
Abstract
Objectives:
To examine the effects of music intervention on sleep quality in community-dwelling elderly people.
Design:
Two-armed randomized controlled trial.
Settings:
Four urban communities in Xi`an, China.
Participants:
People aged 60 years or older with poor sleep quality (Pittsburgh Sleep Quality Index [PSQI] score >7).
Interventions:
All participants received one sleep hygiene education session and biweekly telephone calls. Each participant in the intervention group received an MP3 player with a music database. The participants selected the preferred music and listened for 30–45 minutes per night for 3 months.
Outcome measures:
Sleep quality, the main study outcome, was measured by PSQI at baseline, 1 month, 2 months, and 3 months.
Results:
Sixty-four elderly people with a mean age of 69.38 ± 5.46 years were randomly assigned to the control group (n = 32) or the intervention group (n = 32). All participants completed the study, and none reported discomfort related to the music intervention. The intervention group demonstrated continuous improvements in sleep quality, with a global PSQI score of 13.53 at baseline, 9.28 at 1 month, 8.28 at 2 months, and 7.28 at 3 months. Although the global PSQI score in the control group also decreased from 12.26 at baseline to 8.72 at 3 months, the intervention group achieved greater improvements at each measurement (all p < 0.05). Repeated-measures analysis of variance revealed significant group-by-time interaction effects in global PSQI score and three component scores: sleep latency, sleep efficiency, and daytime dysfunction (all p < 0.05).
Conclusion:
Music is a safe and effective nonpharmacological intervention for improving the sleep quality of community-dwelling elderly people, especially in improving sleep latency, sleep efficiency, and daytime dysfunction.
Introduction
G
Pharmacologic treatment has been the main treatment for sleep disorders. 14 However, it also has adverse consequences, especially among elderly people, such as medication tolerance, daytime confusion, and increased risks for falls and fracture. 11,15,16 Given the rapid progress of aging, exploring safe and effective alternatives to improve sleep quality in elderly people has become a worldwide concern. Over the past decades, various nonpharmacologic interventions were studied for promoting sleep quality, such as cognitive-behavioral therapy, relaxation therapy, music intervention, and exercise. 17 –19
As a method that promotes mind–body interaction, sedative music is widely accepted for improving sleep by general population and healthcare professionals. 20,21 Its effects on sleep quality could be explained by the psychophysiological theory. 22 Physically, sedative music could slow down the body pace and adjust the autonomic nerves (e.g., suppressing the sympathetic system and activating the parasympathetic system). 22 Music is also related to increased release of oxytocin 23 and decreased levels of cytokine and catecholamine in plasma. 24,25 All of these changes contribute to a relaxing mood and help to initiate and maintain sleep. Moreover, music could improve the duration of rapid eye movement (REM) sleep and deep sleep, contributing to better perception of rest. 26 Psychologically, listening to sedative music could “take other things out of heads” and facilitate sleep onset. 27
Considering its safety and low cost, many studies explored the effects of music on sleep disorders in various populations. 28 –31 Some studies demonstrated prolonged deep sleep and increased sleep-wake cycles after receiving music provided by music therapists in neonates and infants. 32–33 Another study also added knowledge that music therapy was an effective and risk-free approach to induce sleep/sedation in children. 34 These studies indicated the validation of sedation practice undertaken by music therapists and its promising effects in improving sleep. 32 –34 Previous studies usually provided music intervention in a passive way, that is, listening to music through a tape recorder, CD/DVD player, or MP3/MP4 player. 28,29 Most of these studies used the Pittsburgh Sleep Quality Index (PSQI) to assess sleep quality, and significant improvements in PSQI scores were widely reported after music interventions. 35 –39 The dosage of music intervention varied among studies, with each session lasting 20–52 minutes, 38,40 at a frequency of daily to weekly, 38,41 and for total period of 1 day to 6 weeks. 38,39,42,43 In addition to professional music therapies, music intervention could also be carried out by doctors, nurses, caregivers, and volunteers. 25,28,44
Music intervention has been implemented in various settings. Most of these studies were conducted in hospitals among patients undergoing invasive treatments (e.g., coronary artery bypass graft surgery or anorectal operation). 37 –39,42 Only a few studies were conducted in communities, in which the participants listened to music by themselves at home. 41,43,45
Recent systematic reviews also indicated that sedative music may be effective in improving sleep quality in adults. 28,29 Because the longest period of music intervention was 6 weeks, 43 the effect of music on sleep quality after 6 weeks was still unknown. Moreover, limited studies were randomized controlled trials, and even fewer studies were conducted in China. 28,29 The effect of music on sleep quality among Chinese elderly people was therefore uncertain. China has the largest elderly population in the world, and most of them live in communities. 46 Considering the poor sleep quality in Chinese elderly people, 5,6 it is necessary to explore a safe, effective and cost-contained measure to improve their sleep quality. Given the promising effects of music in promoting sleep quality, the present study aimed to examine the effects of music intervention on sleep quality among Chinese community-dwelling elderly over a 3-month period.
Materials and Methods
Study settings and participants
This two-armed randomized controlled trial was conducted in Xi'an, the capital of Shaanxi Province, China. Elderly residents with poor sleep quality were recruited from four urban community centers. Each community center serves about 6500 residents, including 550 elderly people. 47
The inclusion criteria were (1) age 60 years or older, (2) poor sleep quality (global PSQI score >7 48 ), and (3) ability to communicate in Chinese. Participants with cognitive disabilities, impaired bilateral hearing abilities, or a history of alcohol/drug abuse were excluded. Those who were musicians or had previously received music interventions were also excluded.
The sample size was estimated on the basis of power analysis. A sample of 46 participants will provide the study 80% power at a two-tailed α of 0.05 to achieve an effect size of 0.35 on sleep quality. 49 Considering a 20% attrition rate in the 3-month follow-up, at least 58 participants were required, with 29 in each group.
Music database
A database with 169 pieces of music was developed by the researcher and an expert team. Because of the limited availability of registered music therapists in China, the present study alternatively invited a musician, who was the music professor in a local conservatory of music and was experienced in music intervention, 50,51 to develop the music database and to guide the delivery of the interventions. Moreover, a psychiatric physician with expertise in sleep disorders and a gerontologist were also included in the expert team. As suggested by previous research, all selected music was soft and sedative, with stable melodies at a tempo of 60–80 beats per minute. 25,52 Previous studies suggested that familiar and preferred music would improve participants' acceptance and adherence. 52 The current music database includes various types of music, including Chinese instrumental classic, Western classic, natural sounds music, and classical songs without lyric. The participants could find their preferred music from this database.
Interventions
Sleep hygiene education
All participants in the present study had poor sleep quality (global PSQI score >7). Following the principle of beneficence, one session of sleep hygiene education was provided to all participants. A standardized education protocol was developed based on literature reviews. 18,53 The education included four aspects, including basic knowledge of sleep; preparing a comfortable environment for sleep; avoiding smoking, alcohol, tea, coffee, cola, being too full or too hungry before sleep; and keeping regular sleep schedules. The education was provided face-to-face to individual participants by the researcher and took 10–15 minutes.
Music intervention
In addition to sleep hygiene education, the intervention group received a 3-month music intervention, which entailed listening to music for 30–45 minutes per night. Each elderly person in the intervention group received an MP3 player, in which the music database was stored. The researcher demonstrated how to operate the player, including turning it on and off, selecting music, pausing and resuming playing, adjusting the volume, and charging. Return demonstrations were performed to ensure that each participant could independently operate the player. Moreover, structured instructions about the music intervention were also provided: (1) finding a quiet environment; (2) assuming the most comfortable position with eyes closed; (3) being relaxed when listening to the music; (4) choosing the preferred music; (5) playing the music at a comfortable volume (60 dB) or the lowest audible volume; 54 and (6) listening to the music with earphones for 30–45 minutes every night before sleep. 52
Telephone follow-up
Biweekly telephone calls were made to all participants. The calls reviewed key points of the sleep hygiene education. For the intervention group, the participants were also reminded to listen to the music as instructed.
Measures
Demographic data
The demographic data were collected by a structured questionnaire, including age, sex, educational level, marital status, and religious beliefs.
Sleep quality: PSQI
Sleep quality was measured by the 19-item self-report PSQI, Chinese version (PSQI-C). The instrument measures seven components of sleep quality: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction. 55 Each component score ranges from 0 to 3. The global PSQI score is a sum of all component scores, ranging from 0 to 21. A higher score indicates poorer sleep quality. The PSQI has been widely applied in different populations, including elderly people. 56 The PSQI-C had been validated among 793 adults with a Cronbach α of 0.84 and test-retest reliability of 0.83. 48 A cutoff score of >7 yielded a sensitivity of 98.3% and specificity of 90.3% in identifying poor sleep quality among Chinese adults; 48 this score was also used in the present study.
Data collection
Figure 1 demonstrates the study flow. All participants were recruited by poster advertisements in community centers from October 2011 to January 2012. Elderly people who responded to the advertisements underwent screenings with PSQI-C and eligible persons were invited to participate. After each participant provided written consent, baseline data were collected. Thereafter, the participants were assigned to the invention or control group by opening a sealed opaque envelope with a computer-generated randomization number indicating the group allocation. All participants received sleep hygiene education and biweekly telephone calls. In addition, each participant in the intervention group received an MP3 player with the music database. Detailed instructions for the 3-month music intervention were provided. As introduced in previous session, the elderly people in the intervention group listened to the music for 30–45 minutes every night before sleep. The baseline data collection and all interventions were performed by the same researcher (the first author).
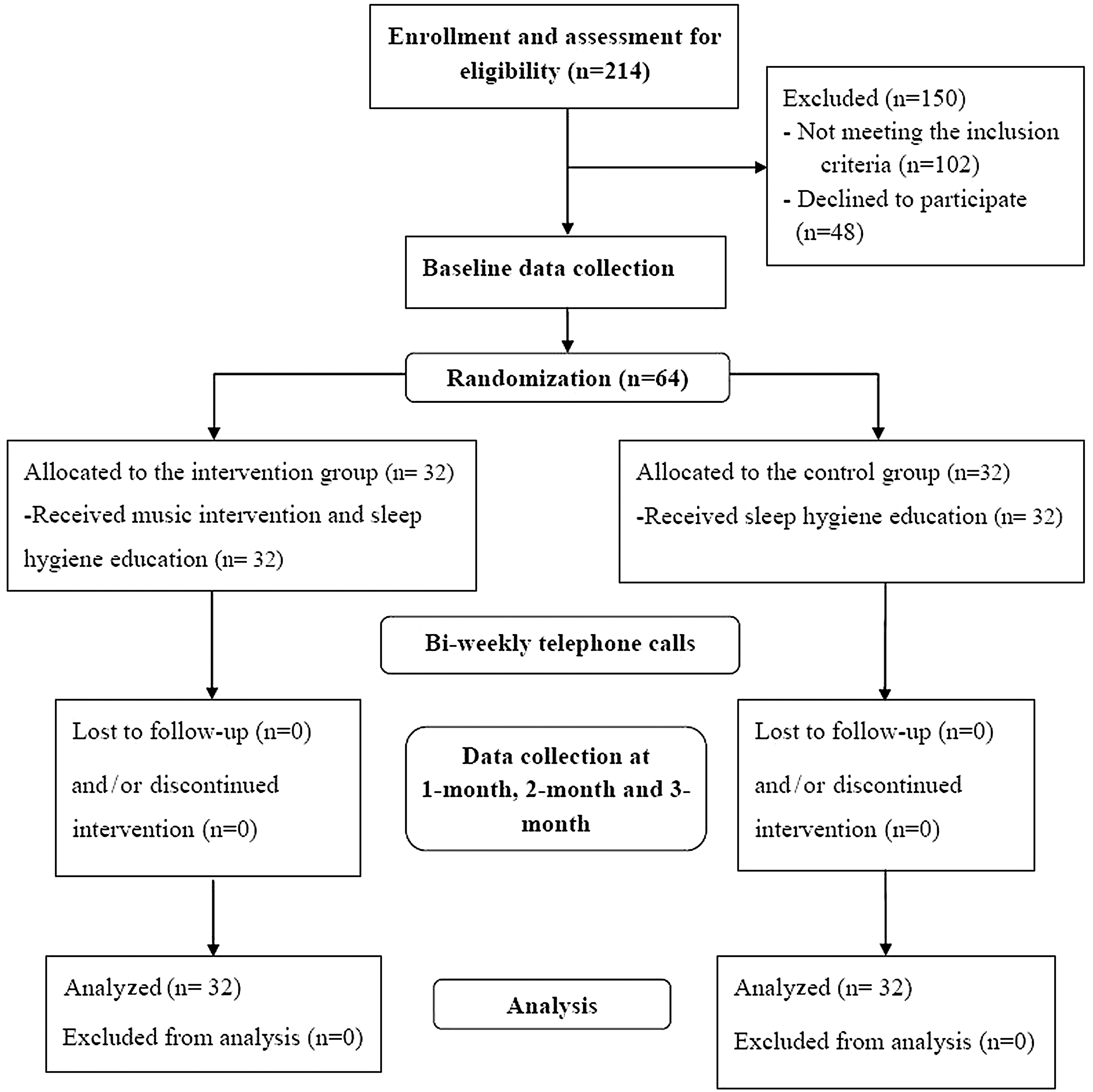
Study flowchart.
Previous studies recommended 3 weeks as the shortest period for observing changes in sleep quality. 57 Moreover, the PSQI assesses sleep quality over a 1-month interval. 55 Therefore, the follow-up measurement was conducted at 1 month (T1), 2 months (T2), and 3 months (T3) after the study entry. The follow-up measurements were conducted by a research assistant, who had received training for administering PSQI and was blinded with the group allocations.
Ethical considerations
This study was approved by the Human Research Ethics Committee of the University. All participants received detailed introduction about the study. They were told about the rights to withdraw at any time without detrimental effects. Written consent was obtained from all participants. Confidentiality and anonymity were assured during the study.
Data analysis
An intention-to-treat analysis was used in the data analysis. Descriptive statistics of frequency, percentage, or mean and standard deviation were applied to describe the data as appropriate. The normality of each variable was tested through skewness and kurtosis statistics. The independent t-test and chi-square test were used to test the homogeneity of the sample. Independent t-tests were applied to compare the changes in sleep quality between groups at each time point. Two-way repeated-measures analysis of variance (RM-ANOVA) was used to examine the effects of music intervention. Effect size was calculated as partial Eta square (η
Results
Among the 214 elderly people who received screenings, 102 did not meet the study criteria and 48 declined to participate. The study recruited 64 participants, with 32 in each group. No difference was detected in characteristics and sleep quality between the elderly people who participated and those who declined to participate (all p values >0.05). All participants completed the whole study, and none reported discomfort related to the music intervention. The participants had a mean age of 69.38 ± 5.46 years. Most were women (80.9%), were married (76.5%), and had secondary education or greater (71.9%). As presented in Table 1, the two groups revealed similar demographic characteristics (all p values >0.05).
Unless otherwise noted, values are the number (percentage) of participants. Values expressed with a plus/minus sign are the mean ± standard deviation.
Tested by independent t-tests.
Table 2 summarizes the sleep quality of the participants at different time points and results of RM-ANOVA. Except for use of sleep medication, six components of PSQI were scored at >1.0, indicating poor sleep quality in individual aspects. At baseline, the two groups revealed no significant difference in individual component scores or global scores in PSQI (all p values >0.05). After interventions, the intervention group demonstrated continuous improvements in sleep quality, with the global PSQI score of 9.28 at T1, 8.28 at T2, and 7.28 at T3. Meanwhile, the control group showed similar changes in PSQI scores. However, RM-ANOVA analysis revealed significant group-by-time effects in global PSQI score (F = 4.189; p = 0.009) and three components: sleep latency (F = 3.684; p = 0.017), sleep efficiency (F = 2.850; p = 0.045), and daytime dysfunction (F = 3.688; p = 0.0177).
Values are expressed as mean ± standard deviation or number (percentage) of participants.
Repeated-measures analysis of variance.
p < 0.05.
p < 0.01.
PSQI, Pittsburgh Sleep Quality Index; S-Q, subjective sleep quality; S-L, sleep latency; S-DU, sleep duration; S-E, sleep efficacy; S-DI, sleep disturbances; S-M, use of sleep medication; S-DD, sleep of daytime dysfunction.
The PSQI also provided detailed information on sleep duration, time spent in bed, sleep efficiency, and sleep latency (Table 2). As study going on, both groups demonstrated continuous improvements in sleep duration, time spent in bed, and sleep efficiency. However, only sleep efficiency revealed significant group-by-time effects in the RM-ANOVA analyses (p = 0.005). At baseline, 26 (81.25%) participants in the intervention group could not fall asleep within 30 minutes three or more times per week, and 15 (46.88) needed more than 60 minutes to fall asleep. After the 3-month music intervention, the number decreased to 7 (21.88%) and 4 (12.5%), respectively.
Table 3 presents the changes in sleep quality at different time points. Compared with the control group, the intervention group achieved greater improvements in global PSQI score at each time point (p = 0.020, 0.012, 0.001). Regarding individual component, the intervention group revealed greater improvements in sleep latency (p = 0.041) and daytime dysfunction (p = 0.005) at T1 and in sleep latency (p = 0.003), sleep duration (p = 0.023), and sleep efficiency (p = 0.006) at T3. Figure 2 presents the sleep quality of both groups.
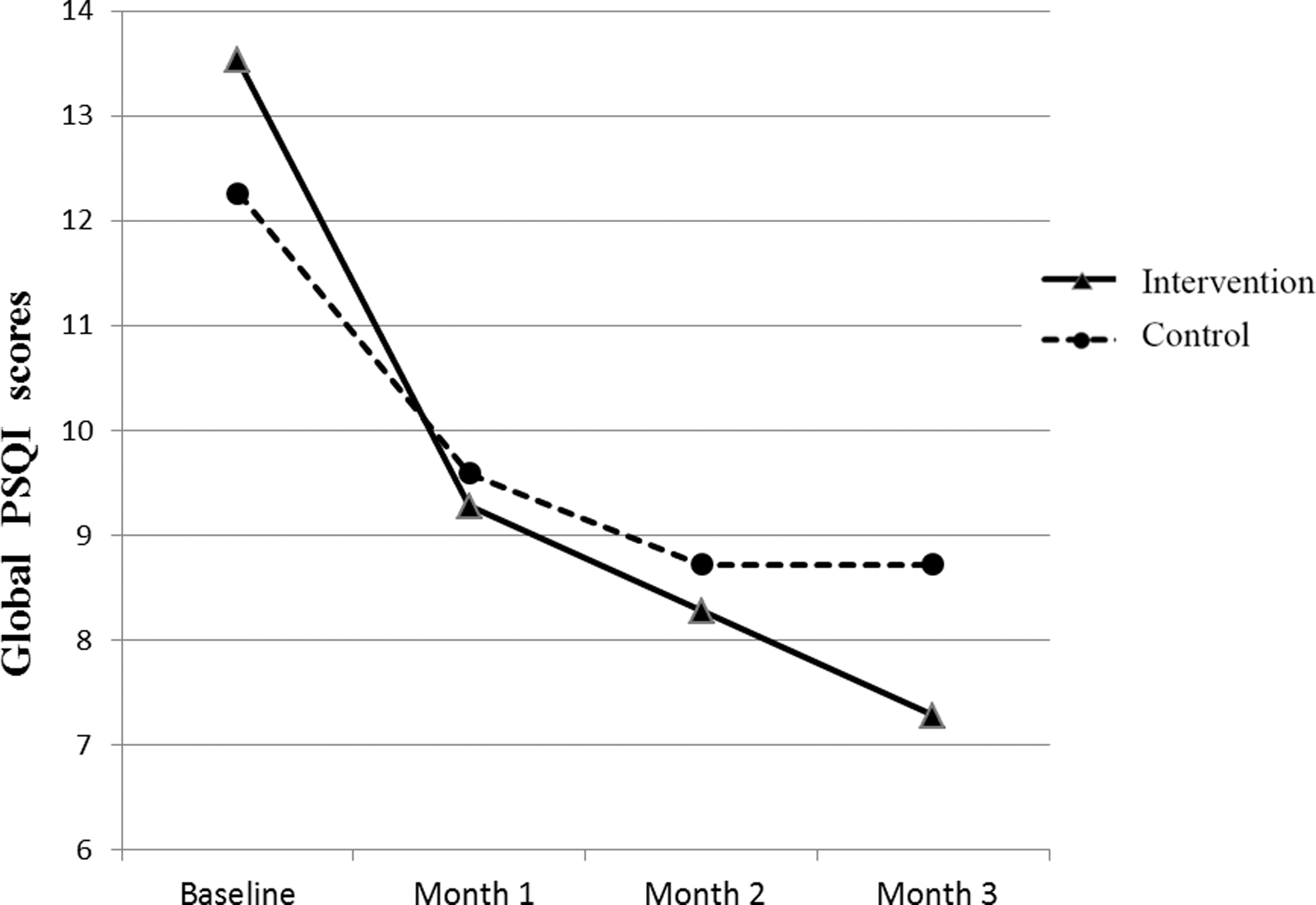
Global Pittsburgh Sleep Quality Index (PSQI) scores of the two groups at different time points.
1-mo changes: changes between baseline and first month; 2-mo changes: changes between baseline and second month; 3-mo changes: changes between baseline and third month.
Independent t-tests between groups.
p < 0.05.
p < 0.01.
Discussion
To the best of our knowledge, this was the first study that used music among Chinese community-dwelling elderly with poor sleep quality. It contributed new evidence to the effect of music intervention on sleep quality in 3 months. During the study, no discomfort or adverse effects related to the music intervention were reported. The intervention group demonstrated continuous improvements in sleep quality. By the end of the study, 16 (50%) elderly people in the intervention group achieved normal sleep quality, with a PSQI global score of 7 or less. Findings of the study indicated that music intervention was safe and effective in improving sleep quality in Chinese elderly people.
Compared with the control group, the intervention group achieved greater improvements in global PSQI score throughout the study. The beneficial and cumulative effects of music on sleep quality were consistent with previous findings. 29,41,43,45 In contrast to previous studies that provided no interventions to the control group, 41,43,45 participants in the control group in the present study also demonstrated improvements in sleep quality. These improvements may be ascribed to the sleep hygiene education. 18,53 However, the RM-ANOVA analysis reported significant group-by-time effects (p < 0.05), which indicated the superior effects of music intervention to a single education session (p < 0.05).
Previous studies focused on the global PSQI score. 28,29 Only a few studies reported the effects of music on individual aspects of sleep quality. 30,45 In the present study, the music intervention revealed significant effects in improving three components of sleep quality: sleep latency, sleep efficiency, and daytime dysfunction. The findings in individual components would provide insights to help improve understanding of the mechanisms of music intervention.
Sleep latency is the length of time from full wakefulness to sleep. 38 At baseline, only 8 (25.0%) participants in the intervention group could fall asleep within 30 minutes. As the intervention proceeded, 20 (62.5%) participants at T1, 21 (65.6%) at T2, and 25 (78.1%) at T3 could fall asleep within 30 minutes. This finding was consistent with that in a previous music interventional study. 45 The psychophysiologic interactions between the body and music could facilitate the onset of sleep and lead to the significant improvements in sleep latency. 22,27 On the one hand, soft and sedative music could lead to an adjustment in the autonomic nerve system and induce relaxation responses, which physically prepare the body for sleep. 22 On the other hand, listening to music could distract the listener from disturbing thoughts and psychologically help initiate sleep. 27 Therefore, music could effectively reduce sleep latency among elderly people.
Sleep efficiency is the proportion of actual sleep time during time spent in bed. 38 Sleep efficiency is a comprehensive indicator associated with both sleep duration and sleep latency. The significant improvements in sleep efficiency in the intervention group may first be ascribed to the prolonged sleep duration. In addition, the shortened sleep latency discussed in previous sessions also indicated that the time spent in bed was more efficiently used for actual sleep.
Consistent with the present finding, one study also reported significant improvements in sleep efficiency score on the PSQI after music intervention. 45 In another study, Chang et al. did not observe significant improvement in sleep efficiency on polysomnography (PSG). 26 Compared with the present study, Chang's study recruited younger adults (age 22–58 years) with better sleep quality (baseline global PSQI score, 9.66) and included more women (94.0%). Moreover, their music intervention lasted only 4 days. The unique characteristics of their participants and short-term intervention may lead to nonsignificant effects on sleep efficiency. Because the PSQI is a subjective measurement of sleep quality based on self-report information, the accurate effects of music on sleep efficiency should be further examined with objective measurements, such as PSG. The current findings indicated that the 3-month music intervention was effective in improving sleep efficiency among elderly people.
Daytime dysfunction reflects the subjective perception of daytime activities after sleep. 38 One study indicated similar findings that may indicate the mechanisms of music in reducing daytime dysfunction. 26 In Chang and colleagues' study, participants who received music intervention rated higher scores on perceptions of rest after sleep, which may facilitate daytime function. Moreover, PSG indicated longer REM sleep after listening to music. Because REM sleep is critical for psychological and emotional health, prolonged REM sleep would also contribute to better perceptions of daytime function. 26 However, another study did not reveal significant improvements in sleep disturbance after music interventions. 45 Compared with the present study, their nonsignificant results may be related to the short-term (3-week) music intervention.
The present study provided various types of music and allowed the participants to choose their preferred music. Consistent with previous findings, 41,43,45 although the participants listened to different types of music, they consistently demonstrated improvements in sleep quality. This finding supported the idea that the beneficial effects of music on sleep were not derived from a specific type of music but from the sedative characteristics, such as stable melodies and slow pace at a tempo of 60–80 beats per minute. 41,43,45
All participants completed the whole study, indicating the acceptability of music intervention among elderly people. The good adherence in the present study may stem from two aspects. First, the biweekly telephone calls facilitated to build trust relationships with the elderly people, which would ensure their participation. Moreover, the continuous improvements in sleep quality would also attract the participants to stay in the study.
This study also had some limitations. First, listening to music was self-conducted by the elderly people at home. Although biweekly telephone calls reminded them to listen to the music as instructed, the actual dose of music intervention may vary among individuals. Second, sleep quality was measured by the PSQI, which could not provide more accurate and objective information of sleep quality (e.g., deep sleep and REM sleep duration). Thus, future studies should use objective measurements, such as PSG and actigraphy. Third, the present study lasted 3 months. This appears to be the longest reported music intervention for sleep quality. Whether the effects could maintain over the longer term is uncertain. Future studies could use a longer follow-up period, such as 6 months or 1 year. Telephone calls are suggested to provide ongoing support and reminders, which would improve participants' adherence. Moreover, all participants were community-dwelling elderly people with poor sleep quality. These characteristics should be considered in applying the current findings to other populations.
Live music and music therapy implemented by music therapists provide more entertainment and opportunities of selecting music by patients themselves and thereby may be more efficacious for sleep inductions. 29,34 Future studies could use live music or music therapy in improving sleep quality in various populations.
Conclusions
Music intervention is a safe and effective nonpharmacologic approach for improving the sleep quality among Chinese community-dwelling elderly people, especially in improving sleep latency, sleep efficiency, and daytime dysfunction. Given its safety, simple implementation, and low cost, music intervention could be used to improve sleep quality not only in communities but also in clinical settings.
Footnotes
Acknowledgments
The authors thank Professor Weijun Yang (the music professor), Dr. Wei Fu (the psychiatric physician), and Professor Zhonghua Wang (the gerontologist) for assistance in establishing the music database and guiding the delivery of the music intervention.
Author Disclosure Statement
No competing financial interests exist.