
Abstract
Objectives:
The aim of this study was to compare chronic pelvic pain, menstrual patterns, and quality of life (QoL) in two groups of women with endometriosis: those who did and those who did not participate in a specific 8-week yoga intervention.
Method:
This was a randomized controlled trial. It was conducted at the University of Campinas Medical School, Campinas, SP, Brazil. Forty women were randomly divided into two groups: an intervention group of women who practiced yoga (n = 28), and a control group of women who did not practice yoga (n = 12). Participants attended 90-min scheduled yoga sessions twice a week for 8 weeks. Additionally, an Endometriosis Health Profile (EHP)-30 questionnaire was applied to evaluate women's QoL at admission and 2 months later upon completion of the yoga program. Menstrual and daily pain patterns were evaluated through a daily calendar (visual analog scale).
Results:
The degree of daily pain was significantly lower among the women who practiced yoga compared with the non-yoga group (p = 0.0007). There was an improvement of QoL in both groups between baseline and the end of the study evaluation. In relation to EHP-30 domains, pain (p = 0.0046), impotence (p = 0.0006), well-being (p = 0.0009), and image (p = 0.0087) from the central questionnaire, and work (p = 0.0027) and treatment (p = 0.0245) from the modular questionnaire were significantly different between the study groups over time. There was no significant difference between the two groups regarding the diary of menstrual patterns (p = 0.96).
Conclusions:
Yoga practice was associated with a reduction in levels of chronic pelvic pain and an improvement in QoL in women with endometriosis.
Introduction
E
Many treatments used for symptomatic endometriosis include clinical and surgical options such as non-steroidal anti-inflammatory drugs (NSAID), gonadotrophin-releasing analogues (GnRH-a), androgen derivatives, combined oral contraceptives, and progestogens. 6 Nevertheless, their side effects contribute to discontinuation of treatment and recurrence of symptoms. 7 The efficacy of surgical options remains uncertain (85% of women undergoing a surgical procedure may return with further complaints of CPP) and involves risks. 6 –8
Despite the large body of publications about endometriosis, there is so far no single therapy that eradicates the disease and its symptoms. 6 The literature shows that CPP and dyspareunia are the most prevalent symptoms, followed by mood swings, depression, and anxiety, which are present in >60% of cases and which affect patients' quality of life (QoL). 9 Therefore, improving women's QoL is perhaps one of the main objectives in the management of this disease. 10
The multiple drawbacks in the treatment of endometriosis have increased the importance given to alternative and complementary methods to control the disease and reduce its recurrence. Mind–body practices could benefit the immune system, control stress and pain, and improve mental health, leading to an improvement in QoL. 2,10 –15 However, there are few scientific reports about these methods, although it has been suggested that its use is widespread and the actual success remains unknown. 8,14 One study 15 integrated two conventional treatments (NSAID and hormonal therapies) with complementary therapies (yoga practice and t'ai chi) and concluded that dysmenorrhea, pelvic congestion, and lower back pain can be reduced.
Currently, yoga is classified as a mind–body practice, considered an integrative and complementary health practice by the World Health Organization. 16,17 Yoga combines physical exercises, meditation, and respiratory techniques that strengthen the muscles and relieve stress. 18 It also helps the body and mind to adapt to depression and anxiety and has a calming and relaxing effect on the individual. Studies have associated the practice of yoga with the relief of many chronic conditions 18 –22 such as lower back pain, 18 asthma, 19 migraine, 20 diabetes, 20 high blood pressure, 21 hypercholesterolemia, 21 signs of menopause, 22 and multiple sclerosis. 23
Major electronic databases were searched for articles in English published between 2000 and 2015. The databases included PubMed, PsychInfo, MEDLINE, and Google Scholar. Key search words included yoga, endometriosis, and complementary and alternative medicine (CAM). All styles of yoga were included. Nevertheless, no reports on the regular practice of yoga among women with CPP-associated to endometriosis were found, and few studies correlated yoga and CPP, menstrual flow, and QoL in women with endometriosis. There were no controlled trials or consensus on the activity's frequency or on which asanas (psychophysical exercises) and pranayamas (breathing exercises) to use. Consequently, the objectives of this study were to evaluate the effect of an 8-week program of yoga practice upon CPP, menstrual flow, and QoL among women with endometriosis.
Material and Methods
This prospective study was carried out from August 2013 to December 2014 in the endometriosis outpatient clinic and in the outpatient physical therapy clinic of the Department of Obstetrics and Gynecology, University of Campinas (UNICAMP) Medical School. The study was approved by the Ethical Committee, and all women signed an inform consent form before beginning the study.
Women were included if they were 18–50 years old, presented with a confirmed diagnosis of endometriosis, had CPP with a score >4 measured by visual analog scale (VAS), 24 had already received some type of treatment for endometriosis (e.g., hormonal therapy, laparoscopy, etc.), and were available to attend the clinic to practice yoga twice a week for 8 weeks. The exclusion criteria were being pregnant, having recent physical trauma, and exercising more than three times a week.
Study design
The study was a randomized controlled trial. The randomization sequence for the yoga group or the non-yoga group was computer-generated in a proportion of 3:1. Upon admission, an envelope with the subject number was opened, and a slip informed the group allocation. For every three women assigned to the yoga group, one woman was assigned to the control group. The women in the non-yoga group received standard treatment given to every endometriosis patient at the clinic: medication and/or one individual physical therapy session a week. To calculate the sample size, a pain intensity parameter previously published by Rakhshaee was used. 25 A total of 40 women with endometriosis and associated CPP took part and were divided into two groups: a yoga intervention group (n = 28), and a group of women with endometriosis and CPP who did not practice yoga (n = 12). Randomization followed with a type I error (alpha) of 0.05 and beta of 0.20.
Assessments
In a first assessment, eligible participants had a baseline interview and a physical evaluation with the physical therapist (principal investigator), and they were informed about the study's procedures. They answered general questions regarding sociodemographic characteristics, their history of endometriosis, and medication currently being used, as well as specific questions related to pain and to exercise patterns. The women who agreed to participate were randomly assigned to either the yoga program twice a week for 2 months or the control group. Women in the control group did not have any yoga practice at all.
To evaluate the data referring to the women's QoL upon admission and upon completion of the yoga program, the Endometriosis Health Profile (EHP-30) questionnaire was applied. This consists of two parts. The first part is a core questionnaire containing five domains (pain, control and powerlessness, emotional well-being, social support, and self-image) comprising 30 items that are applicable to all women with endometriosis. Items 5 and 6 in the pain domain are about limitations in practicing physical activities due to pain. This second part is a modular part containing six domains (work, relationship with own children, sexual intercourse, doctor relationship, treatment, and infertility) comprising 23 items that do not necessarily apply to all women with endometriosis. However, explored in depth, it contains some issues that might be relevant. Each domain ranged from 0 (never) to 5 (always) so that the minimum points achieved would be zero (indicating the best health status) to 100 (indicating the worst health status) to measure the extent of ill health. 5 Menstrual patterns measured daily for 8 weeks were also evaluated using a 0–5 scale for the quantity of blood. Participants registered their daily pain through a VAS on which they marked a score ranging from 0 (no pain at all) to 10 (the worst pain imaginable). 24 The women were instructed to fill in the daily pain and menstrual pattern at the same time every day, and this was collected at the end of the study. Twice a week, before and after the yoga session, women in the yoga group filled in the VAS, which was collected at the end of each practice.
Intervention
The yoga program consisted of 2 h sessions held at the clinic twice a week and conducted under the guidance of the same qualified yoga instructor. Participants joined the practice at any time and left after 8 weeks. Sessions consisted of 30 min conversation and interaction among the participants; 10 min of initial physical and psychological relaxation, with pranayamas (Prāṇa Kriyā Prāṇāyāma), intonation of mantras (Om and Shanti Mantras), and body awareness; 60 min of asanas (hatha yoga postures with 5–10 breathing exercises); 10 min of exercises for physical and psychological relaxation that included meditation, breathing techniques, and chanted mantras; and a final 10 min where the women commented on the session and organized the room in which the class took place.
The same asanas were used during each session, with some variations depending on the pain intensity of the participants. The asanas used were Parighasana, Parighrasana with a twist, BaddhaKonasana, Upavistha Konasana in Dandasana, Badha Konasana, Dandasana, Purvottanasana (variation with legs crossed), BaddhaKonasana in Dandasana, Setu Bandha sarvangasana, Pavanmuktasana, Jatara Parivartanasana, Bhujangasanana, Marjaryásana, AdhoMukhaSvanasana, Balasana, Dandasana variation, BaddhaKonasana on the wall, ViparitaKarani, Matyasana, and Savasana.
Data analysis
First, a descriptive analysis of the measurements was performed for the quantitative variables, and absolute frequencies and percentages was performed for categorical variables of the total sample. The differences in the quantitative variables were assessed by t-test if the distribution of variables was normal or by Mann–Whitney test otherwise. To assess the association between categorical variables, the chi-square test or Fisher's exact test was used. The analysis of variance was used for the analysis of the areas of EHP-30 questionnaire for repeated measures. In the evaluation of the daily pain and menstrual patterns, the differences between the groups were evaluated using the Kolmogorov test. Differences were considered significant if p < 0.05.
Results
Figure 1 shows a flow chart for both groups in the study. Twenty-eight women started the yoga program. However, only 16 women completed the 2 months of the program; the other 12 women discontinued the yoga practice after attending a few sessions. The main reasons were not having childcare available and starting to work full time. One of them stopped for medical reasons. They were considered part of the yoga group in the data analysis as an intention-to-treat cohort. Twelve women were assigned to the control group. The women who practiced yoga were comparable to the women who did not practice Yoga in terms of age, marital status, use of medication, religious orientation, body mass index (BMI; kg/m2), length of endometriosis diagnosis, and pain-VAS score at baseline (Table 1). However, years of schooling and professional activities were different between the groups.

Flowchart.
Data were analyzed using Student's t-test* or the Mann–Whitney test** with p < 0.05 as significant.
BMI, body mass index; VAS, visual analog score.
Regarding the QoL EHP-30 questionnaire, in both groups, the scores decreased from the beginning of the yoga program through the duration of the observation (Table 2). There was a significant difference between the two groups over time in relation to the EHP-30 central questionnaire's domains (pain, control and powerlessness, emotional well-being, and self-image) but not in social support. As for the EHP-30 modular questionnaire's domains, work and treatment were significantly different when comparing the two groups over time (Table 3). In other domains (relationship with own children and sexual intercourse), both groups had lower scores over time. However, these differences were not significant. With regard to infertility and doctor relationship, both groups increased their scores over time.
EHP, Endometriosis Health Profile.
p-value < 0.05 is significant.
SD, standard deviation.
During the 8 weeks of the program, there was no significant difference between the two groups regarding means scores on the diary of menstrual patterns (Fig. 2). Regarding the pain-VAS score, when comparing the two study groups, there was a significant difference in daily pain behavior in women who practiced yoga. The average pain scores were lower compared with women in the group who did not practice yoga, whose pain had a tendency to increase (Fig. 3).

Average scores of menstrual flow between the groups during the 8-week yoga program.
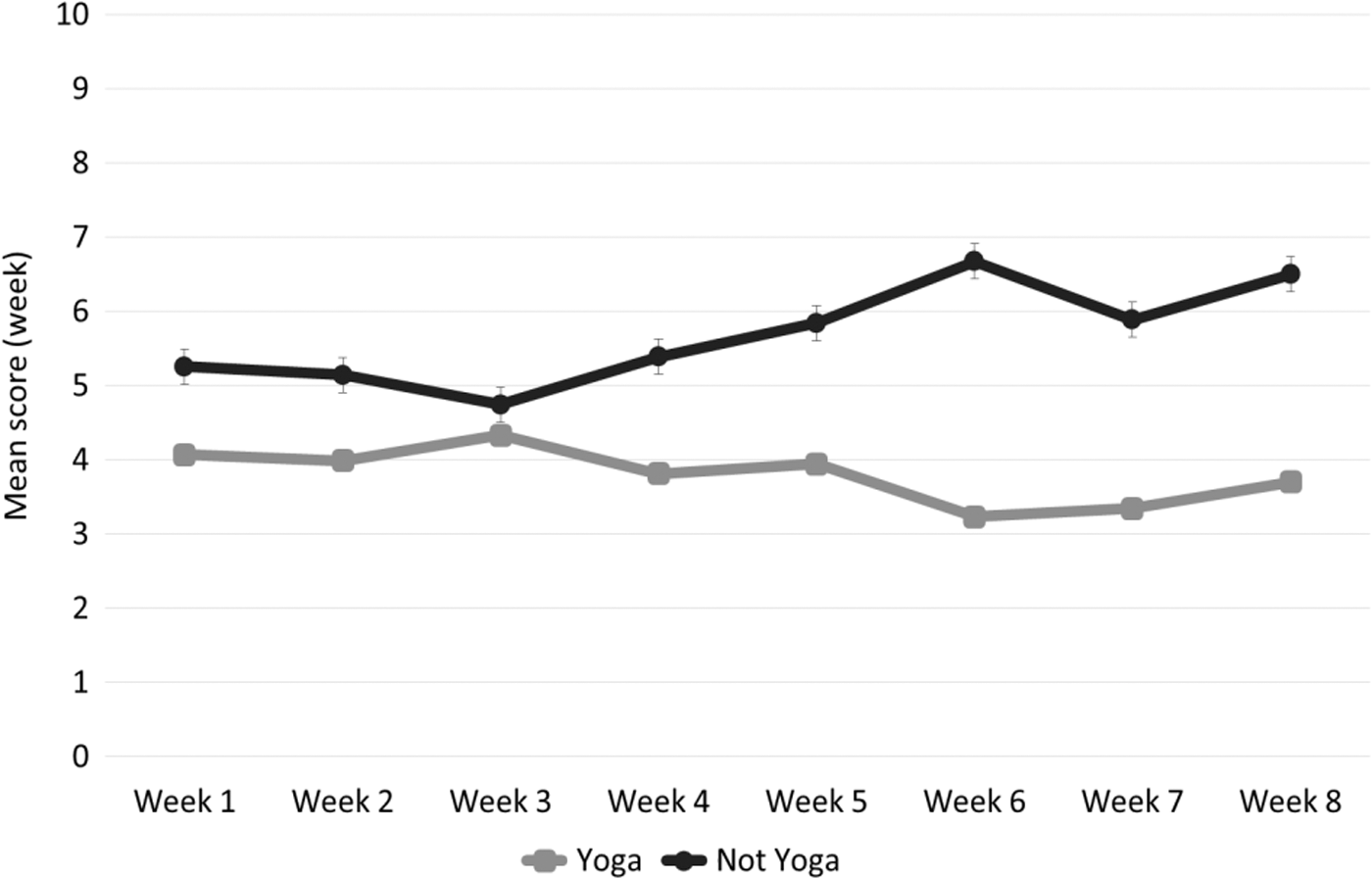
Average scores of pain between the groups during the 8-week yoga program.
Discussion
A positive association was observed between yoga practice and pain relief and QoL in women with endometriosis. The QoL assessed by the EHP-30 and the evaluation of pain-VAS score within the 8 weeks of treatment was significantly lower among the women who practiced yoga compared with those who did not participate in the yoga intervention. Furthermore, the women in the yoga group improved their QoL in the domains of pain, control and powerlessness, emotional well-being, self-image, and social support. In the modular questionnaire, the domains that were significantly lower in the yoga group were work, relationship with own children, treatment, and sexual intercourse. Both groups showed a reduction in daily pain rates. However, women who participated in the yoga group showed a significant reduction, probably because they presented with lower stress levels and greater relaxation.
Several studies have linked the effects of yoga practice with various aspects of both physiological and psychological health, and in response to stress. 20,25 –30 Chronic stress was associated with poor activation of the hypothalamus–pituitary–adrenal axis and autonomic nervous system. This system is responsible for the stress response through the sympathetic and parasympathetic nervous system, and it affects respiratory, cardiac, and digestive functions. The hypothalamic–pituitary–adrenal axis also regulates metabolism, the immune system, thyroid function, and reproduction. 23,25,26,28,30 Relaxation used in yoga practice can counteract the negative effects of stress by restoring balance to the autonomic nervous system and the hypothalamic–pituitary–adrenal axis. 26 Thus, yoga, meditation, and relaxation can be adjuvant therapy in clinical practice, and may have benefit beyond clinical treatment alone. 20,25 –30 It is likely that the balance in the autonomic nervous system acquired by the practice of breathing techniques, yoga postures, and meditation contributed to the improvement in pain levels reported by the women in this study.
Many studies have reported positive relationship between yoga practice and improvement in gynecological problems such as menstrual irregularities, dysmenorrhea, and hormonal disorders. 25 –27 However, there appear to be no reports of women with endometriosis. The practice of yoga allows the union of body and mind through meditation, relaxation, breathing exercises, and different postures. These techniques, which promote well-being and stress reduction, involve physical activity, but this differs from purely fitness exercise because practitioners focus their minds on their bodies, with inner awareness and a meditative focus. 20,26,28
A self-specific questionnaire of QoL was used in this study. The domains of the central questionnaire that improved with yoga practice were pain, control and powerlessness, emotional well-being, and self-image. The domain in the modular questionnaire that improved with yoga was work.
In recent studies on yoga practice in women with dysmenorrhea, it was suggested that some yoga poses can reduce pain during menstruation. 25,30 The cobra pose improves spinal flexibility and strengthens the muscles in the back. The cat pose initiates movement from the center and coordinates movement and breath. The fish pose relieves stiffness of the neck and shoulder muscles and improves the flexibility of the spine. 25 These postures were part of this project. This suggests that yoga could be a good technique to reduce not only menstrual pain but also the pain associated with endometriosis. According to these studies, 25,30 the practice of yoga can regulate the pain gate control mechanism located in the spinal cord and the secretion of the body's natural opioids. Thus, breathing exercises can help to reduce pain due to increased exhalation, which produces relaxation and decreased tension. 28 Breath awareness contributes to calmer and slower breathing, promoting relaxation, and helping to control pain. 20,23,25,28 –30 Corroborating the present findings, yoga practitioners and patients using CAM both reported a sense of personal responsibility for their health and outcomes, seeking a non-medical approach and a way to maximize their individual treatment. 31
Regarding QoL, it was observed that improving one domain might have affected improvement in other domains in the EHP-30. For example, having more control and feeling less powerless might have improved self-image and emotional well-being. One qualitative study reported that yoga practice in patients with neck pain enabled self-control over their bodies and their health, freeing them from feeling as controlled by their pain as they had done before. 30 Additionally, no improvement in QoL scores was observed in either groups in two domains: doctor relationship and infertility. The women who practiced yoga may not have associated the practice with any treatment. They might have seen the yoga practice as something not related to medical treatment, since it was conducted on different premises, and the yoga instructor (a physical therapist) is not part of the staff at the endometriosis clinic.
This study has some limitations and strengths. One limitation is that the women in the yoga group had attended significantly more years of schooling than the group that did not practice yoga. It is possible that these women had more opportunities to learn about yoga and its benefits, and it might have contributed to their adherence to the yoga practice. Additionally, it is possible that the women in the yoga group were available to participate in the weekly sessions because only 13% of them were employed outside the home, while 50% of the women that did not practice yoga were employed. Another limitation was the small number of cases that may have been influenced because the practice of yoga took place twice a week, and many women were unable to attend because they worked and or had no childcare available. In addition, the results only indicate experiences during and immediately after the yoga program. A strength of this study is that prior to yoga sessions, women had time to talk among themselves and with the yoga instructor who, when possible, was able to clarify some of the questions the participants had regarding treatment, diagnostic procedures, or other issues. Apparently, it contrasted with the kind of attention they received in the doctor's office.
Conclusions
This study showed that yoga practice was associated with a reduction in levels of CPP and an improvement in QoL in women with endometriosis.
Footnotes
Acknowledgments
Financial support was received from the Brazilian National Research Council (CNPq), grant #573747/2008-3. A.V.G. was a fellow from CAPES, Ministry of Education, Brazil.
Author Disclosure Statement
No competing financial interests exist.