
Abstract
Background:
Chronic kidney disease (CKD) is a progressive disease with an inverse relationship between kidney function and levels of inflammation and oxidative stress. Curcumin and Boswellia serrata have been reported to exert anti-inflammatory effects on the cyclooxygenase and lipoxygenase pathways. Therefore, the purpose of this study was to study the effects of a supplement containing curcumin and B. serrata on eicosanoid derivatives in early stage CKD patients who had not initiated hemodialysis.
Methods:
Sixteen patients with stage 2 and stage 3 CKD (56.0 ± 16.0 years, 171.4 ± 11.9 cm, 99.3 ± 20.2 kg) were randomized into a treatment group with curcumin and B. serrata or a placebo group. The dependent variables prostaglandin E2 (PGE2), 5-hydroxyicosatetraenoic acid, 12-hydroxyicosatetraenoic acid, 15-hydroxyicosatetraenoic acid, and 13-hydroxyoctadecadienoic acid were measured both before and after 8 weeks of supplementation. Results were analyzed by using a repeated-measures analysis of covariance for compliance and body–mass index.
Results:
A significant group effect (p = 0.05), and a trend for Group × Time interaction (p = 0.056) were detected for PGE2. No significant differences were observed for any other variables.
Conclusions:
This is the first article of baseline levels of the dependent variables in early stage CKD, and the first article to show a significant effect of these supplements on PGE2 in early stage CKD. Further studies are needed to determine whether curcumin and B. serrata may be effective means to reduce inflammation in patients with CKD.
Introduction
C
Lipid mediators such as eicosanoids are implicated in various physiological processes, including normal kidney function. Moreover, they are involved in the regulation of several of the aforementioned risk factors and as such, they are identified as potential targets for therapy. 12 These lipid mediators, which include downstream metabolites of omega-6 (n-6) poly unsaturated fatty acids (PUFAs), linoleic acid (LA), and arachidonic acid (AA), are produced via the enzymatic interaction with cyclooxygenases (COX), lipoxygenases (LOX), and cytochrome P450 (CYP450). 12 Thus, it is prudent to pursue therapies that may intervene in the COX and LOX pathways in hopes of slowing the progression of CKD and CVD.
Two alternative therapies that show promise are curcumin and Boswellia serrata. Curcumin has been shown to decrease prostaglandin E2 (PGE2), an AA metabolite downstream of COX, in human blood samples, 13 inhibit PGE2 receptor gene expression in cancer cells, 14 and inhibit increases in PGE2 production in human coronary artery endothelial cells (HCAEC). 15 Specific to renal disease, curcumin has been reported to protect against oxidative injury from ischemia/reperfusion injury in rat kidneys. 16 In addition, curcumin was reported to improve renal function, increase the level of reduced glutathione, decrease tumor necrosis factor-α (TNF-α), and decrease lipid peroxidation in rats with cisplatin-induced nephrotoxicity. 17 In rodent models, B. serrata has also been reported to be renal protective by inhibiting the induction of nitric oxide by lipopolysaccharide in peritoneal macrophages. 18 The effects of B. serrata have been found to be beneficial in ulcerative colitis, 19,20 collagenous colitis, 21 rheumatoid arthritis, 22 and osteoarthritis of the knee 23,24 in human models without kidney disease.
However, to date, to our knowledge, there are no studies on the effects of curcumin or B. serrata on these pathways in CKD patients. In addition, no studies have been conducted by using a combination of curcumin and Boswellia in a readily available over-the-counter supplement in humans. Therefore, the purpose of this article is to report secondary analysis of metabolites downstream of COX and LOX after short-term supplementation of curcumin and B. serrata supplementation in early CKD nonhemodialysis patients.
Materials and Methods
Participation recruitment
The methodology for this study has previously been published with a primary analysis of this protocol on TNF-α, interleukin (IL)-6, glutathione peroxidase, and C-reactive protein, but it will be reviewed in detail here. 25 All participants were recruited from a community health center. Those patients deemed eligible were informed of study requirements and signed informed consents approved by the Institutional Review Board. Experimental procedures for this study conformed to the ethical consideration of the Declaration of Helsinki. Over-recruitment of subjects was performed to account for patient dropout.
Participant eligibility
Patients recruited for this study were older than 18 years of age and had stage 1–5 CKD, completed a medical history questionnaire, and underwent a general medical exam by a physician to determine eligibility. Patients were excluded from the study if they had taken nutritional supplements in the past 3 months, had a malabsorption syndrome, had an illness requiring hospitalization, had a change in body weight ≥10 lbs. in the past 6 months, had a life expectancy ≤3 months, or were pregnant. In addition, patients with a rice allergy were excluded from the study, as the placebo contained rice powder.
Sample size calculation
Previous research using curcumin as an anti-inflammatory supplement in animal models was used to determine the sample size for this study. 16,17,26 –28 Six to eight participants per group were determined to be sufficient to show significant differences between groups in markers of inflammation with a type I error rate of 0.05 and a power of 0.80.
Randomization
A prospective, double-blind, randomized, placebo-controlled trial was conducted in Central Texas at a community health center providing care for the underserved. Participants were randomly assigned to a treatment or placebo group. Study participants and investigators were blinded to the assignment of patients to treatment or placebo groups. Pharmacists at the community health center prepared all medication and supplements and dispensed the medication and supplements to each group. Therefore, the pharmacists were the only individuals who were not blinded to the treatment protocol. Supplement bottles for each group were identical.
The treatment contained curcumin and B. serrata (824 mg purified turmeric extract, 95% curcuminoids, and 516 mg B. serrata extract, 10% 3-acetyl-11-keto-β-boswellic acid). Placebo contained roasted rice powder. All participants received the standard of care and continued to follow the treatment protocol of their treating physician. As all patients were provided the standard of care, it was deemed reasonable and ethical to randomly assign each to a treatment or placebo group. The supplement or placebo was taken in addition to their current medications. The Institutional Review Board and the treating physicians at the community health center approved the protocol.
Experimental protocol
All participants meeting eligibility requirements attended two testing sessions 8 weeks apart. At the initial testing session, the participants underwent measurement for height, weight, heart rate (HR), blood pressure, and waist and hip circumference. Patients were supplied with 8 weeks of supplement or placebo, and they were instructed to ingest one capsule in the morning with breakfast and one in the evening with dinner, in addition to their usual medications. Participants were asked not to change their normal dietary habits during the study. At each testing session, ∼50 mL of blood was collected after a 12-h fast. Participants were given weekly telephone calls as a reminder to take all study supplements and to record any side-effects. Compliance was assessed via pill counting. Patients consuming >80% of their pills were considered compliant. This is standard practice and has been used in other studies. 29,30 Noncompliant participants remained in the study. Their compliance percentage was calculated and recorded. The Modification of Diet in Renal Disease (MDRD) Study equation was used to calculate glomerular filtration rate (GFR). 31
Plasma and serum analyses
Venous blood samples were collected from the antecubital region into four 6 mL heparin tubes by using a standard Vacutainer apparatus and standardized to the same time of day for each sample. Blood samples were allowed to stand at room temperature for 10 min and then centrifuged. The plasma was removed and frozen at −20°C for later analysis. Using human peripheral blood lymphocyte isolation, whole blood was analyzed for the eicosanoids: PGE2, 5-hydroxyicosatetraenoic acid (5-HETE), 12-hydroxyicosatetraenoic acid (12-HETE), 15-hydroxyicosatetraenoic acid (15-HETE), and 13-hydroxyoctadecadienoic acid (13-HODE). All eicosanoids and their related deuterated standards used in this study were purchased from Cayman Chemical Co. (Ann Arbor, MI).
Liquid chromatography-mass spectrometry analysis of eicosanoids
Eicosanoid metabolites were extracted according to the previously published method from Yang et al. 32 Briefly, an aliquot of the 0.5 mL of PBS buffer was added to the cell pellets followed by addition of peroxidation. Before extraction, an aliquot of 10 of deuterated PGE2; 5-, 12-, or 15-HETE; or 13-HODE (100 ng/mL) was added to the samples' internal standards. They were then extracted with hexane:ethyl acetate (1:1, v/v). All extraction procedures were performed under minimal light. Samples were then reconstituted in 100 μL of methanol/0.1% acetic acid (50:50, v/v) before analysis by LC-MS/MS. 33
The eicosanoids of interest were quantified by LC-MS/MS by using an Agilent 6460 triple quadrupole (QqQ) mass spectrometer (Agilent Technologies, Palo Alto, CA) that was equipped with an Agilent HP 1200 binary pump HPLC inlet (Agilent). Eicosanoids were separated using a 2 × 100 mm Kinetex 3 μC18 analytical column Phenomenex (Torrance, CA). The mobile phase consisted of 0.1% formic acid and acetonitrile with 0.1% formic acid only. The column temperature was maintained at 40°C, and samples were kept at 4°C during the analysis. Individual analytes were detected by using electrospray ionization and multiple-reaction monitoring, and the m/z transitions of eicosanoid metabolites were monitored in the negative ionization mode according to a previous publication. 34 The levels of eicosanoid metabolites were quantified by using authentic standard curves and normalized to the amount of protein determined by a Bradford assay (Bio-Rad).
Statistical analysis
The software SPSS 17.0 was used to perform all statistical computation. The outcome variables were PGE2, 5-HETE, 12-HETE, 15-HETE, and 13-HODE. Data were analyzed by using repeated-measures analysis of covariance (ANCOVA) with pill compliance (% pills taken) and body–mass index (BMI) used as covariates. Compliance was used as a covariate due to the levels of compliance within each group, even though there was no significant difference between groups. In light of recent findings suggesting that obesity has an impact on immunomodulation and CKD, and significant differences at baseline between groups, BMI was used as a covariate. 35 One-way ANOVA was used to analyze changes between groups once statistical significance was reported. Effects sizes (ES) were assessed by using partial eta squared. A p-level of 0.05 was used to determine statistical significance.
Results
Attrition
A total of 23 patients consented to participate in the study. One patient was excluded from analysis for the use of the anti-inflammatory prescription medication Methotrexate, one patient was not able to complete the study due to a new diagnosis of colon cancer, and one patient died of congestive heart failure during the study. None of the aforementioned incidents was related to the participation in the study. Dizziness, fainting, and nausea caused two patients to drop from the study, but it was determined that these patients were taking placebo. Two patients did not start the study due to personal reasons. As such, the final sample size completing the study was 16 patients (56 ± 16.0 years, 171 ± 11.9 cm, 99.3 ± 20.2 kg), with a completion rate of 69.6%. 25
Patient characteristics
Patient demographics, which can be seen in Table 1, have been previously reported, with significant differences existing between groups for height (p = 0.05), BMI (p = 0.01), waist circumference (p = 0.03), and hip circumference (p = 0.02). 25 The placebo group had larger BMIs, and larger waist and hip circumferences. However, the treatment group was taller. In regards to age, weight, systolic blood pressure, diastolic blood pressure, resting HR, GFR, pill compliance, and medication use, no significant differences were found. 25 Based on GFR, four participants were in stage 2 CKD and 12 participants were in stage 3 CKD. Compliance for the experimental and placebo groups was >80%, and as previously stated, no significant difference for compliance existed between the groups. 25 However, three patients in each group were <80% compliant, but they completed the study due to intent-to-treat guidelines.
Variables displayed as mean ± SD (Moreillon et al. 25 ).
Statistically significant between groups.
Differences measured by using chi-square test of dependence for categorical variables.
ACEI, angiotensin-converting enzyme inhibitor; BMI, body–mass index; BUN, blood urea nitrogen; DBP, diastolic blood pressure; GFR, glomerular filtration rate; NSAID, nonsteroidal anti-inflammatory drug; SBP, systolic blood pressure.
Side-effect questionnaires for frequency and severity were complete at each testing session and during weekly calls. Only minor side-effects were reported during the study. Three patients reported increased urination, and one patient reported experiencing nausea. 25 Before our previously published report, 25 the only reported side-effect in the literature was nausea. 24
Treatment effects
The baseline level of 13-HODE (0.525 ng/mg protein vs. 0.255 ng/mg protein, p = 0.031) was signficantly higher the treatment group compared with the placebo group as seen in Table 2. No significant differences existed between groups for baseline values of PGE2, 5-HETE, 12-HETE, and 15-HETE. No significant differences existed post-treatment for any dependent variables. Figures 1 –3 depict pre- and post-treatment levels of all dependent variables. Multivariate analysis showed that within the model the covariate factors, compliance and BMI, were not significantly different for any dependent variable. However, between-subject effects for PGE2 were found to be significant (p = 0.05, ES = 0.283) for treatment groups. In addition, a very strong trend for significance was revealed for a Group × Time interaction for PGE2 (p = 0.056, ES = 0.271). Clinical safety values have previously been reported for this study. 25 A significant group effect (p = 0.05) existed for total bilirubin, with the treatment group having higher levels at both baseline and post-treatment time points.
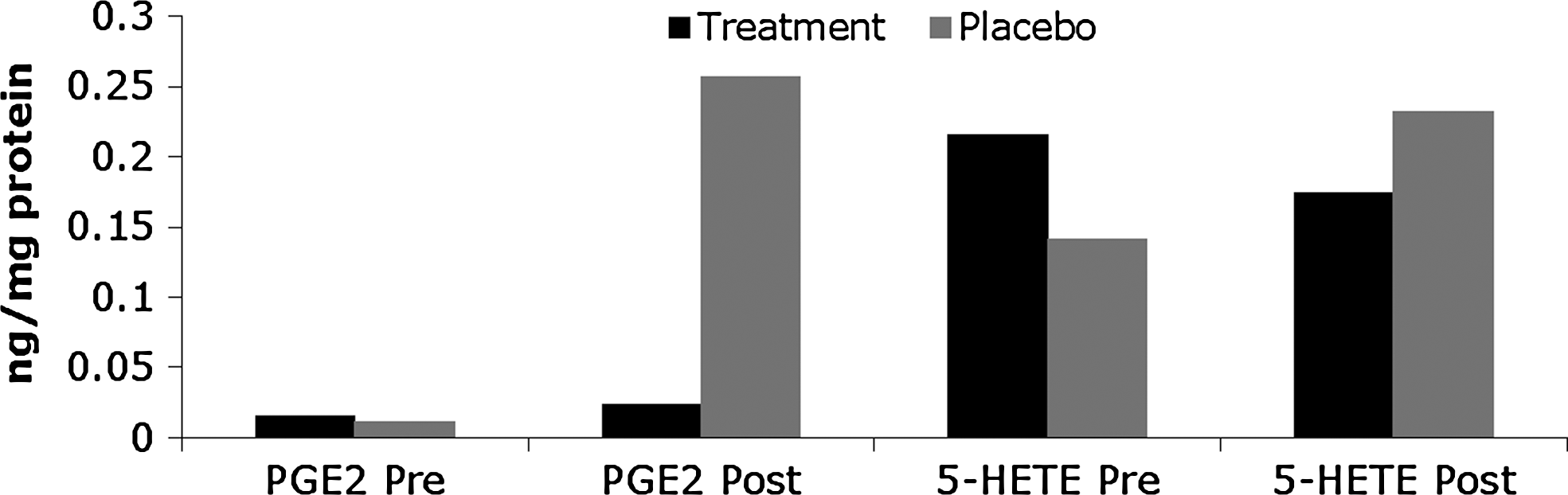
Pre- (baseline) and post-test (8 weeks) circulating levels of PGE2 and 5-HETE. 5-HETE, 5-hydroxyicosatetraenoic acid; PGE2, prostaglandin E2.

Pre- (baseline) and post-test (8 weeks) circulating levels of 12-HETE. 12-HETE, 12- hydroxyicosatetraenoic acid.
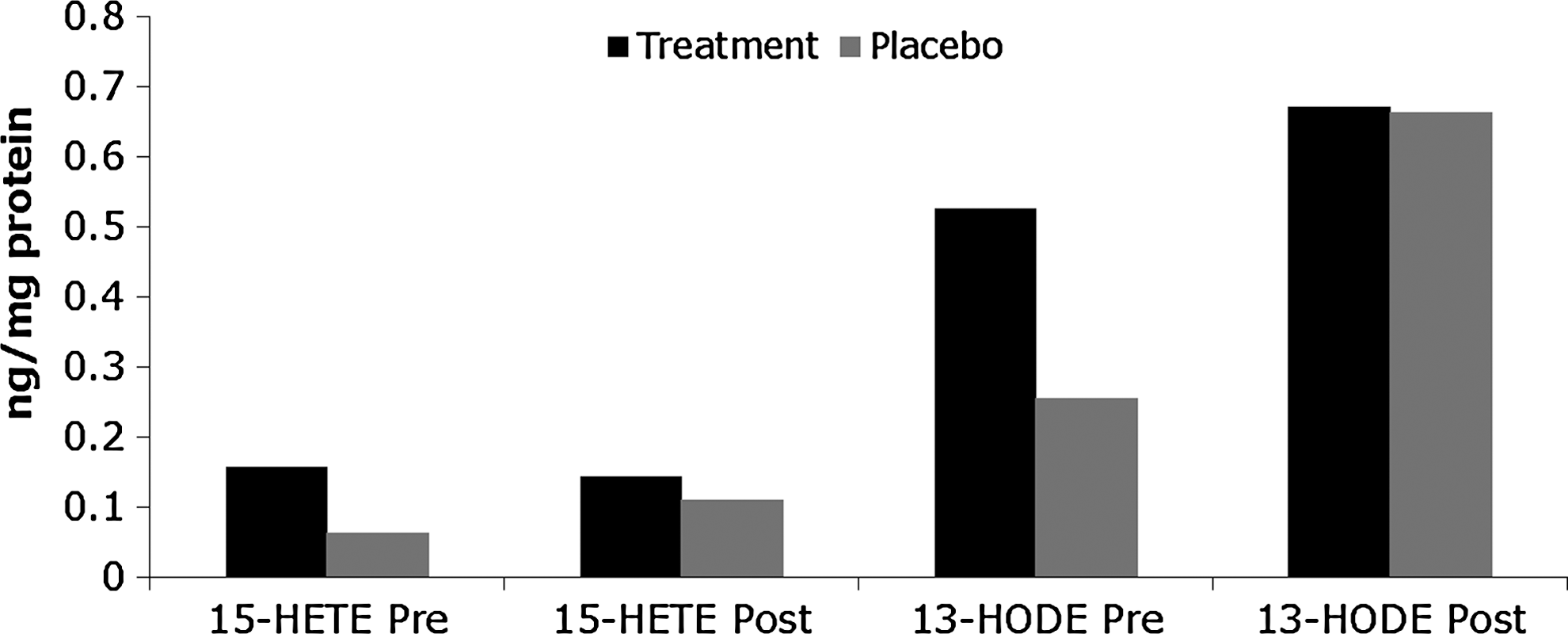
Pre- (baseline) and post-test (8 weeks) circulating levels of 15-HETE and 13-HODE. 13-HODE, 13-hydroxyoctadecadienoic acid; 15-HETE, 15-hydroxyicosatetraenoic acid.
Results are listed as mean ± SD.
Significant group effect (p < 0.05).
Significant difference between groups at baseline (p < 0.05).
5-HETE, 5-hydroxyicosatetraenoic acid; 12-HETE, 12- hydroxyicosatetraenoic acid; 13-HODE, 13-hydroxyoctadecadienoic acid; 15-HETE, 15-hydroxyicosatetraenoic acid; PGE2, prostaglandin E2.
Discussion
CKD is an independent risk factor for CVD, both of which have a myriad of traditional and nontraditional risk factors with varying etiologies that include increased states of inflammation and oxidative stress. 2 Even early stage CKD display marked levels of inflammation. 8 –11 However, CKD is progressive, with an inverse relationship between kidney function and levels of inflammation and oxidative stress. As such, interventions that may attenuate that progression would be valuable. Thus, this study sought to intervene in that progression by having patients with nondialysis early stage CKD supplement with curcumin and B. serrata for 8 weeks, both of which were previously purported to act via COX and LOX pathways.
As this is the only study known to date to examine the effects of curcumin or B. serrata on products from LA and AA via COX and LOX in a human model of CKD, it is difficult to assess how the results of this study compare with others. Only a handful of studies lend themselves to comparison, either for circulating levels of PGE2, 5-HETE, 12-HETE, 15-HETE, and 13-HODE in CKD or fewer still for comparing changes in these variables in response to an intervention that would elicit an effect. However, for the most part, the results in this study supported findings reported in a small number of relevant studies.
The present multivariate analysis found a significant effect for PGE2 between groups (p = 0.05, ES = 0.283), and a very strong univariate trend toward significance for the interaction between Group and Time (p = 0.056, ES = 0.271). In essence, there was a significant difference between the groups in post-treatment PGE2 levels. The treatment group PGE2 levels did not increase to the extent that the placebo group increased. As such, it appears that the supplement may have attenuated the increase in PGE2, which is a product of the n-6 PUFA, AA's enzymatic interaction with COX. PGE2 is produced by the interaction of neutrophils, lymphocytes, and macrophages (cells involved in inflammation and immunity) with injured vascular tissue and is released in response to cytokines. 36 It causes vasodilation and increases vascular permeability. 37 However, it has also been reported to downregulate macrophages and dendritic cells, is released from macrophages after recognition of apoptotic cells along with IL-10 and TGF-β, and may be responsible for activating the release of specialized pro-resolving mediators of inflammation by inducing 15-LOX expression, 35 which may explain this finding in our study.
Our results support the findings of studies using curcumin and B. serrata in regards to PGE2. 13,14,38,39 B. serrata has been used in human models, 19,20 but none of them studied PGE2. However, B. serrata was reported to reduce PGE2 when compared with controls in a rat model of induced arthritis. 38 Curcumin was shown to inhibit the growth of head and neck cancer cells by reducing PGE2 receptor gene expression, 14 as well as to mitigate the increase in PGE2 or PGI2 production in HCAEC. 15 However, there were conflicting results in two clinical trials in humans. A Phase I clinical trial examined curcumin in a dose-escalation study to examine the pharmacology in humans. 13 Patients with advanced colorectal cancer (CRC) consumed as much as 3.6 g of curcumin for a maximum of 4 months. Results indicated that 3.6 g/day decreased inducible PGE2 production by as much as 62% in blood samples, making the authors suggest this dose for further study. A Phase II trial in CRC assessed the effects of oral curcumin, 2 g or 4 g daily for 30 days, on PGE2 on aberrant crypt foci in 44 smokers with ≥8 foci on colonoscopy. 39 Here, curcumin did not decrease PGE2 within the aberrant crypt foci, but it did decrease the number of aberrant crypt foci.
This same study failed to see a decrease in 5-HETE, 39 which conflicts with a report that showed that curcumin decreased 5-HETE in polymorphonuclear leukocytes isolated from blood. 40 In our study, 5-HETE decreased in the treatment group and increased in the placebo group, but these changes were not statistically significant as the changes were relatively small. This could be due to a difference in doses of curcumin. Carroll et al. and Sharm et al. 13,39 used curcumin doses for a maximum of 4 g. The doses of curcumin in this study were far below that level.
Interestingly, for 12- and 15-HETE and 13-HODE, the present study appears to be the only intervention examining the effects of curcumin or B. serrata in humans with CKD. Searches produced several reviews on related topics, but they failed to produce any relevant clinical trials or animal studies for the effects of curcumin and B. serrata on any of these three dependent variables specifically, in any model of CKD or other pathological states in humans. Therefore, comparisons are limited to one study on human platelets. Synthetic curcuminoids on human platelets resulted in an inhibition of 12-LOX, which is responsible for 12-HETE production. 41 Similar to PGE2 in the present study, 12-HETE increased for both groups and increased in placebo to a greater extent than the treatment group, but this was not significant. Fifteen-HETE decreased in the treatment group and increased in the placebo group, but again, these changes did not result in any statistically significant findings. Thirteen-HODE displayed a nonsignificant increase in both groups, with the placebo increasing to a greater extent than the treatment group. The significant difference in 13-HODE that existed at baseline did not exist after completion of the supplementation.
From these findings, it would appear that 8 weeks of supplementation appear to have a slight impact on the inflammatory process, as assessed by eicosanoids PGE2, 5-HETE, 12-HETE, 15-HETE, and 13-HODE, mainly through the effects of PGE2, as this was the only variable that resulted in a significant finding from this intervention.
Thus, although most changes in the present study were not found to be statistically significant, the secondary analysis performed in this study reveals novel information not previously reported in the literature. First, this is the only study to date to report levels of PGE2, 5-HETE, 12-HETE, 15-HETE, and 13-HODE in early stage CKD (stage 2–3). As expected, these levels were less than levels of proinflammatory LOX-derived HETEs reported in advanced CKD and ESRD. 42 –44 Second, this is the first study to report significant findings regarding the use of curcumin and B. serrata on downstream targets of AA in the same population.
Though novel findings are reported, several shortcomings previously reported in the literature were present in this study. 25 Inferences and statistical significance can be difficult to assess with small sample sizes. In addition, compliance with the protocol was problematic, as was the significant difference in BMI between the treatment groups at baseline. Both of these shortcomings were accounted for by using statistical adjustment via repeated-measures ANCOVA. It is also entirely possible that medications used by the participants in this study influenced the outcome of the study though there was no difference in medication usage between groups. Furthermore, the dose of curcumin and B. serrata in this may have been too low so as to exert a significant change on some variables. Lastly, as diet was not standardized in this study, it is plausible that the diet of the participants impacted the outcomes in regards to these dependent variables. It is well accepted that varying ratios of n-3:n-6 PUFAs affect inflammation to varying degrees.
Conclusion
As was previously reported regarding this study, 25 this secondary analysis supports the finding that inflammation is increased in early stage CKD. However, the levels of the dependent variables in this analysis were not as great as in those with advanced CKD in previous studies. This was the first article of baseline levels of some of these n-6 PUFA derivatives, and the first article to show a significant effect of these supplements on PGE2 (p = 0.05, ES = 0.283) in this population. Therefore, larger randomized control trials, using greater doses of the supplements, are needed to investigate the use of curcumin and B. serrata in CKD patients to further elucidate the usefulness of these supplements in mitigating inflammation in early stage CKD.
Footnotes
Acknowledgments
The authors want to thank the staff of the Family Health Center for making this study possible. Special thanks are due to CraShanta Evans, Toni Marshall, and Linda Garcia. The supplements used in this study were donated by Life Extension, Inc.
Author Disclosure Statement
No competing financial interests exist.