
Abstract
Introduction/Aim:
Interest in the gut–brain axis and emerging evidence that the intestinal microbiota can influence central nervous system function has led to the hypothesis that probiotic supplementation can have a positive effect on mood and psychological symptoms such as depression and anxiety. Although several human clinical trials have investigated this, results have been inconsistent. Therefore, a systematic review and meta-analytic approach was chosen to examine if probiotic consumption has an effect on psychological symptoms.
Methods:
The online databases PubMed, Scopus, and the Cochrane Library were searched for relevant studies up to July 2016. Those that were randomized and placebo controlled and measured preclinical psychological symptoms of depression, anxiety, and perceived stress in healthy volunteers pre and post supplementation with a probiotic were included. To control for differences in scales of measurement, data were converted to percentage change, and the standardized mean difference between the probiotic and control groups was investigated using Revman software. A random effects model was used for analysis. Heterogeneity was assessed using the I 2 statistic. Quality assessment was undertaken using the Rosendal scale.
Results:
Seven studies met the inclusion criteria and provided data for nine comparisons. All studies passed the quality analysis. The meta-analysis showed that supplementation with probiotics resulted in a statistically significant improvement in psychological symptoms (standardized mean difference 0.34; 95% confidence interval 0.07–0.61, Z = 2.49) compared with placebo.
Conclusion:
These results show that probiotic consumption may have a positive effect on psychological symptoms of depression, anxiety, and perceived stress in healthy human volunteers.
Introduction
T
Given the cogent impact of gut bacteria on physiological health, the conceptualization of the term microbiota–gut–brain axis has emerged. 4 –6 The microbiota–gut–brain axis refers to the two-way communication network between the GI and the CNS. 7 This term has been used to explain the relationship between gut microbes, their metabolites, and the sympathetic and parasympathetic branches of the autonomic nervous system. 8 There is a clear element of communication between the gut microbiota and the CNS, with the GI tract acting as a platform. Together they form what can be described as a complex reflex network, which consists of afferents that extend the centripetal cortical structures of the CNS and efferents that innervate smooth muscle in the GI tract wall. 3 Evidence suggests that the composition of the microbiota within the gut plays a role in mental illnesses involving the CNS. 4 It is postulated that these effects manifest via the microbiota–gut–brain axis. It has been demonstrated that bacteria have the capacity to generate both neuromodulators as well as neurotransmitters, including GABA, serotonin and noradrenalin, dopamine, and acetylcholine. 9 –11
Probiotics can be described as living organisms that benefit the health of the host, when ingested at adequate levels. 12,13 These living microorganisms are capable of balancing microbial communities and suppressing the growth of pathogens. Probiotics act as immunomodulators by mediating cytokine secretion through signaling pathways such as nuclear factor kappa-light-chain-enhancer of activated B cells (NFκB), which results in proliferation and differentiation of immune cells and epithelial cells. Their impact on epithelial cells may help protect the intestinal barrier. 14 Probiotics also produce neuroactive and neuroendocrine molecules, which can act on the CNS to alter behavior. 4 Recent experimental studies have also shown probiotics to reduce anxiety-like behavior in animals, reverse behavioral effects related to depression in rats post-myocardial infarction, 15 and have beneficial psychological effects in humans. 16 Although the mechanism by which probiotics exert these effects is yet to be completely elucidated, it has been suggested that their metabolic products may affect the host metabolism, impacting brain function, and also through immunological mechanisms by lessening the effects of oxidative stress and inflammatory cytokines. 4
While a number of animal trials have investigated the impact of probiotic consumption on behavior and mood, fewer clinical trials have specifically investigated the impact of probiotic supplementation on psychological symptomology in the general population. This study aimed to pool data from similar studies available to date and used a meta-analytical approach to examine any effects of probiotic intervention on anxiety, depression, and perceived stress.
Methods
Article search
Searches were conducted independently by two researchers via PubMed (MEDLINE), Cochrane Library (Central), and Scopus databases up to July 2016, using combinations of the following search terms: “probiotic, gut, or microbio*,” along with “mood, neuro*, or psych*,” and “gut-brain axis” without imposing time limitations. Results were filtered where possible for human clinical trials. In addition, reference lists of selected studies were screened for additional studies of relevance. Initial screening of studies was conducted by two researchers based on the titles and abstracts. The next phase involved a review of abstracts and an examination of the full text based on the eligibility criteria. The decision regarding the inclusion or exclusion of articles was made through agreement between the two researchers. In case of any disagreement between the first two researchers, a third researcher was involved in decision making. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement was followed as a guideline for conducting and reporting this systematic review and meta-analysis. 17
Study eligibility and selection
Trials for consideration had to be randomized, double-blind controlled trials that used probiotic as a supplement and reported on key aspects of mood and mental state, particularly preclinical psychological symptoms of anxiety, depression, and perceived stress in adult healthy volunteers (aged ≥ 18 years). Selected trials provided pre- and post-intervention measurement data for calculation of overall effect. Studies were excluded if they supplemented the mixture of probiotic and other nutrients. Review articles and conference abstracts with no accessible full text in English were also not included in this systematic review and meta-analysis. Issues such as pregnancy, smoking, food allergy, lactose or gluten intolerance, cardiovascular, renal, hepatic or lung disease, and other severe systemic diseases or inflammation were all factors for exclusion of participants from the trials. Dietary intake such as vitamin or antioxidant supplements, antibiotics, recreational drugs or some other prescribed medications, or high amounts of caffeine also precluded participation.
Figure 1 provides details of the selection process. Quality assessment was undertaken by two reviewers using the Rosendal scale, 18 and disagreements were resolved by discussion. An overall Rosendal score of 60% was regarded as an excellent methodology quality. 19 A Rosendal score of <50% was chosen as a cutoff point for the exclusion of studies. The highest Rosendal score of 94% belonged to Messaoudi et al. study, 20 and Steenbergen et al. 21 had the lowest Rosendal score of 62%.
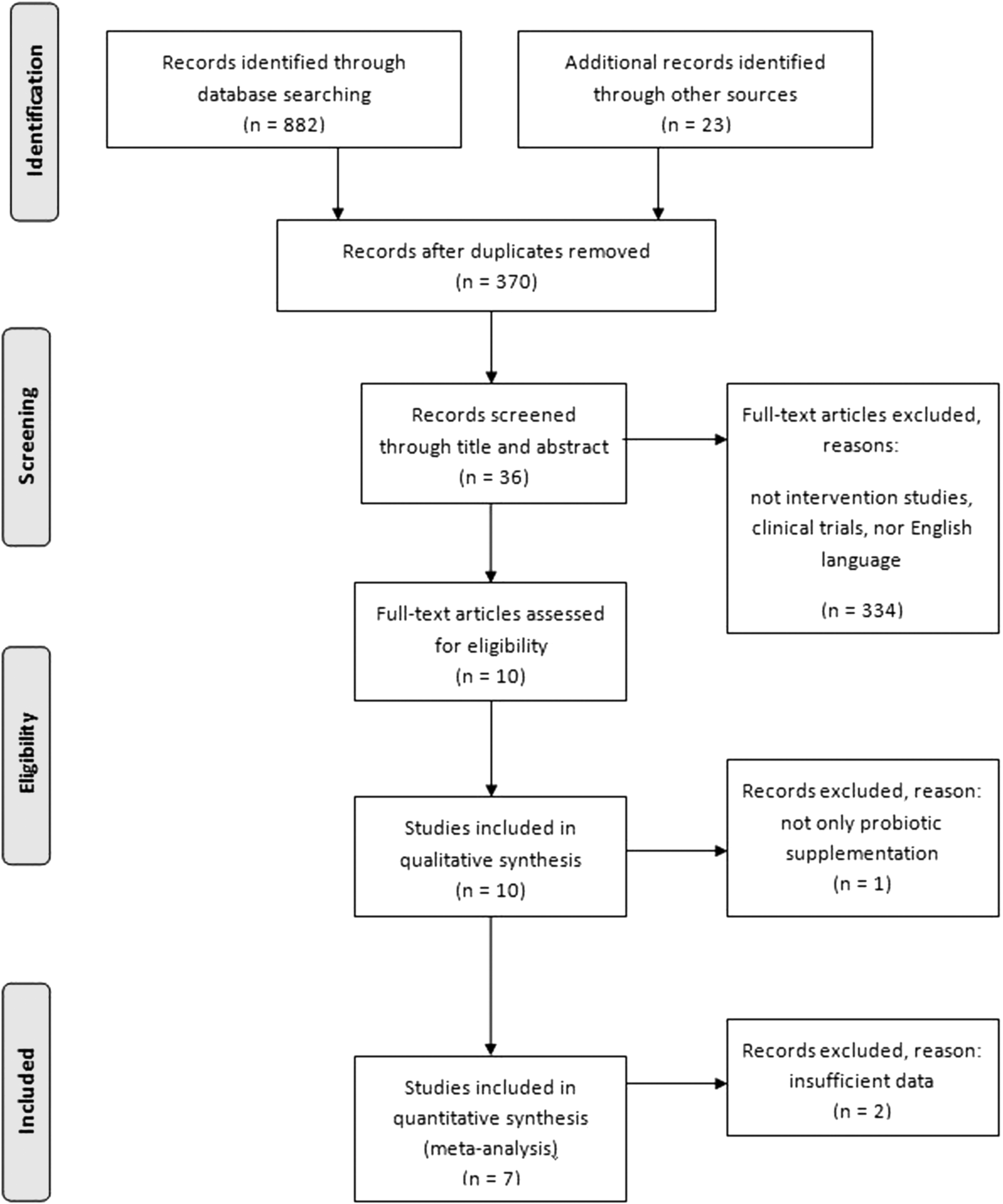
Procedure for selection of relevant studies.
Data handling and statistical analyses
Key aspects of mood and cognitive functioning were examined. Included studies measured multiple psychological aspects, and to minimize heterogeneity of the studies, it was decided to analyze perceived stress, anxiety, and depression, as they were common measures in all studies. RevMan (v5.3) software was used to perform meta-analysis of the data. A random effects model was applied due to expected heterogeneity between studies. 22 Data were extracted using an Excel data extraction tool. To control for differences in scales of measurement, effect was calculated using a percentage change in means from baseline to end-of-study in each of the probiotic and placebo groups. Two studies directly reported results as percentage change in mean (Diop et al. 23 ) or mode (Messaoudi et al. 20 ). Where necessary, standard error data were used to calculate standard deviations. Standard deviations were expressed as a percentage of the change. Due to the differences in scales used to measure perceived stress, anxiety and depression, the standardized mean difference (SMD) was used as the summary statistic to determine the effect size. Heterogeneity was assessed using the I 2 statistic, with >50% representing substantial heterogeneity and >75% representing considerable heterogeneity. 22 A sensitivity analysis was performed by removing one study at a time to determine whether the results could have been influenced by a single study.
Dimensions of psychological symptoms
The choice of particular dimensions of psychological symptoms was based on their common measurement, and they fell into three categories—anxiety, depression, and stress—although researchers used a variety of scales for these measurements. Stress was measured by two commonly used validated self-report measures: the Perceived Stress Scale (PSs) 24 –26 and the State–Trait Anxiety Inventory (STAI), 27 as well as a 10 centimeter Visual Analog Scale (10-cm VAS scale), which has been used extensively to rate pain and other symptoms, 28,29 and a daily web-based stress-scale survey (0 = “no stress”; 10 = “extreme stress”) 30 based on cold/flu symptom intensity. Depression was measured using the Leiden Index of Depression Sensitivity—revised (LEIDS-r), 31 a self-reported questionnaire that measures vulnerability to depression. 32 Anxiety and depression were measured together by the Hospital Anxiety and Depression Scale (HADs), 33 which has been validated previously, 34,35 and all three were measured together by the widely used Depression Anxiety and Stress Scale (DASS) screening tool. 36,37 Details of measurement scales are described in Table 1.
Messaoudi subjects assessed using HADs.
Messaoudi subjects assessed using PSs.
BMI, body mass index; DASS, Depression Anxiety and Stress Scale; HADs, Hospital Anxiety and Depression Scale; LEIDS-r, Leiden Index of Depression Sensitivity—revised; PSs, Perceived Stress Scale; SDS, Self-Rating Depression Scale; SI, symptom intensity; STAI, State–Trait Anxiety Inventory.
Information on supplement
Four trials studied multiple selected commensal bacteria species and/or strains, mostly including lactobacilli and bifidobacteria, 20,23 but also Lactococcus, 21 and one including Streptococcus. 38 Langkamp-Henken et al. 30 investigated individual bacteria strain of Bifidobacterium bifidum R0071, following positive results from an earlier study of these species in a combined bacterial formulation. 39 Both Takada et al. 40 and Kato-Kataoka et al. 41 trialled Lactobacillus casei Shirota strain YIT 9029. Viability of probiotic formulations was checked by the producer and in one study by an independent laboratory. 21 All formulations displayed a good safety profile, with no adverse side effects during the treatment period. Please see Table 1 for formulae and dosages.
Results
Of the total 882 studies initially identified, nine fulfilled the inclusion criteria. All studies passed quality assessment at >50% (see Appendix). Two were later excluded, as data were insufficient for the combined analysis. 42,43 Seven studies were retained in the final analysis. One study, Mohammadi et al., 38 trialed parallel supplementation of two different probiotic preparations on separate subject groups, and another, Messaoudi et al., 20 provided results from two separate psychological measurement tools, providing a total of nine available statistical results for meta-analysis.
Overall, the meta-analysis showed that supplementation with probiotics resulted in significantly reduced preclinical psychological symptoms of anxiety, depression, and stress in healthy individuals (SMD = 0.34, 95% confidence interval [CI] 0.07–0.61, p = 0.01). There was considerable heterogeneity at 67% (Fig. 2).
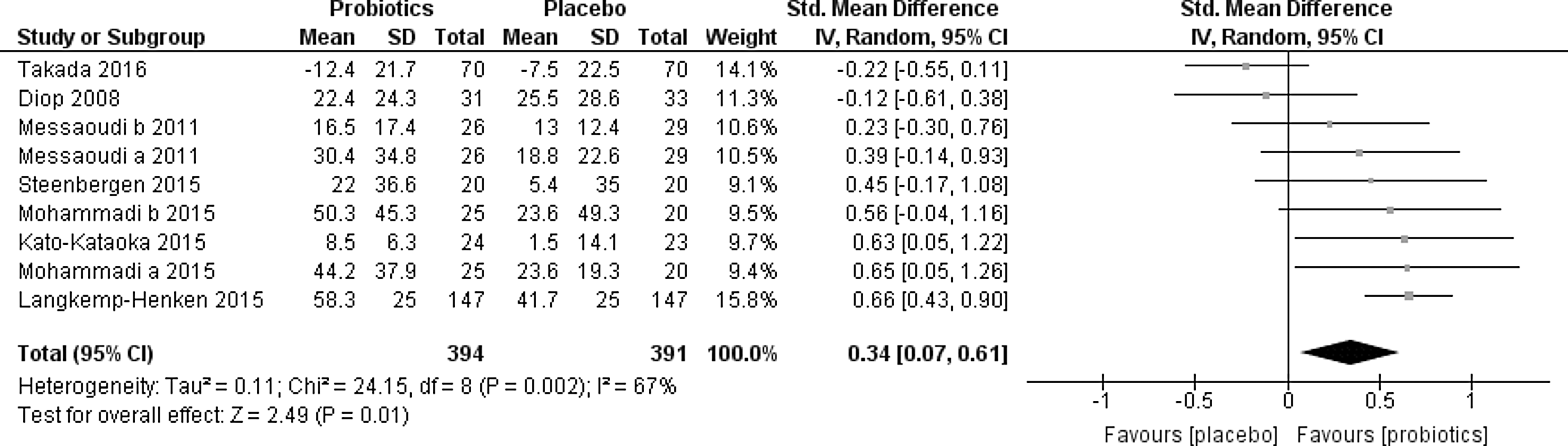
Data and forest plot of probiotic supplementation and placebo for all included studies.
Sensitivity analysis
To evaluate the effect of individual studies on the overall meta-analysis results, a one-by-one sensitivity analysis was conducted. There was no marked change in the pooled SMD or 95% CI, and results remained significant when each study was individually excluded. Therefore, no individual study had excess influence on the pooled results of the meta-analysis.
Discussion
The purpose of this systematic review and meta-analysis was to examine the effect of probiotic consumption on psychological symptoms. The results from this pooled analysis of 394 participants suggest that supplementation of healthy adult subjects with combinations of particular probiotic species may have advantageous effects on mental health by lessening the psychological symptoms of perceived stress, depression, and anxiety.
These results contrast with those of Romjin and Ricklidge, who, after systematically reviewing 10 randomized controls of the effect of probiotics on psychological outcomes and psychiatric symptoms by narrative synthesis, concluded that there was limited evidence for their effect. 44 There are a number of important differences between the present study and that of Romjin and Rucklidge. The present study chose studies examining anxiety, depression, and stress in healthy adult non-smoking participants without systemic or inflammatory disease, while Romjin and Rucklidge chose all psychiatric symptoms including schizophrenia in trials that included smokers and those with chronic inflammatory and other conditions such as irritable bowel syndrome (IBS) and rheumatoid arthritis. 44 The pooled results in the present study were statistically analyzed, while Romjin and Rucklidge produced a narrative synthesis. 44 Only one of the studies included in the present analysis was also included in Romjin and Rucklidge.
There is good evidence from animal and human studies that probiotics may have psychological health benefits in humans (recently reviewed in Liu et al. 45 and Grant and Baker, 46 who also examined the effect of exercise). However, it is possible that this effect may be reduced in individuals suffering from existing chronic conditions, particularly those associated with altered gut microbiota, termed dysbiosis, immune function changes, and psychological comorbidities such as IBS 47,48 and rheumatoid arthritis. 49,50 In conditions with psychoneuroimmunological disturbances, supplementation with probiotics may have limited effect, and may help explain the difference between the present results and those of Romjin and Rucklidge. McFarland 51 performed a systematic review of the use of probiotics in certain disease states and reported that while some species changed the composition of the microbiota in chronic disease states, the disease state made it difficult to determine a normal baseline microbiota, and thus any potential positive effect of treatment. On the other hand, there was significant evidence for the ability of probiotics to restore normal microbiota in situations of acute disruption (e.g., antibiotic exposure), with 12 probiotics out of 15 treatment arms (10 studies) showing evidence for restoration from normal baseline. 51
None of the studies in this pooled analysis examined the microbiota at baseline or after treatment. It is important to note that there is significant interindividual variation of species of microbes in the gut and other areas, and no standard definition of “normal” microbiota. 51 Nevertheless, the absence of chronic disease in the participants of this analysis likely excludes the existence of dysbiosis. It has been shown that in healthy individuals, the use of certain strains of probiotics have a small to medium effect (SMD = 0.34, where SMD 2 = small and SMD 5 = medium 52 ) on subclinical psychological symptoms, and therefore may have benefits in a preventative capacity.
Current understanding suggests that these effects are mediated via the gut–brain axis. 45,53 The gut–brain axis ensures maintenance of GI homeostasis and digestion. 3 This system involves endocrine, immune, and neuronal afferent signaling from the gut, conveying information from the gut lumen to the brain stem via extrinsic vagal afferents and to the spinal cord via spinal afferents. At the same time, mechanical stimuli such as stretch, pressure, distortion, and shearing forces within the GI tract can also directly activate spinal, vagal, and intrinsic primary afferents. 3 Impairment of this axis can result in a number of pathophysiological consequences, including inflammatory GI disorders, obesity, and eating disorders, along with effects on brain function, cognition, and behavior, often resulting in psychological disorders. 1 Additionally, physical and psychological stressors can alter the composition and metabolic activity of the gut microbiome in a “top-down” brain-to-gut mechanism via the autonomic nervous system and systemic circulation. 3 These mechanisms are not completely understood. However, they are supported by results of studies that have examined the effect of stress mediators such as catecholamines on the microbiome directly and via interactions with the intestinal mucosa, 45 and also the knowledge that a number of bacterial species are responsive to stress hormones. 54
As the gut microbiota has been seen to have a direct significant impact on the gut–brain axis, this study considered the therapeutic potential for live probiotic bacteria due to their direct interaction with the gut microbiota. 12,13 Potential favorable effects of probiotics include their ability to modify the composition of the mucosa to prevent the adherence of pathogens, ameliorating the state of the immune system. 55,56 The human intestinal tract supports the largest concentration of immune cells within the human body, along with 500 million neurons. 57 It has been suggested that certain depressive symptoms may derive from activation of the inflammatory immune system through the secretion of signaling molecules such as proteases, histamine, serotonin, and cytokines by immune cells within Peyer's patches and the gut epithelium. 45 These molecules are believed to act via receptor activation in a paracrine fashion on vagal and spinal afferents to the CNS. 45 Additionally, luminal factors such as nutrients, toxins, and antigens are said to activate enteroendocrine cells, leading to the release of gut peptides, hormones, and neuropeptides, all of which reach brain targets systemically. 3
The literature suggests different mechanisms by which probiotics could affect CNS function. In general, the modification of normal gut microbiota and regulation of multiple signaling pathways, including neural pathways, immune pathways, and metabolic pathways, are proposed as potential mechanisms of probiotic action. 45 Some mental disorders such as anxiety and depression are associated with increased inflammatory activation. 58 Therefore, altering microbial composition of the gut, decreasing pro-inflammatory cytokine production, reducing inflammation, and having a favorable effect on gut–brain signaling as a result is one of the possible ways to change the emotional state. 58,59 Given the two-way communication between the immune system and the CNS, probiotics are also capable of increasing the integrity of the gut wall, which is the result of gut-microbiota composition improvement, and it leads to lower immune activation in response to bacterial translocation. 60
A number of preclinical studies have been carried out in an attempt to characterize the bidirectional interactions of the gut–brain axis. These studies have been successful in identifying potential links between changes in gut flora and changes in affective behaviors in animals, reviewed in Wang et al. 7 Several probiotic species have been confirmed to produce neurotransmitters such as acetylcholine, serotonin, and GABA, 61 which act both directly and indirectly on CNS targets. Information from the heart, lungs, pancreas, liver, stomach, and intestines are delivered tonically to the brain via sensory fibers in the vagus nerve. 62 Bravo et al. identified the vagus nerve as a major constitutive of this communication pathway, and confirmed that neurochemical and behavioral effects were not found in vagotomized mice. 63 They established that the probiotic effects of Lactobacillus rhamnosis on the host's GABA receptor expression were absent without an intact vagus nerve. These results confirm that in animals, experimental changes made within the gut microbiota can have an effect on emotional behavior and related brain systems. 64
In another animal study, D'Mello et al. were able to demonstrate that treatment with a high-potency probiotic medical food formulation,VSL#3, can reduce sickness behavior development in mice without affecting severity of liver disease, gut microbiota composition, or gut permeability. 65 This attenuation of sickness behavior was associated with lower microglial activation and cerebral monocyte infiltration, and paralleled by a decrease in circulating TNF-α. Germ-free rodent studies have also demonstrated the influence of gut microbiota on the development of emotional and social behaviors, stress- and pain-modulatory systems, and brain neurotransmitter systems. 66 This influence appears to be of particular importance during critical neurodevelopmental windows and therefore may have an effect on the lifelong functionality of these systems. 67 Probiotics and antibiotics are also known to exert modulatory effects on some of these measures in adult animals. 66 It has also been shown that many bacterial metabolites can act as epigenetic modifiers. 68 This is of significance, as the role of epigenetic mechanisms in influencing brain function and behavior is shifting the understanding of the ways by which probiotics may attenuate psychological symptoms. 69
Limitations
To the best of the authors' knowledge, this study is the first to review the effect of probiotics on symptoms of anxiety, depression and stress on normal healthy volunteers systematically by pooling the results of individual control trials. This study investigated the effect of different species and durations of probiotics on specific preclinical psychological symptoms. However, the current review has several limitations that should be discussed. There was significant heterogeneity as several factors varied across the studies. Supplement administration varied between the included studies in terms of the duration, probiotic type and dose (CFU), and the type of the carrier. The number of studies and sample sizes are also small, which can lead to lower confidence in the meta-analytic results. Moreover, as included studies were conducted in healthy participants, they are not translatable to participants with diagnoses of existing psychological conditions such as anxiety or depression. The baseline characteristics of participants varied, which may have influenced the meta-analysis outcome, and this should be considered in future studies. In particular, there is the issue of variance in a healthy gut microbiome, which may influence response to supplementation with particular strains of probiotics. As no assays are currently able to detect the complete microbiota, this must be acknowledged as a current limitation in the field. 51 A further limitation is the different measures used for anxiety, depression, and stress. For anxiety and depression, all studies used well established and previously validated measures, although they differed between studies. For stress, two studies used 1–10 scales to describe stress. 24,31 One study considered cold/flu symptom intensity as the stress measure—a further limitation, as it would be difficult to distinguish between physiological symptoms and psychological symptoms. 30
Conclusion and Future Directions
The results of this review and meta-analysis suggest that a probiotic intervention may have an advantageous effect on mental health by reducing psychological symptoms including anxiety, depression, and perceived stress in healthy adult volunteers. These results support the notion that probiotic supplementation may have an influence on certain cognitive functions known to determine susceptibility to mood disorders. It has become clear that the gut microbiome has a number of important roles within the body, and appears to be intricately involved with both the systemic immune system as well as the nervous system. For these reasons, the gut microbiome presents as a potential target for the treatment of cognitive and mood disorders. The studies and discussion outlined in this review indicate the increasing need to understand the gut microbiome better and the role it plays in communication via the gut–brain axis, but also highlights the need to understand individual variation. Future studies may allow for the development of novel probiotic treatment strategies for gastrointestinal-related disorders that are associated with impaired communication between the gut and the brain. Such studies will require larger sample sizes and participants with various health conditions, which are matched in baseline characteristics, including microbiome features, to confirm the health benefit and role of probiotics on psychological symptoms. In particular, studies need to be carried out to detect benefits of specific strains as effects may be strain specific.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
| Authors (References) | Eligibility a | Randomization b | Method for randomization c | Sample size calculated d | Pre-trial conditions e | Baseline measures f | Blinding of subjects g | Blinding of investigators h | Method and evaluation of blinding i | Non-completers described j | Stats described k | Measures and variability described l | Between-group stats comparisons m | Adverse effects described n | Reproducibility reported o | Familiarization performance p | % Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diop et al., 2008 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 69% |
| Langkamp-Henken et al., 2015 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 94% |
| Messaoudi et al., 2011 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 75% |
| Mohammadi et al., 2015 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 81% |
| Steenbergen et al., 2015 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 62% |
| Kato-Kataoka et al., 2016 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 0 | 0 | 73% |
| Takada et al., 2016 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 75% |
A clear description of the inclusion and exclusion criteria was provided.
The trials were randomized.
The method used to generate the random allocation sequence, including details of any restrictions (e.g., blocking, stratification) was described.
Sample size was justified (e.g., by power calculation).
Attempts were made to control and/or monitor pretrial condition (e.g., diet, exercise).
Design incorporated measures of important baseline variables.
There was blinding of all subjects.
There was blinding of all investigators involved in the trials.
Both the method of blinding and the evaluation of the successfulness of blinding were described.
Details were provided regarding the inability of subjects to complete study requirements.
Statistical methods used to compare groups for primary outcome measure, and methods for additional analyses, such as subgroup analyses and adjusted analyses, were described.
Both point measures and measures of variability for the primary outcome measure were provided.
The results of between-group statistical comparisons were reported for the primary outcome measure (e.g., an estimated effect size), and its precision (e.g., 95% confidence interval).
The method used to assess adverse effects was reported.
Reproducibility of the primary outcome measures was reported.
If a performance test was used, a familiarization trial was conducted.