant.
ADHD, attention deficit hyperactivity disorder; IQ, intelligence quotient; K-ARS: Korean version of the Attention Deficit Hyperactivity Disorder Scale; RANOVA, repeated-measures analysis of variance; MS, mean square; CDI, Children's Depressive Inventory.
Changes in clinical symptoms
After 4 weeks of EAAT, children with ADHD showed improved K-ARS score (z = 3.18; p < 0.01), while the K-ARS score of healthy children did not change (Table 1). Children with ADHD (z = 2.84; p < 0.01) and healthy children (z = 3.02; p < 0.01) both showed improved depression scores. However, the changes in depressive mood were not significantly different between the two groups.
Changes in balance
The baseline plantar pressure difference between the left and right feet in children with ADHD was larger than in healthy children (z = 2.71; p < 0.01). The baseline COP jerk score within the right foot of children with ADHD was greater than in healthy children (z = 2.02; p = 0.04) (Table 2).
Unless otherwise noted, values are expressed as mean ± standard deviation.
Statistically significant.
COP, center of pressure.
During the 4-week EAAT period, the plantar pressure difference between the left foot and right foot decreased in both the healthy control group (z = 2.24; p = 0.03) and the ADHD group (z = 2.28; p = 0.02). Moreover, no significant difference was observed between the two groups (F = 1.23; mean square (MS) = 1.76, p = 0.28). During the 4-week EAAT period, the COP jerk scores of both the left (z = 1.41; p = 0.16) and the right (z = 9.8; p = 0.33) feet in the healthy control group did not change. However, the COP jerk scores of both the left (z = 2.6; p = 0.01) and the right (z = 2.5; p = 0.01) feet in the ADHD group decreased (Fig. 1).
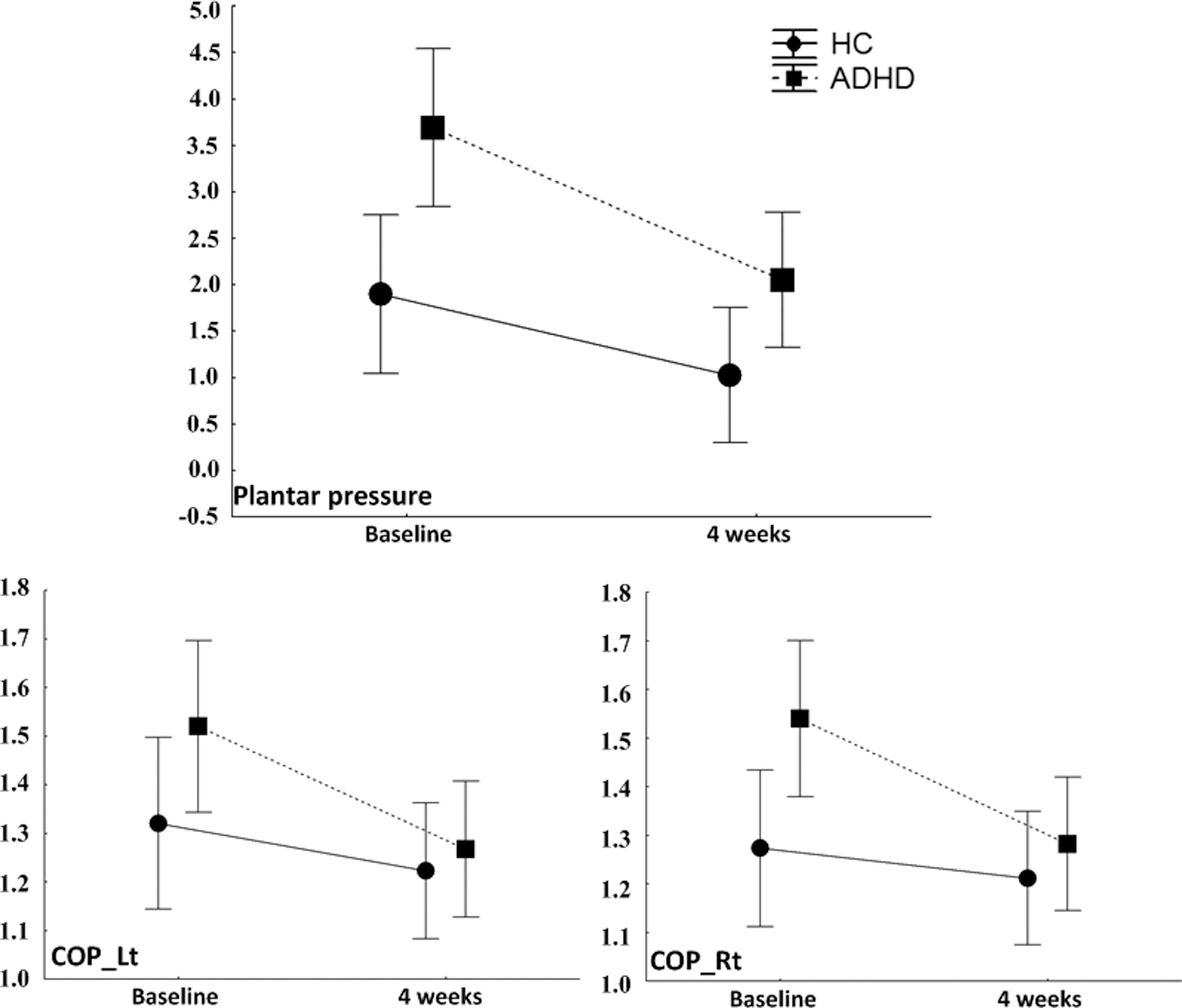
Changes in balance after the 4 weeks of horse riding and training. ADHD, attention deficit hyperactivity disorder; COP, center of pressure; HC, healthy control; Lt, left; Rt, right.
Changes in brain connectivity after horse riding training
After 4 weeks of EAAT, healthy control children showed increased brain connectivity from the cerebellum to the left occipital lingual gyrus, fusiform gyrus, right and left thalami, right caudate, right precentral gyrus, and right superior frontal gyrus (Fig. 2, Table 3). Children with ADHD also showed increased brain connectivity from the cerebellum to the right insular cortex, right middle temporal gyrus, left superior temporal gyrus, and right precentral gyrus; however, they showed decreased brain connectivity from the cerebellum to the left inferior frontal gyrus (Fig. 2, Table 3). Compared with children with ADHD, healthy children showed higher functional connectivity from the cerebellum to the left precentral gyrus (−44, −10, 25; voxel = 40; FDR p < 0.05 = 0.03) and the postcentral gyrus (−44, −18, 32; voxel = 40; FDR p < 0.05 = 0.03) (Fig. 2).
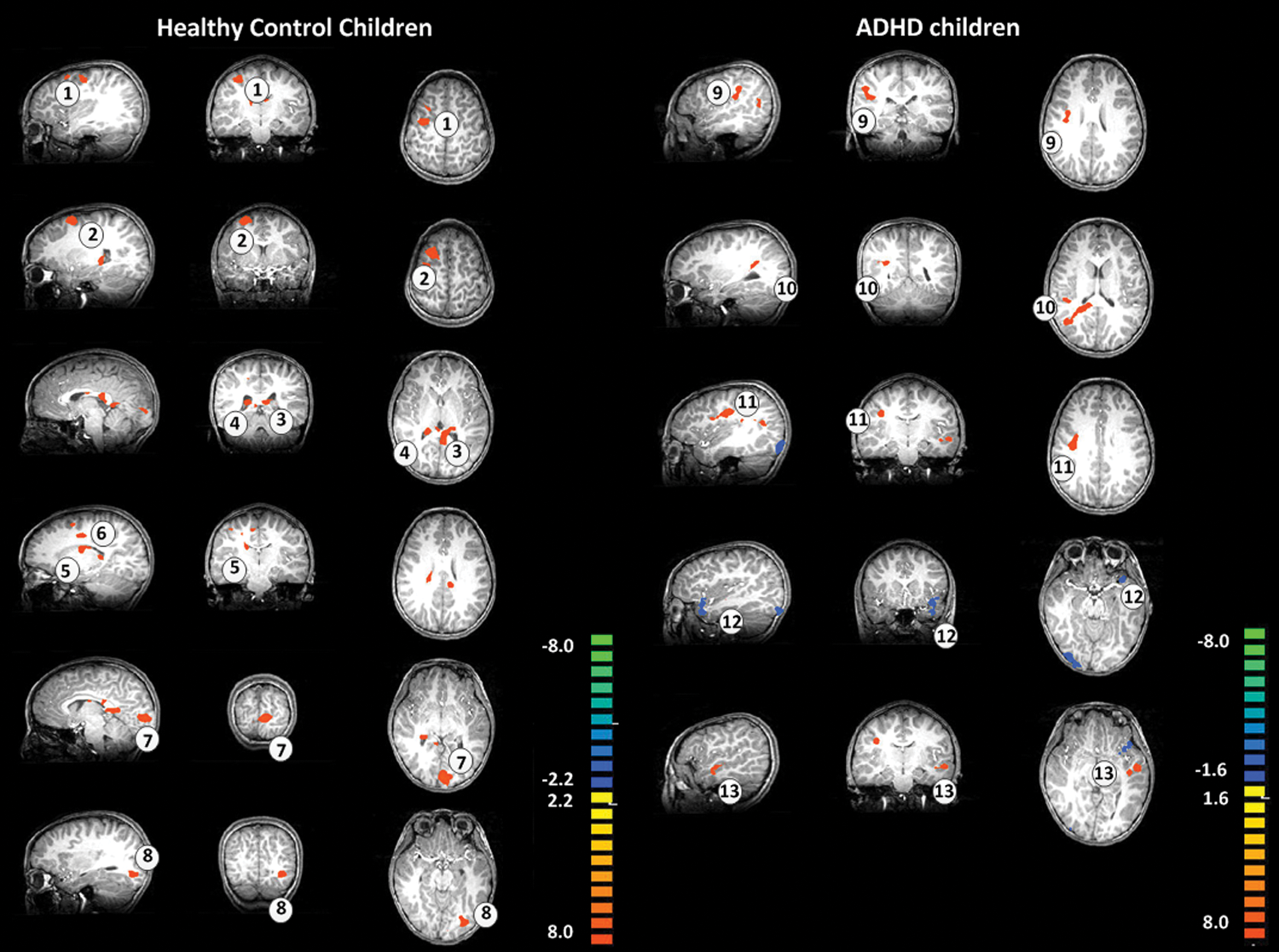
Changes in brain connectivity after the 4 weeks of horse riding training. Color images available online at
FDR, false discovery rate; BA, Brodmann area.
The brain activity changes within the left precentral gyrus from baseline to 4 weeks were negatively correlated with right COP jerk score change (r = −0.72; p < 0.01) in children with ADHD. However, no significant correlation was observed between the left COP and brain activity within the precentral and postcentral gyri.
Discussion
In the present study, clinical symptoms and gait balance were both improved in children with ADHD after 4 weeks of EAAT. Moreover, brain functional connectivity was increased in children with ADHD and in healthy children. However, healthy children showed greater brain connectivity changes from the cerebellum to the frontal cortex compared with children with ADHD.
Changes in clinical symptoms
Several reports have indicated that horse riding improves clinical symptoms in children with ADHD. In a pilot study of 5 children with ADHD, Cuypers et al. observed that 8 weeks of therapeutic horseback riding had positive effects on social behavior, life quality, and motor performance. 21 Jang et al. also reported that 12 weeks of EAAT improved the K-ARS inattention score and the Korean version of the Child Behavior Checklist social problems subscale score in 20 children with ADHD. 31 In the present study, 4 weeks of EAAT improved the clinical symptoms of ADHD and depressive mood in children with ADHD. Frederick et al. suggested that equine-assisted learning increases hope and improves depression in at-risk adolescents. 32 Moreover, therapeutic horse riding was reported to improve cognitive, affective, and behavioral signs of depression in children with dysrexia. 33
Changes in gait balance
In the current study, 4 weeks of EAAT reduced the plantar pressure difference between the left foot and right foot in both the healthy and ADHD groups. However, the COP jerk score was improved only in the ADHD group. Several studies have concluded that participating in horse riding programs improves motor proficiency and body balance. For example, Pan et al. reported that a 12-week horse riding program combined with fitness training improved motor proficiency, cardiovascular fitness, and body flexibility in children with ADHD. 34 Asselin et al. concluded that therapeutic horseback riding improved balance, muscle strength, and self-esteem in a patient with a spinal cord injury. 35 When gait was measured by the 10-m walk test and balance was tested with the Modified Barthel Index, stroke patients who participated in 6 weeks of EAAT exhibited significant improvement in balance and gait compared with stroke patients who did not participate in HRT. 36 In EAAT, the rhythmic and repetitive movement of the horse is thought to stimulate motor neurons and enhance input information to the motor system, similar to the movement patterns of the pelvis when walking. 37,38 In addition, trunk muscle movement, proprioception enhancement, and vestibular functions are regarded as important factors for improving balance during HRT. 39,40
Changes in brain functions
After 4 weeks of EAAT, both the healthy control and ADHD groups showed increased brain connectivity from the cerebellum and the precentral and frontal cortices. These results are consistent with a previous study of brain function in children with ADHD who participated in EAAT. 31 Moreover, 12 weeks of equine-assisted therapy decreased the electroencephalography theta/beta ratio in children with ADHD. 31 Lee et al. reported that 32 weeks of horse riding increased the activity within the cerebellum in patients with ADHD. 41 However, in contrast to the study by Lee and colleagues, which only compared brain activity within the insular cortex and the cerebellum, 41 the current study assessed the changes in brain connectivity from the cerebellum to many other brain regions.
In this study, healthy controls showed increased brain connectivity from the cerebellum to the occipital lobe, thalamus, and prefrontal cortex, while the ADHD group showed increased brain connectivity from the cerebellum to the insular cortex, temporal lobe, and precentral gyrus. In summary, healthy children showed higher functional connectivity from the cerebellum to the precentral gyrus and postcentral gyrus compared with children with ADHD after 4 weeks of EAAT. These differences may be due to the brain pathology of ADHD. It has been proposed that children with ADHD have impaired functional connectivity from the cerebellum to the cerebrum (fronto-cerebellar dissociation). 42,43 This finding of impaired functional connectivity is consistent with recent studies on poor motor response inhibition and motor timing during higher-order motor control in children with ADHD. 44 –46 Decreased connectivity between the prefrontal cortex—the planning and decision-making center—and the premotor/motor system in children with ADHD might cause neuropsychological deficits leading to the core symptoms of ADHD. 44 –46
The present results also indicate that the ADHD group showed increased brain connectivity from the cerebellum to the temporal gyrus and precentral gyrus after 4 weeks of EAAT. In the fMRI study on ADHD conducted by Vaidya et al., the administration of methylphenidate increased striatal activation in ADHD children with atypical frontal-striatal function. 47 Beauregard et al. investigated the therapeutic effects of neurofeedback training on ADHD children during a go/no-go task and Stroop task. After a 14-week neurofeedback treatment, performance improved for both tasks, and hypoactivation of the frontal-striatal network was normalized in the right ventrolateral prefrontal cortex, right anterior cingulate cortex, left thalamus, left caudate nucleus, and left substantia nigra in the treated group. 48 In another recent study, aerobic exercise treatment increased the effectiveness of methylphenidate and increased brain activity within the right fronto-temporal region in ADHD children. 49 We suggest that EAAT improves connectivity within the fronto-striato-cerebellum in ADHD children, like other treatments including medication, neurofeedback, and aerobic exercise.
Interestingly, the COP jerk scores of the left and right feet were improved only in the ADHD group. Moreover, increased brain activity within the precentral gyrus was associated with improved balance in children with ADHD. We hypothesized that horse riding stimulation improves gait balance. However, the short training period (4 weeks) used in the present study appears to be insufficient to change the brain connectivity of the whole balance tract in children with ADHD.
Limitations
The current study has several limitations. First, the small number of participants and relatively short research period limited the extent to which its results can be generalized. Second, this study did not assess any changes in cognitive function in response to EAAT. Future studies should have large numbers of participants and assess the correlations between cognitive function and brain changes in response to horse riding.
Conclusions
EAAT may improve clinical symptoms, gait balance, and brain connectivity, the last of which controls gait balance, in children with ADHD. However, children with ADHD who have deficits in the fronto-cerebellar tract did not exhibit changes in brain connectivity as extensive as those in healthy children in response to EAAT.
Footnotes
Acknowledgments
This study was supported by the Korea Creative Content Agency (grant no. R2014040055) and Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A120013).
Author Disclosure Statement
No competing financial interests exist.