
Abstract
Objective:
To examine the effects of a comprehensive residential mind–body program on well-being.
Design:
The Self-Directed Biological Transformation Initiative was a quasi-randomized trial comparing the effects of participation in a 6-day Ayurvedic system of medicine-based comprehensive residential program with a 6-day residential vacation at the same retreat location.
Setting:
Retreat setting.
Participants:
69 healthy women (n = 58) and men (n = 11) (mean age ± standard deviation, 53.6 ± 12 years).
Intervention:
The Ayurvedic intervention addressed physical and emotional well-being through group meditation and yoga, massage, diet, adaptogenic herbs, lectures, and journaling.
Outcome measures:
A battery of standardized questionnaires.
Results:
Participants in the Ayurvedic program showed significant and sustained increases in ratings of spirituality (p < 0.01) and gratitude (p < 0.05) compared with the vacation group, which showed no change. The Ayurvedic participants also showed increased ratings for self-compassion (p < 0.01) as well as less anxiety at the 1-month follow-up (p < 0.05).
Conclusions:
Findings suggest that a short-term intensive program providing holistic instruction and experience in mind–body healing practices can lead to significant and sustained increases in perceived well-being and that relaxation alone is not enough to improve certain aspects of well-being.
Introduction
“Well-being is about lives going well.”
W
The field of positive human functioning, including positive psychology and positive psychiatry, 10,11 examines how attributes such as spirituality and gratitude support well-being as compared to the effects of more enduring negative emotions and attributes, which tend to undermine our well-being. 12 –14 Clinically, this work has helped give birth to fields such as psycho-oncology and behavioral cardiology. 15,16 In such clinical populations, positive attributes, such as overall sense of spirituality and hope, are supportive of patients' ability to cope with the challenges of their illnesses as well as particular challenges of acute treatments themselves. 17 –19 For example, in patients with heart failure there is a positive correlation between spiritual well-being and better mental and physical health. 17,20 –22
There are innumerable approaches to enhancing well-being in both healthy and clinical populations, including professional self-management, cognitive-behavioral therapy, mindfulness-based stress reduction, and physical activity, to name a few. 23 –26 As would be expected, efficacy and the maintenance of outcomes across the many approaches to enhancing well-being vary widely.
Ayurveda is the traditional system of medicine of India and emphasizes holistic principles primarily focused on personalized health and well-being. Along with Traditional Chinese Medicine and Traditional Tibetan Medicine, it is receiving increased attention in the medical literature. 27,28 Ayurveda offers a “whole-person” approach to wellness that incorporates practices and therapies to support physical, emotional, and spiritual well-being. Integrative medicine, an approach to medicine that combines mainstream allopathic therapies with evidence-based complementary therapies, is a growing movement in the United States and Europe and in many ways seeks to emulate the holistic approaches and values of traditional medical systems such as Ayurveda. 29,30
Studies have examined the effectiveness of various individual Ayurvedic treatment modalities for medical conditions, including osteoarthritis and rheumatoid arthritis 31,32 and gastrointestinal health. 33 Studies have also examined the effects of individual Ayurvedic treatments in isolation, including massage 34 and herbs, 35,36 on stress, mood, and cognitive performance. A recent noncontrolled pilot study in a small cohort of patients with coronary heart disease examined the effects of an Ayurvedic intervention program that included diet, herbs, yoga, meditation, and breathing exercises and reported improvements in low-density lipoprotein cholesterol and triglycerides. 37
Few if any controlled studies have examined the potential benefits of Ayurvedic approaches to well-being using the more holistic approach advocated by Ayurveda (i.e., not using only isolated modalities found within Ayurveda but rather simultaneous prescription of meditation, yoga, breathing exercises, adaptogenic herbs, oils, massage, diet, and discussion of relevant knowledge related to well-being). The objective of this study was to examine the psychological effects of a brief multidimensional well-being program based on Ayurvedic principles on psychological well-being as compared with a control condition.
Materials and Methods
Study participants and design
Participants were recruited mostly from the greater San Diego and Los Angeles, California, areas, but some participants came from greater distances. Recruitment was via email announcements on the University of California San Diego faculty and staff and Chopra Center for Wellbeing list-servers. Study flyers stated that the week-long Self-Directed Biological Transformation Initiative (SBTI) study would be conducted at the Chopra Center for Wellbeing, located at the La Costa Resort in Carlsbad, California, in order to learn more about the psychosocial and physiologic effects of the 6-day Perfect Health (PH) Program compared with a 6-day stay at the La Costa Resort. The study was approved by the University of California San Diego Institutional Review Board, and all study participants provided written informed consent before participation. The trial is registered on
Eligible participants were healthy English-speaking women and men aged 30–80 years with no current major medical or mental illnesses. Exclusion criteria included being a smoker, pregnancy, estrogen or hormone replacement therapy, a body mass index of 35 kg/m2 or greater, and current use of illicit drugs. Participants were willing to refrain from drinking more than one alcoholic beverage per day during the weeklong stay at the resort. Finally, individuals who had previously participated in the PH program or other Chopra Center programs or a yoga or meditation retreat of any kind within the past 12 months were also excluded from study participation.
As shown in the Consolidated Standards of Reporting Trials flow diagram (Fig. 1), a total of 261 individuals were screened for eligibility, learned details of study involvement, and were asked to consider their commitment and availability before they were enrolled into the study. It was emphasized that this included a commitment to stay in the study even if they were not randomly assigned into their preferred group. Ninety-eight individuals (81% of the total cohort) were randomly assigned (1:2) to the PH group or the vacation (RELAX) group. A group of 23 individuals were assigned to the PH program in a nonrandomized fashion. There were no expenses for participation in the study.
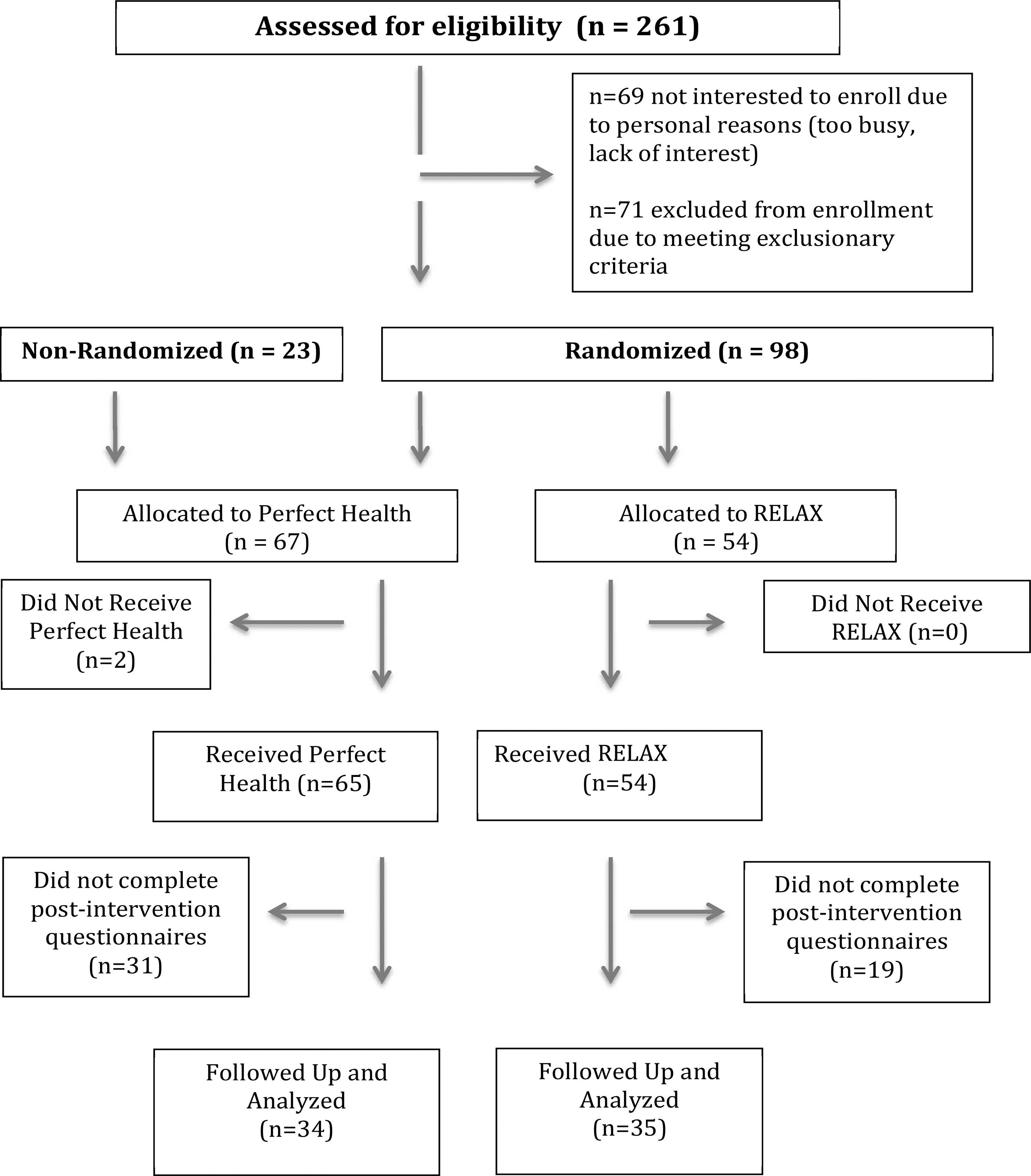
Consolidated Standards of Reporting Trials flow diagram for study participants.
Study interventions
SBTI was a quasi-randomized trial comparing the effects of participation in the 6-day PH program as compared with a 6-day vacation (RELAX) at the same location. The intervention groups were not blinded, and site investigators and study personnel knew to which group participants were assigned. The two groups had no contact with each other during the study and did not know the details of the daily schedule of the other group. Upon arrival at the resort, participants were given a 1-hour orientation meeting with the study team, where they learned about the overall study schedule and procedures and the assessment schedules.
PH program
PH has been offered at the Chopra Center for Wellbeing for approximately 15 years, with approximately 800 individuals taking the course each year. PH is essentially an Ayurvedic immersion program of detoxification and rejuvenation based on core principles from the Ayurvedic system of medicine. The PH program addresses physical, emotional, and spiritual well-being through daily practices and lectures. Key components of the program include physical cleansing through ingestion of herbs, fiber, and oils that support the body's natural detoxification pathways and facilitate healthy elimination; two Ayurvedic meals daily (breakfast and lunch) that provide a light plant-based diet; daily Ayurvedic oil massage treatments; and heating treatments through the use of sauna and/or steam. The program includes lectures on Ayurvedic principles and lifestyle as well as lectures on meditation and yoga philosophy. The PH study group also participated in twice-daily group meditation and daily yoga and practiced breathing exercises (pranayama) as well as emotional expression through a process of journaling and emotional support. During the program, participants received a 1-hour integrative medical consultation with a physician and follow-up with an Ayurvedic health educator. The teachers of the PH program delivered their standard program to the SBTI study participants.
RELAX comparison
Participants randomly assigned to the RELAX group were asked to do what they would normally do on a resort vacation with the additional following restrictions: They were asked not to engage in more exercise than they would in their normal lifestyle and to refrain from using La Costa Resort spa services. RELAX participants were also asked not to drink ginger tea or take Gingko biloba during the 2 days before and during the study week.
Assessments
Data reported here are part of the larger SBTI study, which included biochemical and physiologic assessments that will be reported elsewhere. Participants completed an online battery of standardized questionnaires at three different times: at home, immediately following their respective 6-day program, and at 1-month follow-up at home.
The Spirituality Scale
This 23-item scale assesses beliefs, intuitions, lifestyle choices, practices, and rituals representative of the human spiritual journey. 38 The scale has very strong reliability (0.81–0.93) and validity. 38,39 The Cronbach α was 0.95 for this cohort.
Gratitude questionnaire
The short form of the Gratitude, Resentment and Appreciation Test (GRAT-sf) questionnaire has 16 items and measures trait gratitude, particularly a sense of abundance and appreciation of others. 40,41 As described by McCullough et al., the instrument has strong construct validity and reliability. 41 The Cronbach α was 0.91 for this cohort.
Self-Compassion Scale
This 26-item scale measures the degree to which a person is kind and understanding toward himself or herself, perceives his or her own struggles as part of the larger human experience, and is mindful of negative thoughts and feelings. 42 As described by Neff and Vonk, 42 the instrument has excellent validity and reliability; the Cronbach α was 0.90 for this cohort.
Ryff Scale of Psychological Wellbeing
This 84-item questionnaire assesses well-being and has excellent reliability (>0.76) and validity (>0.63).being. 43 The Cronbach α was 0.98 for this cohort.
Center for Epidemiology Studies-Depression (CES-D)
This 20-item self-report screening tool for depressive symptoms was developed by the National Institute of Mental Health. It has excellent reliability (0.88–0.91) and validity (0.50–0.75). 44,45 The Cronbach α was 0.76 for this cohort.
PROMIS Anxiety Scale
This instrument is part of the National Institutes of Health research initiative, the Patient-Reported Outcomes Measurement System (PROMIS) and Assessment Center. The 8-item PROMIS Anxiety Scale assesses the full range of anxiety symptoms and has excellent reliability and validity (
Other outcomes
Blood pressure (BP), height, weight, and number of months practicing meditation and/or yoga were obtained from all participants.
Statistical analysis
Data analyses (data analysis software, SPSS version 22) included Pearson correlations, one-way analysis of variance (ANOVA), and repeated-measures ANOVA/analysis of covariance (ANCOVA). To address the primary aims regarding potential group differences in well-being, planned comparisons examined potential group differences in treatment effects (i.e., from preintervention to postintervention) and maintenance effects (i.e., from postintervention to the 1-month follow-up assessment). Of the 34 PH participants who completed the postintervention assessments, 20 completed the 1-month follow-up assessments. Of the 35 RELAX participants who completed the postintervention assessments, 26 completed the 1-month follow-up assessments (Fig. 1).
Results
Preintervention characteristics
To address potential preintervention differences among the nonrandomized PH and the randomized PH groups and RELAX group initial one-way ANOVAs examined potential preintervention differences in age (F = 1.2; p = 0.306), body mass index (F = 0.53; p = 0.59), caffeine (chi-square = 5.8; p = 0.271) and alcohol (chi-square = 4.21; p = 0.101) use, sex distribution (chi-square = 0.259; p = 0.891), months of meditating (F = 1.9; p = 0.153), months practicing yoga (F = 0.517; p = 0.599), and the psychological questionnaire data (Fs<0.883; ps>0.41). There were no significant preintervention differences among groups for any of these variables. The nonrandomized and randomized PH participants were therefore combined into a single PH group, and subsequent analyses examined this combined PH group to the RELAX group using 2 × 3 repeated-measures ANOVA/ANCOVA. Correlations were examined between baseline characteristics and outcome measures; systolic BP was correlated with spirituality (r = −0.31; p = 0.011) and therefore was used as a covariate in the analysis of the spirituality data. Controls had higher systolic BP than the nonrandomized PH but not the randomized PH group (F = 2.9; p < 0.05). There were no group differences in diastolic BP (F = 1.1; p = 0.389) or heart rate (F = 0.711; p = 0.547). See Table 1 for an overview of the baseline characteristics by condition.
Values expressed with a plus/minus sign are the mean ± standard deviation.
p < 0.05.
BMI, body mass index; BP, blood pressure.
Intervention effects
Means and standard deviations for all outcome measures by condition are presented in Table 2. There was a significant main effect of time for spirituality (F = 6.61; p < 0.01; partial η2 = 0.106). In addition, a significant group-by-time interaction (F = 8.34; p < 0.003; partial η2 = 0.135) indicated that participants in the PH program showed significant increases in ratings of spirituality compared with the RELAX group, which showed no change (Fig. 2). Planned comparison tests indicated that compared with the RELAX group, the PH group reported a greater initial treatment effect on spirituality from preintervention to postintervention (p < 0.004), as well as a greater maintenance effect between postintervention to the 1-month follow-up (p < 0.05) (Fig. 2). Systolic BP was not significantly related to change in spirituality over time (F = 0.35; p = 0.704).
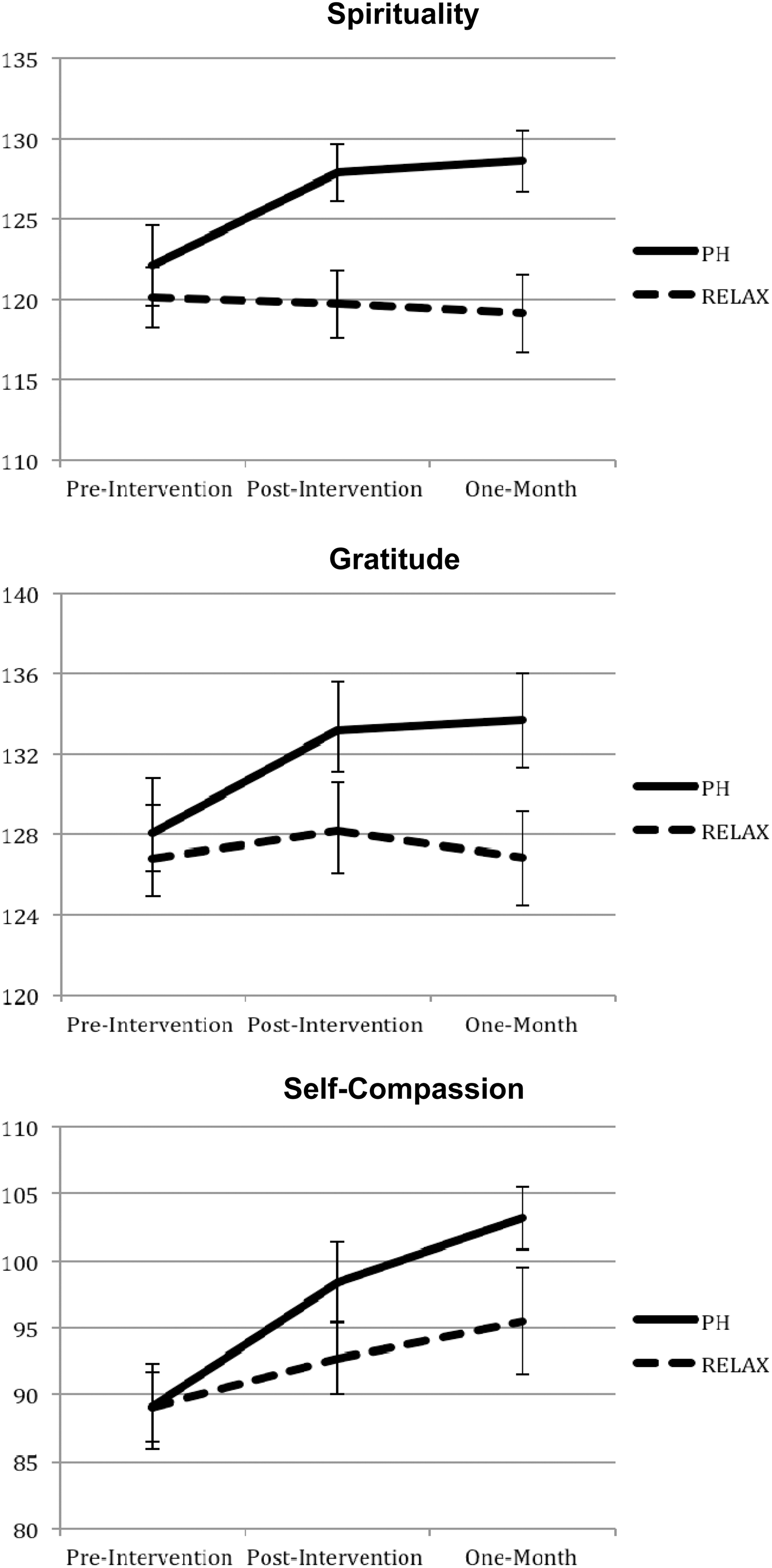
Compared to the RELAX group, the Perfect Health (PH) group reported significant treatment (from preintervention to postintervention) and maintenance (from preintervention to the 1-month follow-up) effects for spirituality and gratitude (p < 0.05), as well as a treatment effect for self-compassion (p < 0.05).
Values are expressed as mean ± standard deviation.
Main effect for time, p < 0.01.
Time-by-group interaction, p < 0.01.
Planned comparisons, p < 0.05.
Main effect for time, p < 0.05.
Time-by-group interaction, p < 0.05.
PROMIS, Patient-Reported Outcomes Measurement System.
Similarly, there were a main effect of time for gratitude (F = 4.23; p < 0.02; partial η2 = 0.100) and an accompanying significant time-by-group interaction effect (F = 3.90; p < 0.05; partial η2 = 0.007). Planned comparisons indicated that compared with the RELAX group, the PH group reported a stronger immediate postintervention treatment effect (p < 0.05) as well as a maintenance effect at the 1-month follow-up (p < 0.05) (Fig. 2).
Ratings for self-compassion showed a significant main effect for time (F = 12.98; p < 0.001; partial η2 = 0.228) with a marginally significant group-by-time interaction (F = 2.42; p = 0.095; partial η2 = 0.052). Planned comparison tests indicated that the PH group reported greater improvements in self-compassion at immediate postintervention (p < 0.05) compared with the RELAX group (Fig. 2). Although both groups continued to improve during the follow-up period, the degree of these improvements did not significantly differ between conditions.
For psychological well-being, there was a main effect of time (F = 13.2; p < 0.01; partial η2 = 0.167), indicating that participants reported improved well-being across the course of the study. There was a marginally significant group-by-time interaction (F = 2.79; p = 0.09; partial η2 = .041) indicating that during the study participants in the PH group improved more in psychological well-being than those in the RELAX group, although this difference was not uniquely discernible in the treatment or maintenance period.
Ratings of anxiety decreased significantly over time in both groups (F = 17.6; p < 0.001; partial η2 = 0.296); the time-by-group interaction was marginally significant (F = 2.54; p = 0.085; partial η2 = 0.057). Planned comparison tests indicated that compared with the RELAX group, those in the PH group reported greater reductions in anxiety symptoms from preintervention to postintervention (p < 0.03). Changes in anxiety during the follow-up period did not significantly differ by condition. Depressed mood did not change significantly across time or by condition (F = 2.08; p = 0.130; partial η2 = 0.047).
Comparison of participants who completed with those who did not complete questionnaires
As shown in Figure 1, some study participants did not complete the postintervention questionnaires. A test for potential preintervention differences in age and sex and questionnaire data indicated that participants who did not complete the postintervention questionnaires had at intake higher scores of depressed mood than those who did complete it (15.8 ± 14.1 versus 10.2 ± 9.31), respectively (F = 5.18; p < 0.05). All other questionnaire scores were similar.
Discussion
This study examined potential well-being benefits of a brief mind–body intervention based on Ayurvedic principles. 27,28 Although most prior studies of Ayurvedic approaches examined only isolated modalities, such as only herbs or only yoga, this study's intervention represented a more thorough Ayurvedic approach based on the principles of Panchakarma, 47 providing multiple Ayurvedic modalities for well-being in a nonclinical population.
Some of the study's most significant and enduring effects were on spirituality and gratitude, with participants in the PH program having sustained increases in both. Spirituality has many connotations and definitions, including the depth of experience of one's own nature and the sense of connectedness with the world. In addition to increased quality of life, 48 spirituality is linked to better health and capacity to cope with the challenges of illness. 17 –19,49 Within this context, there is a growing literature seeking to understand linkages between spirituality and religiousness and well-being in cancer and cardiovascular diseases. 50 We previously showed that spiritual well-being is associated with fewer depressive symptoms in patients with cardiovascular disease. 21 Spirituality is generally considered a foundational resource for maintaining psychological well-being. 51 –54
As with compassion and empathy, gratitude is considered a vital component of spirituality. Gratitude has been defined as a life orientation toward noticing and appreciating the positive aspects of life 55 and can be attributed to internal as well as external sources, such as an animal, person, or nonhuman (e.g., God, the cosmos). We recently showed that patients with heart failure who have more gratitude also have more energy, better mood, and less inflammation. 56 In these same patients, gratitude fully or partially mediated several of the beneficial effects of spirituality on well-being, including better sleep and mood, indicating its vital contribution to the effects of spiritual well-being. In the literature, a primary approach to increasing sense of gratitude is to regularly journal about things for which one is grateful. 57
Self-compassion describes a positive and caring attitude toward ourselves that fosters greater connection with oneself and is associated with more positive cognitive and psychological well-being. 58 Importantly, regarding health, self-compassion is associated with increased practice of health behaviors 59 and has been identified as a modifiable resource to promote healthy attitudes toward aging. 60 Interventions directed to increase self-compassion include mindfulness and acceptance and commitment therapy. 61 –63
Although there are many approaches to understanding well-being, work by Ryff and others has focused more on the psychological components of well-being, 64,65 identifying foundational factors such as quality of ties to others, living in accord with one's personal convictions, and making use of one's talents and potential. 43 Psychological well-being has been linked to better health and better sleep. 64,66 Interestingly, both the relaxation and PH groups showed similar increases in psychological well-being scores, suggesting that the experience of rest and relaxation, and perhaps concomitant detachment from the normal commitments to life, increase sense of psychological well-being. 67
A limitation of this study was the potential for bias in the findings given the high number of participants who did not complete the postintervention questionnaires, with only 50% of those allocated to PH and only 66% of those allocated to relaxation completing the postintervention questionnaires. There was further attrition in completion of the 1-month follow-up assessments. A test for potential meaningful differences in completers and noncompleters found that among the preintervention assessments, noncompleters had higher depressed mood ratings (noncompleters, 14.1 ± 14; completers, 10.2 ± 9; p < 0.05).
For the CESD scale, a score greater than 16 is considered to indicate depressed mood; 44 9 of the study participants (13.2%) who did complete the postintervention assessments scored above this cutpoint at intake (4 in the RELAX group and 5 in the PH group). When these nine participants were examined together (ie, independent of group assignment), there was a significant improvement in their mood: from 28.2 ± 12.8 at preintervention to 16.7 ± 8.9 at immediate postintervention (p < 0.01).
Thus, although because of attrition potential intervention differences in participants with poorer mood at the preintervention intake could not be addressed, in a subgroup of participants with high mood scores there was an overall improvement in mood regardless of group assignment. Anxiety was reduced in all study participants, with a moderately better improvement in the PH group.
Conclusions
Just as there are numerous intervention approaches to enhancing psychological well-being, 23 –26 there are also numerous strategies for enhancing spiritual well-being, including nondenominational spiritual retreats, guided imagery, drumming, journal writing, and nature-based activities. 68,69 The Ayurvedic approach to well-being does not focus exclusively on enhancing any one particular aspect of well-being but rather broadly seeks to support the whole person, to return balance to all aspects of one's life. 28,70 In the current study this approach led to a sustained and significant improvement in sense of spirituality and gratitude, effects not seen in a group of individuals focused solely on relaxation. Overall, the findings suggest that a short-term intensive whole-system medicine program supports a significant and sustained increase in well-being.
Footnotes
Acknowledgments
Supported by the Fred Foundation, the MCJ Amelior Foundation, the National Philanthropic Trust, the Walton Family Foundation, and the Chopra Foundation.
Author Disclosure Statement
P.M. is director of research at the Chopra Foundation. D.C. is the co-founder of The Chopra Center for Wellbeing. The remaining authors have no competing financial interests.