
Abstract
Objectives:
To investigate the effects of a yoga program on menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea.
Design:
Single-blind, randomized controlled trial.
Participants:
40 randomly selected undergraduate nursing students, with 20 each assigned to an exercise or a control group.
Intervention:
The participants engaged in a yoga program for 60 minutes once a week for 12 weeks. The program consisted of physical exercise combined with relaxation and meditation.
Outcome measures:
Menstrual cramps and menstrual distress levels were measured by using the Visual Analogue Scale for Pain and the Menstrual Distress Questionnaire, respectively. Data were analyzed by using the Kolmogorov-Smirnov and Shapiro-Wilk normality tests, t-test, chi-square test, logistic regression analysis, and multivariate analysis of variance (SPSS program).
Results:
Menstrual pain intensity (group difference, −0.94; 95% confidence interval [CI], −1.47 to −0.42; p = 0.001) and menstrual distress (group difference, −1.13; 95% CI, −1.43 to −0.82; p < 0.0001) scores decreased significantly in the experimental group compared with the control group.
Conclusions:
These findings indicate that yoga interventions may reduce menstrual cramps and menstrual distress in female undergraduate students with primary dysmenorrhea.
Introduction
M
Menstrual cramps are generally defined as colicky pre- or mid-menstruation pain in the pelvis, lower back, or upper legs that persists for 48–72 hours. 7 Menstrual distress has also been reported to manifest with such symptoms as lower back pain, abdominal distension, indigestion, headache, nausea, fatigue, diarrhea, lethargy, sensitivity, breast tenderness, fluid accumulation, autonomic nervous symptoms, attention degradation, depression, and emotional distress and disturbance. 6,8 Menstrual cramps and distress can lead to a variety of health problems that can affect daily activities, such as housework, job or work time, and academic performance. 5,6,8 –10
In particular, menstrual cramps and menstrual distress in undergraduate students often result in an increased use of medical services when school is in session; effective measures are therefore needed to alleviate these problems and avoid consequent socioeconomic problems due to decreased productivity and class deficiency. 8 –10 Most clients with menstrual cramps and menstrual distress either endure the symptoms or are administered medications such as analgesics. However, analgesics are not a long-term solution because of risks for decreased effectiveness and increasing dependency. 1,2,4 Accordingly, alternatives to these conventional therapies, such as aromatherapy, acupressure, acupuncture, massage, topical heat, transcutaneous electrical nerve stimulation, behavioral interventions, yoga, and herbal and dietary therapies, are increasingly attracting attention. 6,7,11,12
Previous studies have suggested that, of these alternatives, yoga may have beneficial effects on physical and mental health problems through downregulation of the hypothalamic–pituitary–adrenal axis and the sympathetic nervous system, which may also be useful for managing primary dysmenorrhea. 7,12,13 Yoga practices generally consist of pose, exercise, breathing, relaxation, and meditation. Yoga programs that have been adjusted to clients with primary dysmenorrhea include three yoga poses, surya namaskara, and yoga nidra. 7,11,12 Hence, the authors reorganized an integrated yoga program with yoga practices applied in previous studies because of the presumption that the integrated yoga program may aid in simultaneously alleviating physical, mental, and emotional problems of dysmenorrhea according to medical pain theory of a spiral processing of pain, tension, fear, and pain sequentially. 7 The integrated yoga program of the present study included surya namaskara, three yoga poses, and yoga nidra sequentially.
Yoga is now recommended as a noninvasive method and easily accessed intervention for pain relief that is safe and cost-effective with minimal or no side effects. 11,12 However, relatively few studies have examined the benefits of yoga for relief of menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea. 7,11 –13 Moreover, previous studies have significant limitations, with issues such as potential bias due to lack of blinding, randomization in client recruitment process, ultrasound confirmation of primary dysmenorrhea or pelvic diseases, and proposed underlying mechanisms. 7,11 –13 Follow-up studies are needed to improve understanding of the effectiveness of yoga via rigorous methodologic application of a variety of yoga programs. Therefore, considering the limitations presented in previous studies, this study aimed to assess the effects of an integrated yoga program for management of menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea.
Materials and Methods
Participants
Study participants were recruited through the Internet homepage of our nursing department. The volunteer participants were all students at a nursing college near the Daejeon metropolitan area in the Republic of Korea. The study procedures were approved by the institutional review board of Kangwon National University (KWNUIRB-2015-02-002-001). The selection criteria were as follows: (1) age 18–25 years, (2) menstrual cramp pain score above 6 points on the 10-point Visual Analogue Scale for Pain (VASP), (3) menstrual cycle duration between 20 and 40 days, and (4) body–mass index between 18 and 25 kg/m2. Volunteers meeting the following criteria were excluded: (1) diagnosis of pelvic or gynecologic diseases or secondary dysmenorrhea, (2) surgery related to pelvic or gynecologic diseases, (3) use of contraceptives, and (4) experience with yoga exercises.
All participants received detailed information on the purpose and usefulness of this study and were given a written consent form. After the participants signed the form, an obstetrics and gynecology specialist at a women's hospital near Daejeon performed pelvic ultrasound examinations to screen for pelvic or gynecologic diseases, and the VASP and short-Form Menstrual Distress Questionnaires (SF-MDQs) were distributed to all participants. A total of 40 respondents aged 20 years or older were screened for cycles lasting 21–40 days, with actual menstrual periods lasting 3–7 days; 40 volunteers entered the initial phase of the study. Sample size was estimated by using G power 3.1 14 on the basis of data from a previous study. 15 Participants were randomly assigned to yoga exercise (n = 20) or control (n = 20) groups by a random permuted block design using a random-number table through the Excel random-numbers function (Microsoft Corp., Redmond, WA). Forty participants completed the entire study, 20 each in the yoga exercise and control groups. Demographic and menstrual information, VASP score, menstrual pain duration, and SF-MDQ responses were measured before initiation of the 12-week yoga program. VASP score, menstrual pain duration, and SF-MDQ responses were also measured after program completion.
Intervention
This study was a single-blind, randomized controlled trial. On the basis of a literature review of yoga for managing primary dysmenorrhea, an integrated yoga program consisting of three parts (surya namaskara, three yoga poses, and yoga nidra) was used. These parts were chosen because of the availability of scientific studies on these specific types of yoga. 7,12,16 Surya namaskara, or “sun salutations,” consists of 12 postures and breathing exercises. The three yoga poses were cobra, cat, and fish. Yoga nidra, which means “psychic sleep,” is a specific yogic relaxation and meditation practice. 16 The integrated yoga program in this study (Fig. 1) was conducted for about 1 hour once a week for 12 weeks under the guidance and supervision of a yoga specialist certificated by the Korea Yoga Association. The integrated yoga program was performed at the Konyang University Continuing Education Center at a nursing college. The participants first performed 10 cycles of surya namaskara for 15 minutes and then performed shavasana for 5 minutes of relaxation. Next, five cycles of cat, cobra, and fish yoga poses were performed for 10 minutes. Finally, the participants performed yoga nidra for 30 minutes. Yoga nidra was performed in shavasana. Yoga nidra has several steps, including resolve; rotation of consciou.m.sness; awareness of breath, feeling, and sensation; and visualization. 12,16 It ends with resolve. 12,16 The control group did not practice this yoga program. For yoga quality control, the participants were motivated to continuously attend the yoga program; the yoga instructor confirmed and corrected yoga postures and movements of participants in every yoga class. Before starting yoga, if possible, information that proposed limits on other exercises except yoga during the study period was given to the experimental group, but there was no special restriction on exercises or daily activities except yoga to the control group. The yoga group was asked to strictly abstain from any other types of yogic practices and to avoid direct contact with the control group. Bread and beverages were offered to all participants after practicing the yoga program, which started at 5 p.m. every Friday.
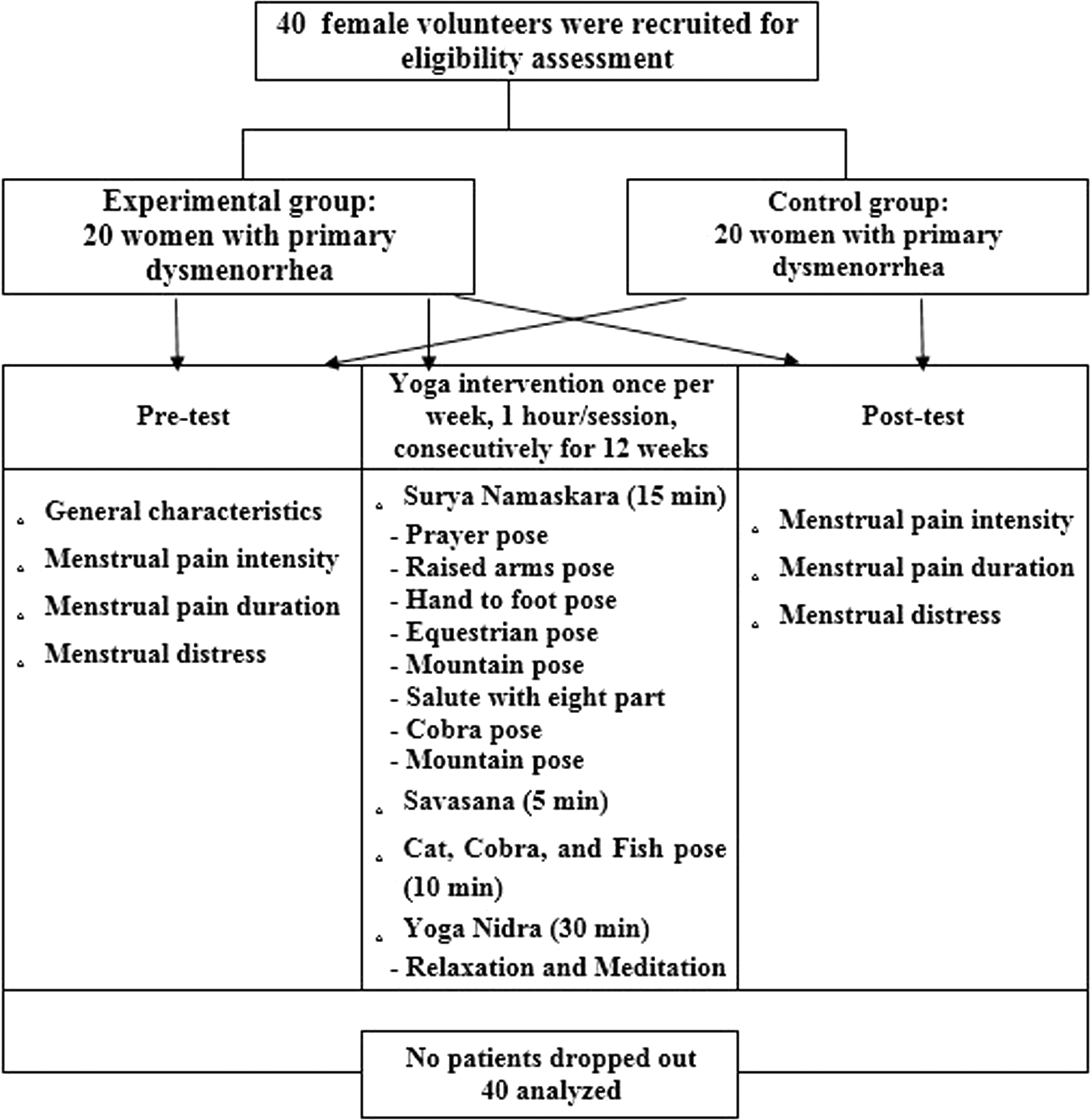
Flowchart of the study.
Outcome measures
Measurement of menstrual pain intensity
Pain intensity measured by using a 10-point VASP in which a line was calibrated from 0 to 10 with 0 representing “no pain at all” and 10 representing “worst pain possible.” Participants indicated their perceived pain levels by pointing to the appropriate value on a 10-cm horizontal ruler. 6 The intensity of pain was rated to the first decimal place in centimeters. Higher scores represented higher menstrual pain intensity.
Measurement of menstrual pain duration
Duration of pain was measured by using descriptive data obtained from study participants.
Measurement of menstrual distress
Menstrual distress was measured by using a modified SF-MDQ to screen and assess both psychological and physical aspects associated with premenstrual and menstrual distress. 5,6,11,17,* This tool consisted of 27 items scored using a 5-point Likert scale, ranging from never (1) to very often (5), and measured sources of menstrual distress based on subscales such as psychological and physical distress. Higher scores indicated higher perceived levels of menstrual distress. Cronbach α for the internal consistency reliability of the SF-MDQ was 0.83 in an earlier study and 0.94 in this study.
Statistical analysis
Statistical analyses were conducted by using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY). Data are presented as mean ± standard deviation or as numbers and percentages. Menstrual distress was verified to be normally distributed according to the Kolmogorov-Smirnov and Shapiro-Wilk normality test except for menstrual pain intensity and menstrual pain duration. Therefore, for the menstrual pain intensity and menstrual pain duration, a chi-square independence test was used. The prescores of menstrual pain intensity and menstrual pain duration were skewed in specific values; all of the adjusted standardized residual was below 2, and there was no difference in the distribution between the two groups. There was no significant difference in menstrual pain intensity and menstrual pain duration between the two groups. Therefore, normality was in violation; however, considering the consistency of the statistical approach, normality was assumed. A t-test or chi-square test was used to test for homogeneity of prescored demographic and menstrual characteristics between the experimental and control groups (Table 1). Multivariate analysis of variance tested for the homogeneity of prescored menstrual characteristics. Because prescored menstural pain intensity had no homogeneity between the experimental and control groups (Table 2), propensity score matching was processed to create homogeneity between the groups. The propensity score matching process was as follows: Group was considered a dependent variable and menstural pain intensity as a covariate; logit probabability was presumed through logistic regression analysis. On the basis of the logit probability, the probability values were drawn out that may be involved whether in the experimental group or not. According to logit probability values of both groups, excluding two participants who had 0.84409 logit probability in the experimental group and 0.24578 logit probability in the control group, the total sample size of 36 was confirmed, with 18 in each group.
Values are expressed as mean ± standard deviation or number (percentage).
Values expressed with a plus/minus sign are the mean ± standard deviation.
Significant differences between groups were determined using independent two-sample t-tests. Significant differences within groups were determined by using paired-sample t-tests. Treatment effects were reported as adjusted group differences, including their respective 95% confidence intervals (CIs) and p-values. To ensure comparability between the different outcomes measures, standardized effect sizes were calcultaed by dividing the estimated group difference by the mean standard deviation at baseline. p-Values less than 0.05 were considered to indicate statistically significant differences.
Results
Participant characteristics
As shown in Table 1, there were no significant differences in demographic and menstrual characteristics between the yoga and control groups.
Menstrual pain intensity
As shown in Table 3, at week 12, the yoga group had significantly decreased menstrual pain intensity compared with the control group (between-group difference, −0.94; 95% CI, −1.47 to −0.42; p = 0.001). From baseline to week 12, the mean postintervention menstrual pain intensity level in the yoga group decreased significantly compared with the preintervention level (p < 0.0001).
The p-values of differences between groups were calculated by independent two-sample t-test and paired-sample t-test; mean group difference and standardized effect size with 95% CIs. Values expressed with a plus/minus sign are the mean ± standard deviation.
Significantly different from baseline.
p < 0.05.
p < 0.0001.
CI, confidence interval.
Menstrual pain duration
As shown in Table 3, at week 12, there were no significant differences between the yoga and control groups (p > 0.05). The mean postintervention menstrual pain duration level in the yoga group decreased significantly compared with the preintervention level (p < 0.05).
Menstrual distress
As shown in Table 3, at week 12, the yoga group had significantly decreased menstrual distress score compared with the control group (between-group difference, −1.13; 95% CI, −1.43 to −0.82; p<0.0001). The mean postintervention menstrual distress score in the yoga group decreased significantly compared with the preintervention score (p < 0.0001).
Safety
No participants reported treatment side effects, and none withdrew from the study before completing the post-test assessment.
Discussion
In this trial, the yoga group had significantly decreased menstrual pain intensity levels after a 12-week integrated yoga program compared with the control group. Additionally, participants in the yoga group had significantly decreased pain intensity levels compared with before starting yoga practice, while pain intensity levels did not differ significantly in the control group. These findings are similar to those of a previous study, which suggested that menstrual pain intensity levels decreased significantly from baseline after 1 and 2 months. 7 A previous study assessed the effects of an 8-week intervention comprising cobra, cat, and fish poses on the health of university students with primary dysmenorrhea. The results of this study indicate that yoga interventions might be effective in decreasing stress, promoting relaxation, and increasing circulation based on the gate control theory, which describes regulation of pain centers located in the spinal cord that reduce pain and secrete natural painkillers in the body. 7 Other studies have also suggested that yoga breathing exercises can increase relaxation and reduce tension; awareness of breathing can also lead to relaxation and pain management through calmer and slower respiration. 7,13
Like previous studies, the present study also supports the paradigm that yoga exercise can have beneficial effects on menstrual pain in nursing students with primary dysmenorrhea. In addition to the effects of yoga practice, these findings may be influenced by the potential positive effects of community or social interaction, which may be a confounding factor. Some of the observed effects may be due to social interaction before, during, or after class in the treatment group; the control group did not participate in group activity. This effect may be particularly relevant because the participants met with the same group in yoga classes each week and had the same instructor. Menstrual pain intensity in this study did not differ in the control group after 12 weeks, possibly because the control group was influenced by a variety of factors, such as fatigue, diet, health status, lifestyle, and other personal issues. At week 12, menstrual pain duration did not significantly differ between the yoga and control groups in this and another study. 7 However, the mean postintervention menstrual pain duration level in the yoga group decreased significantly compared with before the intervention. This finding is similar to that of a previous study. 7 Further investigation is needed to confirm the efficacy of yoga for management of menstrual pain duration because of the small number of studies.
As shown in Table 3, compared with preintervention scores, menstrual distress score decreased significantly after participants completed the 12-week yoga program. In addition, menstrual distress scores decreased significantly during the 12-week period in the yoga exercise group but not in the control group. These findings are similar to those of an earlier study, which reported significantly decreased menstrual distress scores after an 8-week yoga practice period. 11 The researchers assessed the effects of a yoga program on menstrual distress in young college students with and without dysmenorrhea. 11 In that study, the yoga program comprised a warm-up period and static yoga postures, such as tortoise, cobra, reverse table, bridge, and cobbler's poses, with regular breathing and relaxation. 11 The authors also suggested that yoga might have positive psychological and physical effects because of its similarity to exercise and that yoga might be considered as part of an exercise program to reduce stress, improve flexibility, and strengthen muscles. 11 Like the previous study, the present study supports the paradigm that yoga exercise can reduce psychological and physical problems in nursing students with primary dysmenorrhea.
Previous studies found that the integrated yoga program used in the current study had beneficial effects on menstrual pain or menstrual distress in college students with primary dysmenorrhea. In a traditional model, surya namaskara is thought to induce pain relief and nervous/endocrine balance. 13 Previous research has also suggested that “the cobra pose yoga improves spinal flexibility and strengthens the muscles in back, cat pose yoga initiates movement from center and coordinates movement and breath, and the fish pose relieves stiffness of the neck and shoulder muscles and improves flexibility of spine.” 7 The deep relaxation techniques of yoga nidra lead to a relaxation response. 12,18 This response reportedly results in decreased sympathetic nervous system activity and oxygen consumption, reduced oxidative stress, and increased pain relief. 11,12 In previous studies, researchers stressed that, even with brief program exposure, yoga postures and breathing exercises were effective methods for controlling psychological and physical problems in participants with primary dysmenorrhea. 7,11
Similar to previous studies, the present study suggests that the integrated yoga program can also help to reduce menstrual pain and menstrual distress. Therefore, the 12-week yoga intervention in this study was identified as significantly and clinically meaningfully decreasing menstrual pain intensity and menstrual distress levels in primary dysmenorrhea clients. Through these findings, the potential mechanism for effectiveness in primary dysmenorrhea can support the downregulation theory of hypothalamus pituitary adrenal axis and sympathetic nervous system by practicing combined exercise and relaxation of yoga with deep breathing of yoga sequentially. However, limited data are available on the effect of the integrated yoga program studied on menstrual distress scores in participants with primary dysmenorrhea. Moreover, scientific evidence of the integrated yoga program is developed to support the effects of this yoga intervention in primary dysmenorrhea. Unlike other yoga programs, this program is integrated and cyclic, comprising a variety of poses, exercise, breathing, relaxation, and meditation.
In addition, these findings suggest that biochemical parameters, such as levels of homocysteine, nitric oxide, or other hormones leading to menstrual pain, must be included in a follow-up study because of correlation of the participants' reports with laboratory data. 11,12 Because these findings were also obtained from nursing school students, further global studies considering a variety of sociocultural and economic context to confirm these findings and how they apply other women of reproductive age are needed. Furthermore, through rigorous methods, meta-analysis of studies on the effects of the integrated yoga program will enable review and assessment of the effect size of accumulated research outcomes. 7,11 –13,19
This study has several strengths. First, participants were randomly allocated. Second, confirmation of primary dysmenorrhea or pelvic diseases was based on ultrasound scans rather than participant reports. Third, there were no treatment side effects or withdrawal events. Finally, the yoga group was strictly blinded about the yoga program.
The present study also has some limitations. First, it was not possible to perform this study under double-blind conditions. The control group did not receive any treatment during the study period, which may have influenced the results. In addition, the small sample from a single college prevents generalization of the study results. This study also did not measure biochemical parameters. Finally, the participants were not on a strict and uniform diet and lifestyle.
Conclusions
Despite these limitations, these findings suggest that an integrated yoga program, such as the one described in this study, can improve not only levels of menstrual pain intensity but also menstrual distress scores in nursing students with primary dysmenorrhea.
Footnotes
Acknowledgments
This study was supported by a 2104 research grant from Kangwon National University (award no. C 2001008-01-01).
Author Disclosure Statement
No competing financial interests exist.