
Abstract
Objectives:
This study aimed to identify the acupressure effect over time, compare the efficacy in different dosages, and identify feasibility issues with saliva sample collection and acupressure implementation in agitated nursing home residents with dementia.
Design:
Time serial design with eight dosage-combination groups.
Setting:
Three residential care homes (RCHs) in Hong Kong.
Participants:
Agitated RCH residents with dementia.
Interventions:
Acupressure was performed for 9 minutes altogether on five acupoints: Fengchi (GB 20), Baihui (GV 20), Shenmen (HT 7), Niguan (PC 6), and Yingtang (EX-HN 3). Two frequencies (once and twice a day) and four durations (1, 2, 3, and 4 weeks) formed eight dosage combinations.
Outcome measures:
The primary outcome was agitation, measured by the Cohen Mansfield Agitation Inventory. The secondary outcome was stress, measured by salivary cortisol.
Results:
Twenty-four participants from three RCHs completed the study. Acupressure was successfully completed for 88% of total sessions, and 79.17% of participants completed more than 80% of expected sessions. The effect of acupressure on agitation onset was seen immediately at week 1 (p < 0.001), resurged at week 4 (p = 0.001), and was sustained until week 6 (p < 0.001). The effect on stress began immediately to a mild extent at week 1 (p = 0.011) and peaked at week 4 (p = 0.010). Acupressure was observed to show the largest effect when it was performed twice a day (p = 0.026) for 2 weeks (p = 0.005). Valid saliva samples were collected for 53.33% of participants. Hyposalivation caused this unsatisfactory yield of valid saliva samples.
Conclusion:
Acupressure can be conducted on agitated RCH residents with dementia, but low yield of saliva samples related to participants' hyposalivation is a problem. Preliminary findings suggest that acupressure is effective in reducing both agitation and stress. Its onset of effect was immediate, and the effect was sustained until 6 weeks after the intervention. The optimal dosage appears to be a course of acupressure twice a day for 2 weeks.
Introduction
D
Acupressure is a nonpharmacologic intervention to apply pressure on specific acupoints on the body to treat a wide range of conditions or promote individual well-being. 15 The working mechanism of acupressure is not fully known, but it can be explained by many different theories. 16 Traditional Chinese Medicine (TCM) explains that acupressure stimulates the acupoints to enhance energy or qi flowing along the meridian, achieving therapeutic outcomes by improving the functions of body systems, or zangfu. 17 Biochemical studies explain that stimulation of the acupoints by pressure may cause complex neuro-hormonal responses; one of these may involve the hypothalamus-pituitary-adrenocortical (HPA) axis in counteracting the overproduction of cortisol to cause a relaxation response. 18 Similar manipulative therapies, such as massage and therapeutic touch, were shown to be useful in lowering patients' stress and cortisol after treatment. 19,20
Preliminary studies 21 –23 have shown that acupressure can reduce agitation in PWD. However, some issues that are important references for further studies were not discussed in the previous ones. 21 –23 Therefore, this pilot study aimed at resolving these issues by (1) identifying the effect over time, (2) comparing the efficacy of acupressure delivered in different dosages (i.e., frequency and duration of the intervention), and (3) identifying the feasibility issues in saliva sample collection and acupressure implementation on agitated PWD.
Materials and Methods
Design and participants
This study used a time serial design with multiple groups and was conducted in three RCHs in Hong Kong from May to July 2013. All residents in these three RCHs were screened for eligibility. All eligible residents were recruited. Inclusion criteria were age older than 65 years, documented status of dementia in the medical record, and having agitated behaviors for 1 month before the time of recruitment according to the criteria for agitation stated in the Cohen-Mansfield Agitation Inventory (CMAI) instruction manual. 24 Exclusion criteria were skin problems on acupoints and musculoskeletal problems. This study, including the intervention protocol and study procedures, was developed according to the Medical Research Council guideline 2008 for developing complex interventions. 25
Allocation to groups
To compare the effect among different dosages, participants were divided into eight groups according to different combinations of frequency and duration, as shown in Table 1. Frequency refers to the number of acupressure sessions performed in a day. Duration refers to the number of weeks during which acupressure was performed. Two frequencies and four durations were tested because they had been used in previous studies 21,22 or were suggested by the expert panel of TCM practitioners in this study.
2D1W, twice daily for 1 week; 2D2W, twice daily for 2 weeks; 2D3W, twice daily for 3 weeks; 2D4W, twice daily for 4 weeks; 1D1W, once daily for 1 week; 1D2W, once daily for 2 weeks; 1D3W, once daily for 3 weeks; 1D4W, once daily for 4 weeks.
Intervention
The intervention ingredients (e.g., selection of acupoints, procedural specifications) were determined by two methods: literature review and Delphi process. 26 In the literature review, articles discussing the theories possibly connecting the use of acupressure and agitation were identified through a systematic search of the literature. Evidence related to the use of acupressure on agitation in PWD was retrieved by using a systematic review. The literature review identified the existing evidence to justify the use of acupressure on agitation in PWD. This evidence was then summarized as a document for reference in the subsequent Delphi process. In the Delphi process, a panel of TCM experts specializing in acupuncture was consulted. Through this process, panel experts were first asked to suggest intervention ingredients and their rationales, with reference to the evidence summarized from the literature review and their own professional knowledge and experience. Then, intervention ingredients were identified through rounds of stepwise anonymous discussion. The rounds of discussion terminated when the necessary intervention ingredients were identified with complete agreement. Only ingredients with complete agreement from the expert panel were selected for the intervention protocol.
The intervention protocol involved five acupoints: Fengchi (GB 20), Baihui (GV 20), Shenmen (HT 7), Niguan (PC 6), and Yingtang (EX-HN 3). The acupoint locating techniques were based on two textbooks. 27,28 Acupressure application followed a light-strong-light pattern. Pressure was gradually increased until it reached the optimal level, was sustained for 3 minutes, decreased gradually, and ended with a kneading. The optimal pressure was defined as the level when de qi sensations (i.e., soreness, numbness, distention, heaviness) 29 were reported by the participants or when relevant behaviors (e.g., frowning, withdrawing) were observed by the interventionist. The level of pressure to achieve the de qi sensation was therefore different among individuals. Yintang (EX-HN 3) was first pressed for 3 minutes. Baihui (GV 20) and Fengchi (GB 20) were then pressed simultaneously for another 3 minutes. Finally, Neiguan (PC 6) and Shenmen (HT 7) were pressed simultaneously for the last 3 minutes. Each acupressure session lasted for 9 minutes.
To minimize the possible influence of the acupressure effect from the unavoidable human contact, the interventionists were instructed to minimize communications unrelated to the implementation of the acupressure during the intervention. The intervention period varied from 1 week to 4 weeks according to the group allocation, as shown in Figure 1.
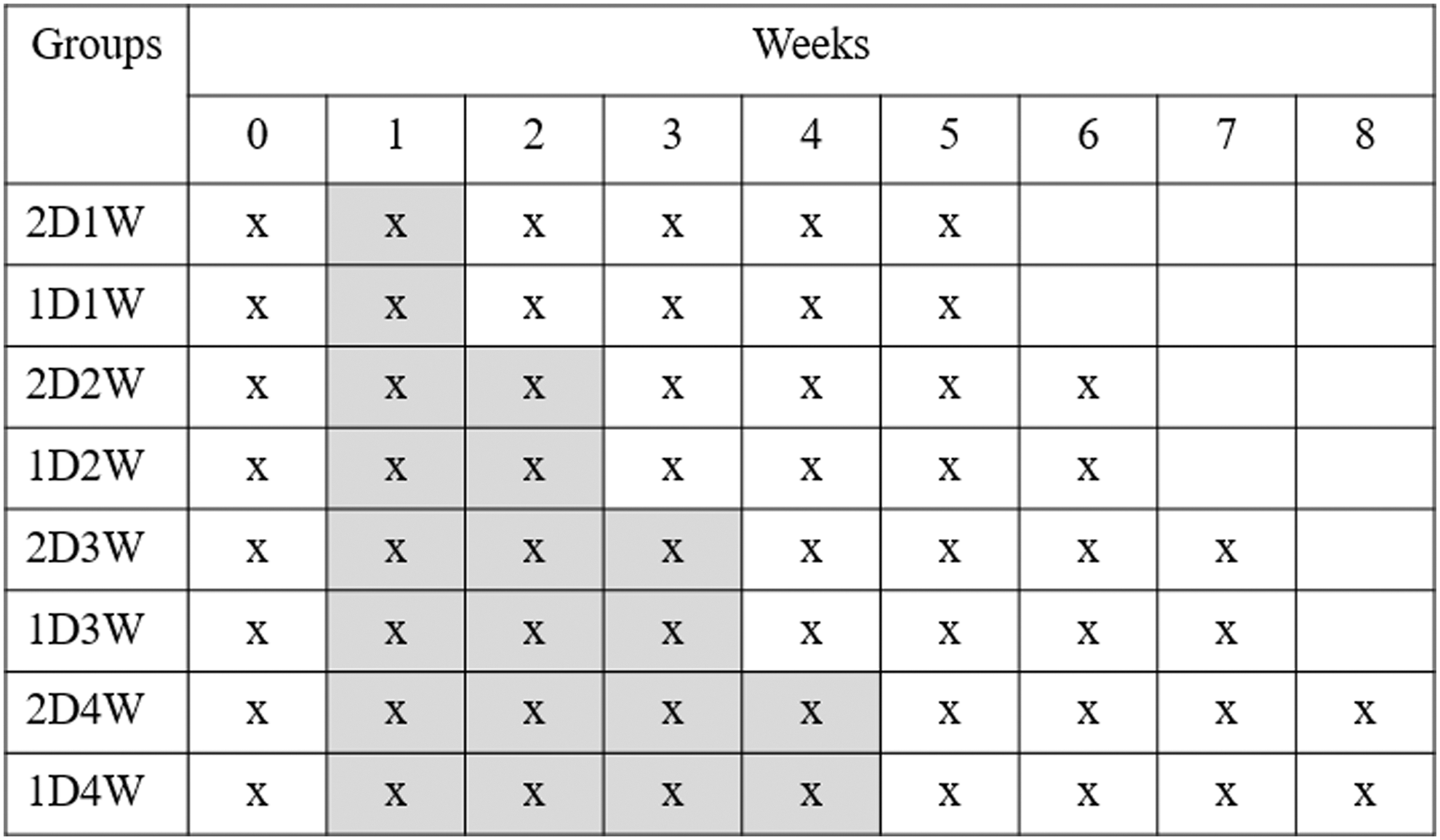
Intervention period and outcome measurement period in different groups. Shaded box, intervention period; boxes that contain an “x,” outcome measurement period. 1D1W, once daily for 1 week; 2D1W, twice daily for 1 week; 1D2W, once daily for 2 weeks; 2D2W, twice daily for 2 weeks; 1D3W, once daily for 3 weeks; 2D3W, twice daily for 3 weeks; 1D4W, once daily for 4 weeks; 2D4W, twice daily for 4 weeks.
Data collection and measurements
At the baseline, demographic data, such as age, sex, length of stay in the RCH, number of psychotropic drugs used, and number of comorbidities, were collected. Level of functioning using the modified Barthel Index (mBI), Chinese version, 30 and level of cognitive function using the Mini-Mental State Examination, Chinese version, 31 were collected.
The two outcomes were agitation and salivary cortisol (SC). They were measured weekly from the week before commencement of the intervention until 4 weeks after its completion. Because the duration of the intervention varied among groups, the periods of data collection in different groups also varied from 6 to 9 weeks according to the group allocation, as shown in Figure 1.
Agitation was the primary outcome and was measured by CMAI 32 weekly on the Sunday of the related week. The psychometric properties of the CMAI were good when the instrument was used on PWD in Hong Kong. The internal consistency was high (Cronbach α = 0.83). The content was valid (content validity index, 0.86) and the inter-rater reliability good (intraclass correlation coefficient, 0.82).
Stress was the secondary outcome and was measured by SC. Cortisol level is influenced by many other factors apart from stress, such as cortisol awakening response, eating, time of collection, and exercise. 33,34 To control for these confounding factors, all saliva samples were collected from 07:00 to 08:00. The collection time was also 1 hour after awakening and before oral care, breakfast, and all forms of activities. Saliva samples were collected twice weekly on the Saturday and Sunday of the related weeks. The two samples were averaged to represent the SC level of a participant in a particular week.
Saliva samples were collected using the Salimetrics Oral Swab. The swab was placed in the participant's oral cavity for 2–5 minutes. Collected saliva samples were kept in Salimetrics storage tubes and frozen at or below −20°C within 2 hours. During transportation, the samples were kept cold by ice-packed insulators. For analysis of the samples, the frozen swabs were thawed at room temperature and then centrifuged at a rate of 3000 RPM for 15 minutes to extract the saliva. The data collection, storage, and analysis procedures followed the manufacturer's guidelines. 35,36
This Salimetrics enzyme-linked immunosorbent assay kit is reliable because it requires 25 μL of saliva and has a sensitivity of less than 0.003 μg/dL and a calibration range of 0.012–3.000 μg/dL. Coefficient of variation is 6.41% across 12 runs; intra-assay variability coefficient of variation is 3.65%. 37 Free cortisol is the final product of the HPA axis, and saliva contains approximately 10% of the level of cortisol in plasma. 38 In a validation study of a healthy elderly cohort, the correlations of cortisol level in saliva and serum over a day were all significant (r = 0.54–0.96), 39 showing that salivary cortisol reflects serum cortisol well.
All data were collected by two trained research assistants, who attended an 8-hour training provided by the first author. The contents of training were prepared with reference to the original instruction manuals of the tools. During training, data collection was practiced on elderly volunteers. All data collectors had to demonstrate 100% inter-rater reliability with the first author in order to be considered competent. The data collectors and the CMAI informants (i.e., the formal caregivers in the RCH) were blinded to the participants' group label.
Statistical analysis
Statistical analysis was performed by using the IBM SPSS Statistics 20 for Windows software. 40 Continuous data are presented as mean with standard deviation (SD) or median with interquartile range and were compared between groups by using the Kruskal-Wallis test, Wilcoxon signed-ranks test, and Mann-Whitney U test. Nominal data are presented as frequency with percentage and were compared between groups by using a chi-square test. Because of the small sample size, nonparametric tests were used for comparison. Significance was defined as p < 0.05 in two-sided tests. Missing data were replaced by the last-observation-carried-forward principle. 41
Ethics
Proxy consent and assent from all recruited participants were obtained before they were formally admitted to the study. Written consent was also obtained from residents who were cognitively capable to give consent. After the consenting process, baseline data collection started. This study was approved by the Human Subjects Ethics Sub-Committee of the Hong Kong Polytechnic University (application number: HSEARS20120920001).
Results
Procedures
As shown in Figure 2, 403 residents were screened for eligibility in the three RCHs. There were 368 residents who did not meet the inclusion criteria. All excluded residents did not have a documented diagnosis of dementia or agitated behaviors as reported by the nursing home staffs. The remaining 35 residents were contacted one by one. The invitations of 10 residents were declined by the residents or their families. Finally, 25 participants were recruited, yielding a recruitment rate of 6.2%. These 25 eligible residents were nonrandomly allocated into groups. Twenty-four participants (96%) completed the intervention, and one (4%) dropped out and declined to give consent to provide data for this study, without giving any reasons.
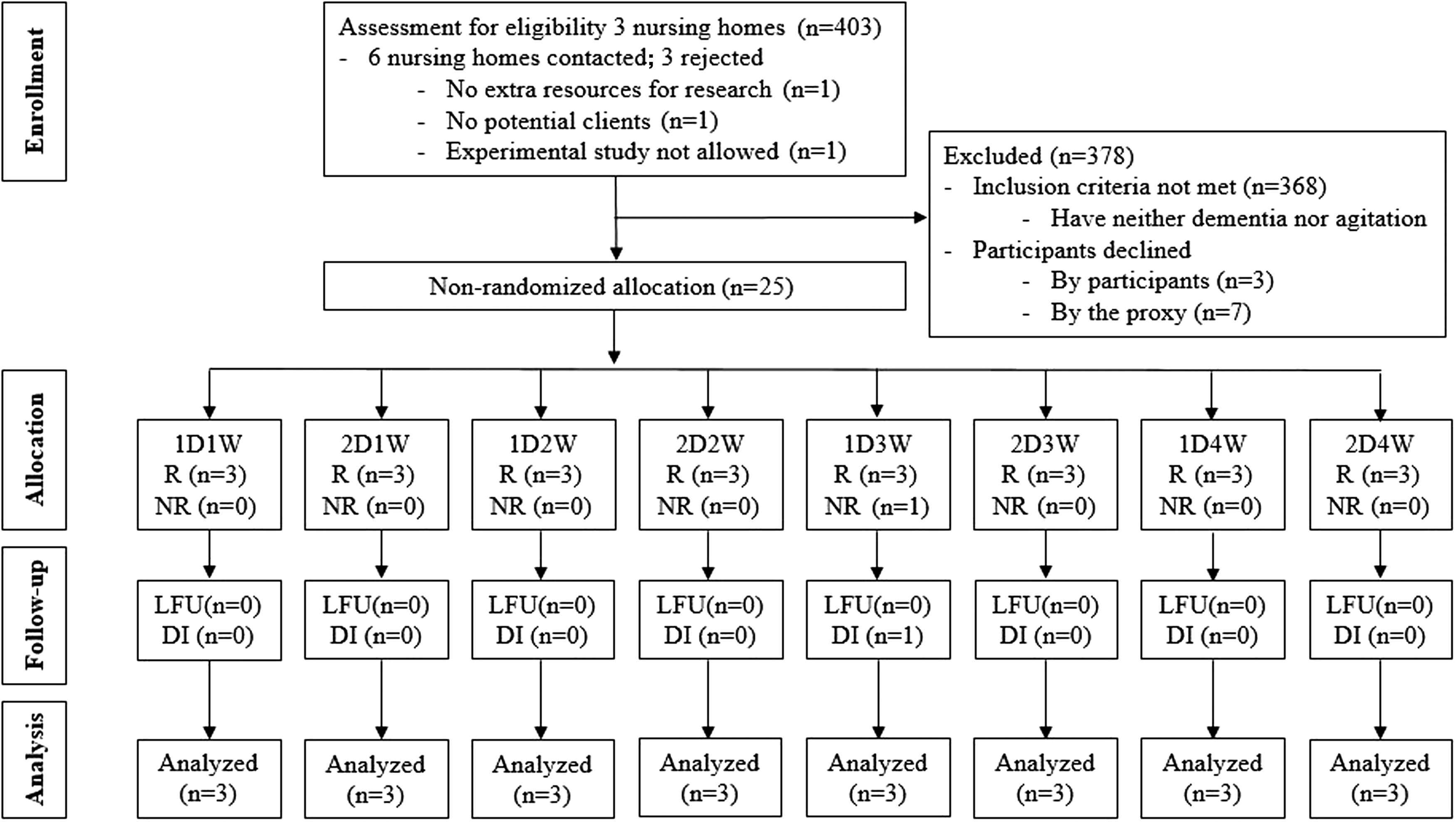
Participant flowchart. DI, discontinued intervention; LFU, lost to follow-up; NR, did not receive acupressure; R, received acupressure.
Participant characteristics
All participants were documented to have dementia without specification of the type on their medical records. As shown in Table 2, the mean age of the 24 participants was 82.83 years (SD, 6.94). There were 18 female (75%) and 6 male (25%) participants. The mean length of stay in the RCH was 33.08 months (SD, 20.94). The mean Mini-Mental State Examination score was 6.61 (SD, 6.32), the mean modified Barthel Index score was 20.83 (SD, 24.13), and the mean CMAI score was 43.67 at baseline (SD, 10.57). Most participants were taking one to three psychotropic drugs at baseline (75%).
Values expressed with a plus/minus sign are the mean ± standard deviation.
Only 23 participants completed the MMSE because 1 participant declined to do so.
RCH, residential care home; MMSE, Mini-Mental State Examination; mBI, modified Barthel index; CMAI, Cohen-Mansfield Agitation Inventory.
Effect over time
Primary outcome: CMAI
The pattern of changes in agitation for all groups over time is shown in Table 3. Agitation was reduced markedly in the first week after the commencement of acupressure. This effect diminished in weeks 2 and 3 and surged again in weeks 4, 5, and 6. The effect diminished gradually after week 6 and tailed off in week 8. The peak effect was observed in week 5. The reduction of median CMAIs was significant at weeks 1 (median difference, −9.0; p < 0.001), 4 (median difference, −9.0; p = 0.001), 5 (median difference, −9.5; p < 0.001), and 6 (median difference, −8.0; p < 0.001).
By Wilcoxon signed-rank test.
Statistically significant.
IQR, interquartile range.
Secondary outcome: SC
The pattern of changes in SC level of all groups over time is shown in Table 4. SC level was slightly reduced in the first week of acupressure. It was progressively reduced in weeks 2 and 3, reached a trough in week 4, and resurged markedly in weeks 5–7. It decreased again sharply in week 8. Reductions in median SC level were observed at most of the time points except weeks 5 and 7. The reduction in median SC level was significant in weeks 1 (median difference, −0.08 μg/dL; p = 0.011) and 4 (median difference, −0.30 μg/dL; p = 0.010).
By Wilcoxon signed-rank test.
Statistically significant.
SC, salivary cortisol.
Efficacy of the acupressure delivered in different dosages
The efficacy of the acupressure in different dosages was compared among groups by factors (i.e., duration and frequency) at the time point at which peak effect occured. Peak effect was observed for agitation in week 5 and for SC in week 4.
Comparison among various dosages for primary outcome: CMAI
In week 5, changes in CMAI compared with the baseline were significantly different in the 1-week group (median difference, −11.5; p = 0.046) and 2-week group (median difference, −14; p = 0.026), as shown in Table 5 and more significant (i.e., a lower p-value) in the 2-week group than the 1-week group. There were no significant differences among other groups (i.e., the 3- and 4-week groups).
By Wilcoxon signed-rank test.
Statistically significant.
In week 5, changes in CMAI compared with baseline were significantly different in the once-a-day group (median difference, −12.00; p = 0.019) and twice-a-day group (median difference, −9.00; p = 0.005), as shown in Table 6, but the reduction was more significant (i.e., a lower p-value) in the twice-per-day than the once-per-day group.
By Wilcoxon signed-rank test.
Statistically significant.
Comparison among various dosages for secondary outcome: SC
In week 4, there were no significant effect differences in SC level from the baseline in any groups on the basis of duration. However, in week 4, SC level significantly differed from baseline in the twice-per-day group (median difference, −0.37 μg/dL; p = 0.015), as shown in Table 7.
By Wilcoxon signed-rank test.
Statistically significant.
Feasibility issues
Valid saliva sample return rate
For the saliva sample collection, of the 24 participants with twice-weekly repeated measurements, 360 salivary samples were expected to have been collected. As shown in Figure 3, 161 samples were excluded because participants declined to undergo saliva sampling or returned saliva-collecting swabs containing no or inadequate saliva volume. After the enzyme-linked immunosorbent assay, seven samples were discarded because the salivary cortisol level exceeded the calibrated range because of possible contamination (n = 5) and duplicate labeling (n = 2). Finally, 192 saliva samples were used for data analysis, with a valid return rate of 53.33%.
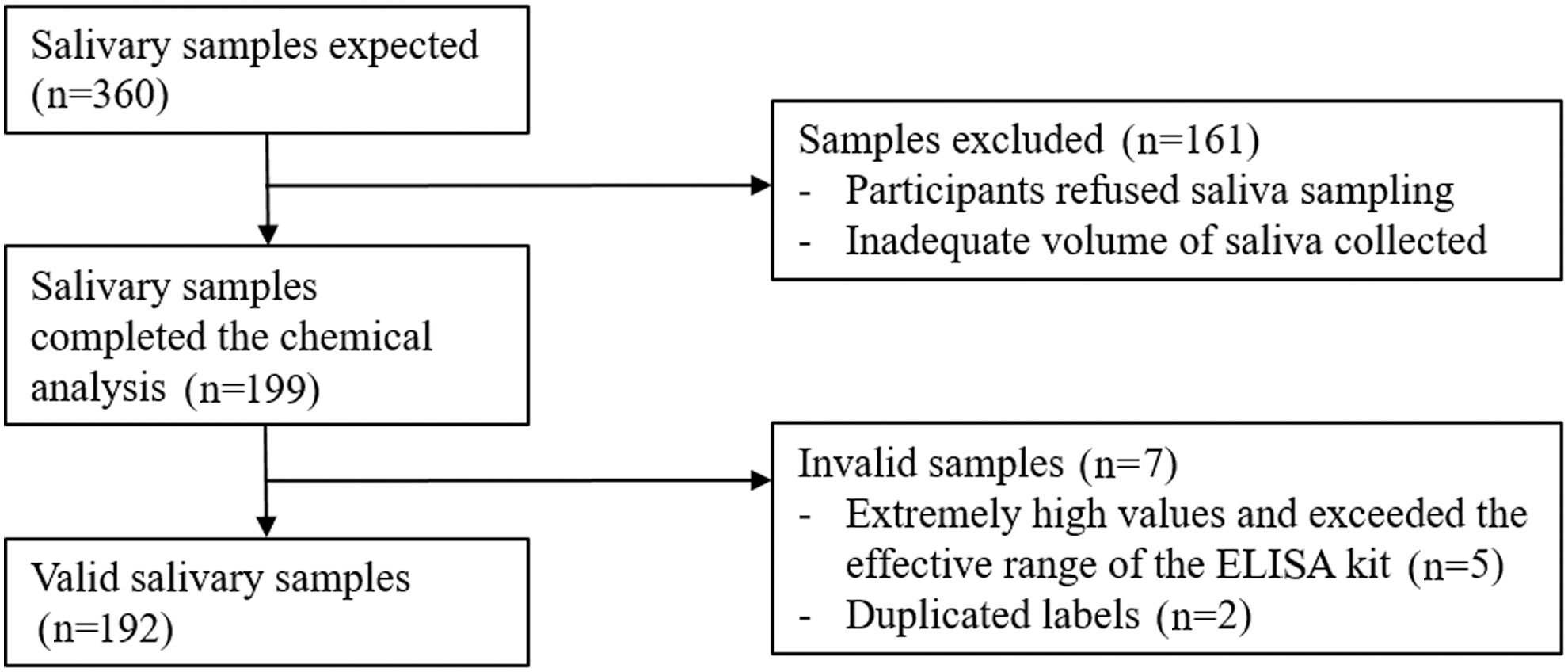
Flowchart of valid salivary samples collected. ELISA, enzyme-linked immunosorbent assay.
As shown in Figure 4, some participants yielded very few saliva samples because of their persistent dry mouth (n = 4) or consistent refusal (n = 2). They yielded less than 10% of the expected saliva samples, and no saliva could be collected at baseline. Their samples were excluded from data analysis. Finally, 184 salivary samples from 18 participants were used for data analysis.

Flowchart of participants who gave valid salivary sample selection.
Adherence to the intervention protocol
In this study, 450 sessions of acupressure were expected to be provided to the 24 participants in eight groups. Fifty-four of the sessions were not conducted because participants were not available when the interventionists visited them (e.g., medical appointment or family gathering), or the participants or their families declined because of episodic bad mood, transient illnesses, or hospitalization of participants. A total of 396 sessions were completed, with an adherence-by-session rate of 88%.
Participants were considered to have adhered to the intervention only if they had completed 80% or more of the expected number of sessions; 19 of 24 participants adhered, with an adherence-by-participant rate of 79.17%.
Discussion
The findings from the pilot study showed a promising effect of acupressure in terms of agitation and SC reduction, although the value of the findings was restricted by some limitations. These findings support the potential value of using acupressure to manage agitation in PWD and provide references for future clinical trials and similar studies in terms of (1) sample size estimation and recruitment strategies, (2) optimal acupressure dosage to be used, (3) outcome measurement intervals, and (4) data collection and intervention implementation strategies.
Sample size estimation and recruitment strategies
The effect size by Cohen d in this study ranged from 0.58 to 1.03. This was lower than the value in a previous study, in which the Cohen d was 1.71. 21 This could be because the baseline agitation level was lower in this study (mean CMAI, 43.67) than in Yang and colleagues' study (mean CMAI, 79.3). 21 Attrition in this study was 4%, lower than the 10% in another previous study. 22 This could be because the duration of the intervention in many groups was shorter than in Lin and colleagues' study. 22 The recruitment rate, not reported in the two earlier studies, 21,22 was 6.2% in the current study.
Given the low recruitment rate in this study and considering cost-effectiveness, it is suggested that only large RCHs be invited to participate. Measures should also be taken to ensure correct screening by the RCH person-in-charge in order to ensure that all eligible people are invited. Such measures include a face-to-face meeting to explain the screening process, written screening procedure instructions, and meetings to discuss uncertain eligibility.
Estimation of optimal acupressure dosage
This study found that relatively shorter duration (i.e., 1 or 2 weeks) and greater frequency of the intervention (i.e., twice a day) showed larger effects. This dose was different from the acupressure protocol for managing agitation in PWD reported earlier; those studies administered acupressure once daily for 4 weeks 21 or twice daily for 4 weeks. 22 However, the previous studies did not compare effect sizes of different dosages. Therefore, the current authors recommend acupressure twice a day for 2 weeks for optimal results.
Outcome measurement intervals
For the primary outcome (i.e., agitation), peak effect was observed at week 5 and tailed off at week 8. Significant effect of acupressure for managing agitation in PWD was also observed in similar protocols 21,22 in previous studies at week 5. It is justified to believe that the peak agitation-reducing effect appears at week 5. However, previous studies did not report the delayed effect. To capture the effect, it is suggested that outcomes and delayed effect be measured at weeks 5 and 8 after commencement of the intervention, respectively.
Data collection and intervention implementation strategies
In this study, saliva could not be extracted from many collected samples because of dry mouth in the elderly RCH residents. Hydration is the most important factor influencing saliva production. 42 Ensuring that study participants are well hydrated may play an important role in successful saliva collection. The participant adherence rate was satisfactory (79.17%). This may show that this acupressure protocol is well tolerated by participants and that no modification against acceptability is needed.
Strengths and limitations
Previous studies of acupressure for agitation in PWD rarely discussed recruitment, saliva sample collection, implementation of acupressure protocol, dosage justification, and effect duration. This study enriches understanding of these issues. It also provides promising results of acupressure on agitation reduction, consistent with the findings of previous similar studies, 21 –23 and concurrently on cortisol reduction, which has been rarely reported. Nevertheless, the findings of this study are limited by its small sample size (24 participants), unsatisfactory collection of valid saliva samples (53.33%), and flaws in the study design (e.g., too few participants in each group, no random group allocation, no control groups for comparing the possible effect of usual care and human contact). Further studies should aim to resolve these methodologic flaws in order to improve understanding of the effects of acupressure. Further studies should also examine whether acupressure reduces agitation in PWD through mediations of the HPA axis.
Conclusion
This study showed that acupressure produced the largest effect when performed twice daily for 2 weeks. The effect of acupressure on agitation had an immediate onset in week 1, resurged in week 4, and was sustained until week 6. The effect of acupressure on cortisol was mild in week 1 and peaked only in week 4. Delivering acupressure to agitated PWD was feasible, with a fairly good adherence rate. Saliva sample collection was feasible, but the hyposalivation of PWD should be resolved in order to yield more valid samples. This study reported recruitment rate, attrition rate, and effect size, which may be useful for further similar studies. It had some methodologic flaws (i.e., small sample size and number of participants per group) and unsatisfactory collection of valid saliva samples. Yet this study found that acupressure reduces both agitation and SC levels. Further studies should be done to resolve the saliva sample collection difficulties and examine the possible role of the HPA axis in explaining how acupressure reduces agitation.
Footnotes
Acknowledgments
This study was funded by the Sigma Theta Tau International Nursing Honor Society under the Small Grant category in 2012. The sponsor had no involvement in the study.
Author Disclosure Statement
No competing financial interests exist.