
Abstract
Purpose:
Medical students have higher rates of depression and psychologic distress than the general population, which may negatively impact academic performance and professional conduct. This study assessed whether 10–20 min of daily mindfulness meditation for 30 days, using a mobile phone application, could decrease perceived stress and improve well-being for medical students.
Methods:
Eighty-eight medical students were stratified by class year and randomized to either intervention or control groups to use the mobile application Headspace, an audio-guided mindfulness meditation program, for 30 days. All participants completed the Perceived Stress Scale (PSS), Five-Facet Mindfulness Questionnaire (FFMQ), and General Well-Being Schedule (GWBS) at baseline (T1), 30 days (T2), and 60 days (T3). Repeated measures analysis of variance (rANOVA) was conducted for intervention versus control groups across T1, T2, and T3 to examine differences in stress, mindfulness, and well-being.
Results:
There was a significant interaction between time and treatment group for perceived stress and well-being. Perceived stress significantly decreased for the intervention group from T1 to T3 (F[2,142] = 3.98, p < 0.05). General well-being significantly increased for the intervention group compared to the control group from T1 to T2, and the increase was sustained through T3 (F[2,144] = 3.36, p < 0.05).
Conclusions:
These results highlight that a mobile audio-guided mindfulness meditation program is an effective means to decrease perceived stress in medical students, which may have implications on patient care. Integrating mindfulness training into medical school curricula for management of school- and work-related stress may lead to fewer negative physician outcomes (e.g., burnout, anxiety, and depression) and improved physician and patient outcomes. This has implications for a broad group of therapists and healthcare providers, ultimately improving quality of healing and patient care.
Introduction
M
This trend continues into later years of training 12,15 and resembles similar reports on physicians. 16 –18 Shanafelt et al. 18 found that U.S. physicians are more likely to have symptoms of burnout and job dissatisfaction compared to other working individuals in the general population. The implications of physician burnout include decreased productivity, higher rates of depression and substance abuse, and depersonalization associated with longer patient recovery time and lower patient satisfaction. 14,18 –20 To combat these negative effects, mindfulness-based practices have demonstrated favorable outcomes on stress reduction. 11,21 –25
Mindfulness-based exercises focus on reducing reactivity to challenging experiences through purposeful and nonjudgmental self-awareness of physical sensations, cognitions, and emotions. 26 Jon Kabat-Zinn originally designed Mindfulness-Based Stress Reduction (MBSR) as a behavioral medicine program for the management of chronic pain. 25,27 Since its introduction, the technique has been useful for the treatment of anxiety and a broad spectrum of other disorders. 25,28
A number of medical schools have implemented various strategies to promote self-care and awareness of mental health problems. 24,25,29,30 At Jefferson Medical College, medical students participated in 10 weeks of a 1.5-h weekly MBSR seminar and were provided with an audiocassette for 20 min of daily meditation practice on their own. 21 At the University of Tasmania, students received an audio CD to practice mindfulness independently for 30 min each day for 8 weeks. 23 Both of these studies demonstrated significant and sustained reductions in stress levels, at the end of the 10-week intervention at Jefferson Medical College and at both 8 weeks postintervention and at 16 weeks follow-up at the University of Tasmania, in their target populations. These results show promise for the utility of MBSR and other mindfulness based interventions among medical students.
MBSR, as it was conceived by Jon Kabat-Zinn, traditionally consists of 26 h of training time, including eight weekly 2.5-h class meetings and one all-day class. In addition, students are given audiocassettes with recordings of guided meditation for individual practice throughout the week. 28,31 The goal is for participants to study the principles of self-regulation through mindfulness and develop the skill of practicing mindfulness independently. However, the length of the course may exclude some populations from participating in this standard format. Subsequent studies have modified the traditional MBSR format with fewer in-class hours and found that abbreviated adaptations may be worthwhile for those who are seeking stress reduction but cannot commit to a lengthy program. 31
The purpose of the present study was to determine the feasibility, efficacy, and effectiveness of a 30-day mindfulness meditation program for stress reduction among medical students at Keck School of Medicine at the University of Southern California (USC). The authors also sought to assess the utility of a mobile phone application as a delivery method for this training, which to date has never been studied in a randomized controlled manner. 32 To their knowledge, this is the first study to utilize mobile phone technology for implementation of stress reduction tools for medical students. Considering the time constraints of the medical school curriculum, the authors explored a means of delivery that would allow students to customize mindfulness training to their individual schedules.
Methods
This was a prospective, randomized controlled trial approved by the USC Institutional Review Board with both an intention-to-treat and a per-protocol analysis. The recruitment strategy is depicted in Figure 1. All medical students (716) at the Keck School of Medicine of USC were recruited by e-mail to participate in the study. Ninety-seven (97) students responded to the initial interest e-mail, seven (7) subsequently declined to participate, and two (2) were excluded due to not having a smartphone. A total of eighty-eight (88) students ultimately enrolled in the study. Informed consent was obtained by provision of study information sheet and voluntary selection.

Consort diagram.
Participants were stratified by year in medical school to account for differences in examination scheduling and randomized using a computer-generated randomization program to either an intervention group or a waitlist control group. Participants received access to the mobile application and links to online surveys through e-mail. Both groups completed baseline (T1) questionnaires on Qualtrics, an online survey system, including demographics, Perceived Stress Scale (PSS), Five-Facet Mindfulness Questionnaire (FFMQ), General Well-Being Schedule (GWBS), and additional open-ended questions, to evaluate sources of stress, coping strategies, and current and past exposure to meditation and other forms of alternative therapies.
The intervention group was asked to download the smartphone application Headspace, an audio-guided mindfulness meditation program. Headspace is a monthly digital subscription service that their participants accessed for free using 3-month subscription codes provided by the company for research purposes upon request. Its founder, Andy Puddicombe, developed the program by drawing from his personal experiences with meditation, as well as clinical and translational research that has found mindfulness to aid in stress reduction, improving life satisfaction, increasing focus, and modifying self-control. 33,34
The investigators of the current study adopted Headspace as the primary intervention following meetings and discussions with the Headspace leadership. Given that the principles behind Headspace's mindfulness program were well aligned with the techniques and goals of traditional MBSR and those of the abbreviated adaptations of mindfulness training that have been previously tested among medical students, this smartphone application appeared to be the best match. Furthermore, the mobile format was selected to provide flexibility such that participants could individually choose when and where they meditated each day.
The mindfulness training program is structured such that each session lasts 10 min for the first 10 days, 15 min for the next 15 days, and 20 min for all subsequent sessions. Each session consists of gentle audio-guided prompts for users to follow while seated comfortably. Instructions that range from taking notice of the body at rest, breathing with intention, and breathing normally to noticing sounds, sensing emotions, and acknowledging thoughts without assigning judgment are delivered in a calm manner with intermittent breaks in audio.
The intervention group was asked to use the application daily, or as much as possible, for 30 days. All questionnaires were completed again at the 30-day time point (T2). The intervention group was asked to keep a log of the number of minutes that they used the app, using a calendar provided by the authors. They were also asked to send a screen shot of a report within Headspace that tracks users' minute progress. Intervention participants continued to have access to Headspace after the initial 30-day period to use as desired, but were not explicitly told to use it. A final set of questionnaires were administered at the 60-day time point (T3) to assess whether participants continued to use the application on their own and whether any initial changes in the stated outcomes were maintained.
The control group completed all questionnaires at the same time points as the intervention group. They were placed on a waiting list to receive Headspace subscription codes at the 60-day time point (T3) at the conclusion of the study.
Measures
Stress
The 10-item PSS 35 is a brief self-reported measure of stress. It is a widely used psychologic instrument for measuring perceived stress, which is defined as the extent to which persons perceive that their demands exceed their ability to cope. 35 It is a measure of the degree to which situations in one's life are appraised as stressful. It was designed for use with community samples of at least junior high school education. Internal consistency at T1 was good (α = 0.85).
Mindfulness
The FFMQ 36,37 is a 39-item self-reported questionnaire based on research assessing mindfulness as five components: observing, describing, acting with awareness, nonjudging of inner experience, and nonreactivity to inner experience. Observing includes noticing or attending to internal and external experiences, such as sensations, cognitions, emotions, sights, sounds, and smells (eight items). Describing refers to labeling internal experiences with words (eight items). Acting with awareness includes attending to one's activities of the moment and can be contrasted with behaving mechanically while attention is focused elsewhere, often called autopilot (eight items). Nonjudging of inner experience refers to taking a nonevaluative stance toward thoughts and feelings (eight items). Nonreactivity to inner experience is the tendency to allow thoughts and feelings to come and go without getting caught up in or carried away by them (seven items). These five facets were bound together in a factor analytic study to develop the FFMQ. Taken together, the five facets have been shown to be significantly related to the meditation experience and to have a negative relationship with psychologic symptoms related to depression, anxiety, anhedonia, and insomnia. 36,37 Internal consistency at T1 was excellent (α = 0.91).
Well-being
The General Well-Being Schedule (GWBS) 38 is a self-reported 18-item questionnaire designed to measure subjective feelings of psychologic well-being and distress, including dimensions of anxiety, depression, general health, positive well-being, self-control, and vitality. Once scored, results are categorized as positive well-being, low positive, marginal, stress problem, distress, serious, or severe. 39 The scale was developed for the U.S. Health and Nutrition Examination Survey (HANES), with reference standards derived from the HANES data (in which 71% of the adult population fell into the positive well-being category). 38 At baseline, 80 (93%) respondents in this study were stressed, 4 (5%) were in a state of distress, and 2 (2%) were marginally stressed (Fig. 2). The authors elected to include this survey because inspiration for the present study originated from GWBS survey data presented of their first year medical school class. The GWBS has been reported as having high internal consistency and there is wide evidence of agreement with other depression and anxiety scales. 38 Internal consistency at T1 was excellent (α = 0.93).

Baseline general well-being score.
Statistical analysis plan
All statistical analyses were conducted using SPSS Version 21. Independent-samples t tests were conducted to determine baseline differences between groups on all measures. Repeated measures analysis of variance (rANOVA) analyses were conducted for “intention-to-treat” intervention group versus control across T1, T2, and T3. An additional subset analysis was performed in which those in the “intention-to-treat” group who never used the intervention based on self-report and a screen shot of the progress minutes as reported in the mobile app were removed from the analysis. The remaining group that used the intervention at least once “per-protocol” was compared separately to the control group. The purpose of separating these two groups when comparing to the control group was to examine the effectiveness and the efficacy of the mobile application separately, using the “intention-to-treat” and “per-protocol” designations, respectively. A p-value of <0.05 was considered statistically significant.
Results
Of the 88 medical students who participated, 32 (36%) were male and 56 (64%) were female. Other demographic information is presented in Table 1. Not all participants who were enrolled at T1 completed questionnaires at T2 and T3. At T2, 81 (92%) of the original 88 participants completed the questionnaires. At T3, 82 (93%) of the original 88 participants completed questionnaires. If there were two data points available (i.e., T1 and at least one other of T2 and/or T3), their data were included in the analyses. At the conclusion of the study, the authors found that 27 (60%) members of the intention-to-treat group actually used the Headspace application at least one time during the 30-day intervention period. The mean number of days of use was 11.97 (SD = 7.76, Range 0–28). Of the 27 that used the application during the 30-day intervention period, 20 (74%) participants continued to use it on their own during the subsequent postintervention period.
Parent's highest level of education used as a proxy for socioeconomic status.
Stressful experiences
Participants were asked “Has your life become more stressful since the beginning of medical school?” (yes or no) and to follow up, “In what ways has your life become more stressful since the beginning of medical school?” Seventy-three (83%) of their participants self-reported that life became more stressful since starting medical school, such as experiencing depressive symptoms, anxiety symptoms, relationship stress, less sleep, constant pressure, financial stress, lack of personal time, lack of self-confidence, less time for exercise, no longer top of class, eating and cooking less, weight changes, and time management stress.
Descriptives among variables
A table with the means and standard deviations (SD) for each outcome at each time point has been provided (Table 2). When examining outcome measures, t test results revealed that there were no significant differences between intention-to-treat and control groups at baseline on all dependent variables: stress (t[83] = −0.38, p = 0.70); well-being (t[84] = 0.24, p = 0.81) and all five subscales of mindfulness: (1) observing (t[82] = 0.59, p = 0.56), (2) describing (t[82] = 0.46, p = 0.64), (3) acting with awareness (t[82] = 0.17, p = 0.87), (4) nonjudging of inner experience (t[82] = 1.42, p = 0.16), and (5) nonreactivity to inner experience (t[82] = −0.80, p = 0.42).
Intent-to-treat findings: perceived stress
Results from the intention-to-treat ANOVA for the outcome of perceived stress found no significant main effects for condition F(1,71) = 0.002, p = 0.96 and time F(2,142) = 2.38, p = 0.10, but a significant interaction between time and condition: F(2,142) = 3.98, p = 0.02 (Fig. 3).

Changes in perceived stress across study period.
Intent-to-treat findings: mindfulness
There was a significant main effect of condition, as measured by FFMQ. Mindfulness increased for both groups from T1 to T3 for three subscales: observing (F[2,140] = 6.33, p = 0.02), acting with awareness (F[2,138] = 4.29, p = 0.02), and nonreactivity to inner experience (F[2,138] = 11.45, p < 0.01). The last two subscales evidenced insignificant findings for (1) describing: main effect of condition F(1,70) = 0.002, p = 0.96, main effect of time F(2,140) = 0.74, p = 0.48, and interaction F(2,140) = 1.15, p = 0.32; (2) acting with awareness: main effect of condition F(1,69) = 0.01, p = 0.91 and interaction F(2,140) = 0.58, p = 0.56; and (3) nonjudging of inner experience: main effect of condition F(1,70) = 1.02, p = 0.32, main effect of time F(2,140) = 2.826, p = 0.06, and interaction F(2,140) = 2.96, p = 0.06.
Intent-to-treat findings: well-being
There were significant main effects of time (F[2,144] = 3.95, p = 0.02), but no main effect of condition (F[1,72] = 0.09, p = 0.77) on well-being, as measured by the GWBS scale. However, there was a significant interaction between time and condition on well-being, where the intervention group had significant increases in well-being at T2, which was maintained through T3, compared to the control group over time, F(2,144) = 3.36, p = 0.04 (Fig. 4).
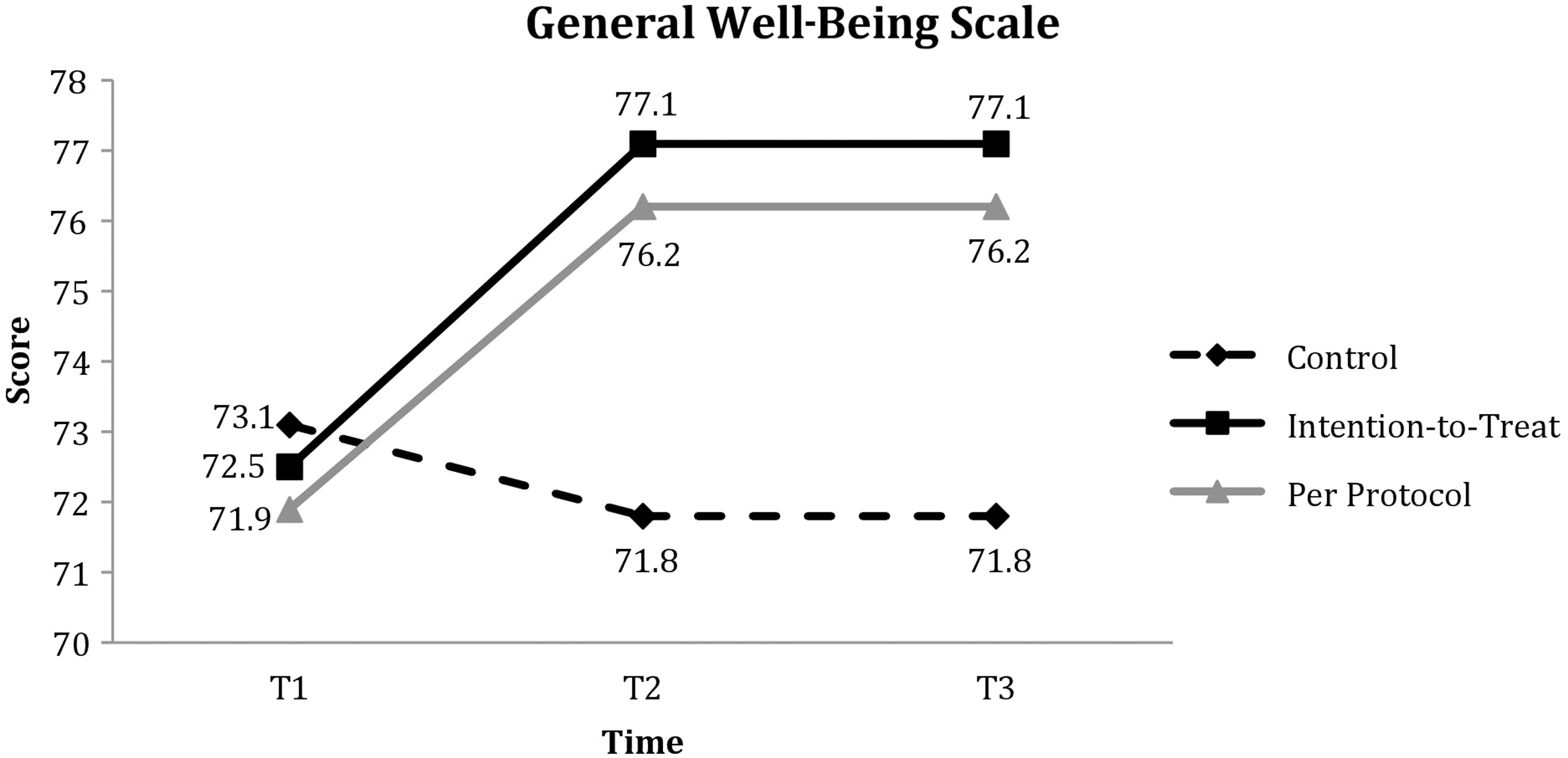
Changes in general well-being across study period.
Per-protocol findings: perceived stress
The per-protocol subset analysis of intention-to-treat group that used the intervention at least one time (n = 27) also showed decreased stress levels according to PSS compared to control, with a greater effect size. There was a significant main effect of time F(2,60) = 3.39, p = 0.04, but not condition F(1,61) = 0.26, p = 0.61. However, there was a significant interaction between condition and time F(2,60) = 4.35, p = 0.02.
Per-protocol findings: well-being
GWBS showed a trending interaction; there was an improvement in well-being in the per-protocol group over time F(2,124) = 2.83, p = 0.06. There were significant main effects of time F(2, 124) = 3.81, p = 0.03 and no main effect of condition, F(1, 62) = 0.44, p = 0.51.
Per-protocol findings: mindfulness
The observing subscale of FFMQ increased significantly in the per-protocol group but not the control group. Similarly to the findings on stress, there were significant main effects of time F(2,59) = 12.05, p < 0.01, but not condition F(1,60) = 0.39, p = 0.53. And there was a significant interaction between condition and time F(2,59) = 6.62, p < 0.01. Two subscales: Nonreactivity to inner experience and Acting with awareness had a significant main effect of time, where for both conditions, this increased from T1 to T3: Nonreactivity to inner experience subscale main effect of condition F(1,60) = 0.19, p = 0.66, main effect of time F(2,59) = 10.27, p < 0.01, and interaction F(2,59) = 0.67, p = 0.52. Acting with awareness main effect of condition F(1,60) = 0.06, p = 0.81, main effect of time F(2,59) = 3.28, p = 0.04, and interaction F(2,59) = 0.19, p = 0.83. The other two subscales showed no significant differences: (1) Describing main effect of condition F(1,60) = 0.10, p = 0.75, main effect of time F(2,59) = 0.89, p = 0.42, and interaction F(2,59) = 1.51, p = 0.23; (2) Nonjudging of inner experience subscale main effect of condition F(1,60) = −0.24, p = 0.62, main effect of time F(2,59) = 2.99, p = 0.06, and interaction F(2,59) = 3.11, p = 0.05.
Discussion
The purpose of this study was to examine the feasibility, efficacy, and effectiveness of a mobile phone application for meditation in medical students. The current findings support that such an intervention can significantly decrease stress and improve well-being for medical students.
Medical school is a critical period of personal growth and development, as students become leaders in promoting health and caring for the ill. 2,40 This ideal is highly discordant with experiencing significant psychologic distress. 2 Although medical training is challenging, students should find fulfillment and healthy methods to cope with the stressors in their future career. Several studies found first year medical students to be more depressed at the end of their first year than at the beginning, suggesting a need for early intervention in medical training. 1,41
Given the extensive time requirements of the medical school curriculum, an MBSR program with fewer time requirements may be even more beneficial. In our study using a brief meditation period of 30 days, perceived stress significantly decreased and well-being showed a significant increase among the intervention group but not the control that was sustained through the postintervention period in the intent-to-treat group. These findings indicate that brief mindfulness training through a mobile phone application format can be an effective means of reducing stress and promoting well-being in medical school.
Only the observing subscale of the FFMQ showed a significant increase relative to controls in the per-protocol group. This suggests that one's ability to take a virtual step back from their immediate situation to observe their internal and external environment with more space and awareness, as mindfulness training teaches, may be tied to one's perception of their stress. Interestingly, in a study on the construct validity of FFMQ, the observing facet was unexpectedly found to be positively related to thought suppression while having a negative association with alexithymia. 42 Perhaps perceived stress can be lowered by training subjects to suppress unwanted thoughts while maintaining the ability to identify and describe emotions. However, given that the other subscale scores on the FFMQ did not increase relative to the control group, it cannot be concluded that increases in mindfulness are related to decreases in perceived stress and increases in well-being as observed in the intervention group.
Although 84 (98%) participants were in a state of stress or distress at baseline with an apparent motivation to learn meditation, only 27 (60%) of the intervention group downloaded the application and used it at least one time. This discrepancy indicates that intention did not necessarily translate into action for some participants and that the mobile application format or the reality of taking up to 20 min each day to meditate may not have been as agreeable with a medical school schedule as the authors had considered. Several medical student participants reported that they wanted to use the app more than they actually did.
The study was designed such that once the download instructions and subscription codes were provided, no further contact was made with the participants until the 30-day time point. Thus, the authors did not remind participants to download the application or check to see if they had started using it. The purpose of this design was to see whether motivation was strong enough for students to follow through with the intervention on their own, without any reminders or outside accountability.
For those who did try the intervention at least one time, the mean number of days of use was 11.97, which indicates that those who did try the application continued to use it frequently throughout the month, even without reminders or ongoing accountability. This may indicate that once users overcame the initial time investment of setting up their Headspace account online and downloading and learning how to use the application, they were likely to continue using it. It is possible that some sort of personal contact, such as a reminder or check-in e-mail a few days after the beginning of the intervention period, may have motivated more students to put in that initial investment.
Of the participants who did use the application during the initial 30-day intervention period, 20 (74%) continued to use it in the subsequent 30 days of their own accord. This may indicate that the majority of those who did try the program found it to be a beneficial and feasible addition to their daily lives.
Limitations of this study include selection bias and response bias due to self-report questionnaires. Only 14% of medical students at Keck participated in this study, and study participants were more likely to be experiencing high stress levels and therefore more willing to volunteer for a program that could potentially help them. In addition, the intervention period was shorter compared with previous studies. The mobile application may have been effective for greater stress reduction or other significant findings given a longer duration of intervention or given increased engagement with the app during the intervention period. This remains an area for further investigation, and future studies may implement a longer intervention period with multiple medical schools to elucidate the utility of mobile technology for stress reduction in the general medical student population.
Since the conclusion of this pilot study, Headspace has launched a newer version of their original platform. While adhering to the fundamental introductory series of 10-min meditation sessions for the first 10 days, users can now elect to explore targeted goals such as relationships, creativity, focus, stress, and anxiety. There is now also an expanded ability to set reminders and alerts which may increase engagement with this type of application among medical students. There are also features to connect with friends and other users on Headspace and view each other's progress, which may create group accountability despite the individualized platform.
This pilot study did not perform secondary analyses on whether personal characteristics or demographics affected usage of the app. Future directions in this area of study may wish to examine if there are differences between participants who actually use the mobile app and those who never did. Further studies can also look at differences in characteristics between those individuals who chose to continue to use the mobile app beyond the first 30-day intervention period and those who did not. In their pilot study, the authors collected demographics data to determine any baseline differences between control and intervention groups, but the authors did not collect data to analyze differences between participants who used the app and those who did not.
Since the conclusion of the study in November 2013, a number of stress intervention programs have been implemented at the Keck School of Medicine. The Student Health Center now offers MBSR training workshops at least quarterly. The Integrative Medicine student interest group also offers weekly mind–body group sessions aimed at introducing different tools for stress reduction to the student population. As more information about burnout and life satisfaction for healthcare workers and medical students becomes available, the importance of stress reduction and burnout prevention becomes increasingly clear. It is imperative that medical schools invest time and resources into stress reduction training and other forms of self-care for students and faculty alike.
The current study is the first mobile mindfulness meditation intervention for medical students. The study supports the significance of the integration of mindfulness meditation practices in the educational curriculum; specifically stress reduction techniques, as these reductions will have a profound impact on the individual healthcare professional, as well as the manner in which s/he delivers clinical services to patients. Healing the healer can never be underestimated when it comes to the delivery of health and human services.
Footnotes
Acknowledgments
The authors thank Headspace, a digital health platform providing guided meditation sessions and mindfulness training through a smartphone app or website.
Previous Presentations
Poster Presentation: Yang E, Schamber L, Meyer R, Gold JI. Can Guided Mindfulness Meditation Decrease Stress and Improve Well-being for Medical Students? Article presented at Jacquelyn Perry Research Day, USC Health Sciences Campus, April 17, 2014, Los Angeles, CA.
Oral Presentation: Mindfulness Meditation for Medical Students. Presented at 6th Annual Graduate Research
Symposium, April 10, 2014, Los Angeles, CA.
Oral Presentation: Baxter International Foundation KSOM Summer Research Fellowship Award findings presented to Baxter Foundation Advisory Board, March 31, 2014, Los Angeles, CA.
Poster Presentation: Mindfulness Meditation for Medical Students. Presented at American Medical Student Association Annual Meeting, March 7, 2014, New Orleans, LA.
Oral Presentation: Mindfulness Meditation for Medical Students. Presented at Innovations in Medical Education Conference, February 22, 2014, San Gabriel, CA.
Author Disclosure Statement
No competing financial interests exist.