
Abstract
Objectives:
To evaluate the effects of craniosacral therapy on disability, pain intensity, quality of life, and mobility in patients with low back pain.
Design:
A single-blinded randomized controlled trial.
Patients:
Sixty-four patients with chronic nonspecific low back pain (mean age ± SD, 50 ± 12 years; 66% female) who were referred for physical therapy at a clinical unit of the Health Science School of the University of Almeria (Spain).
Interventions:
Participants were randomly assigned to an experimental group (10 sessions of craniosacral therapy) or a control group (10 sessions of classic massage).
Outcome measures:
Disability (Roland Morris Disability Questionnaire [RMQ, primary outcome] and Oswestry Disability Index), pain intensity (10-point numeric pain rating scale), kinesiophobia (Tampa Scale of Kinesiophobia), isometric endurance of trunk flexor muscles (McQuade test), lumbar mobility in flexion, hemoglobin oxygen saturation, systolic blood pressure, diastolic blood pressure, hemodynamic measures (cardiac index), and biochemical estimation of interstitial fluid. These outcomes were registered at baseline, after treatment, and 1-month follow-up.
Results:
No statistically significant differences were seen between groups for the main outcome of the study, the RMQ (p = 0.060). However, patients receiving craniosacral therapy experienced greater improvement in pain intensity (p ≤ 0.008), hemoglobin oxygen saturation (p ≤ 0.028), and systolic blood pressure (p ≤ 0.029) at immediate- and medium-term and serum potassium (p = 0.023) level and magnesium (p = 0.012) at short-term than those receiving classic massage.
Conclusions:
Ten sessions of craniosacral therapy resulted in a statistically greater improvement in pain intensity, hemoglobin oxygen saturation, systolic blood pressure, serum potassium, and magnesium level than did 10 sessions of classic massage in patients with low back pain.
Introduction
L
Craniosacral therapy is an alternative and complementary therapy based on the theory that restricted movement at the cranial sutures of the skull negatively affect rhythmic impulses conveyed through the cerebral spinal fluid from the cranium to the sacrum. 5,6 Restriction within the craniosacral system can affect its components: the brain, spinal cord, and protective membranes. The brain is said to produce involuntary, rhythmic movements within the skull. This movement involves dilation and contraction of the ventricles of the brain, which produce the circulation of the cerebral spinal fluid. 5,6 The theory states that this fluctuation mechanism causes reciprocal tension within the membranes, transmitting motion to the cranial bones and the sacrum. 7
Craniosacral therapy and cranial osteopathic manual therapy originate from the observations made by William G. Sutherland, who said that the bones of the human skeleton have mobility. These techniques are based mainly on the study of anatomic and physiologic mechanisms in the skull and their relation to the body as a whole, which includes a system of diagnostic and therapeutic techniques aimed at treatment and prevention of diseases. These techniques are based on the so-called primary respiratory movement, which is manifested in the mobility of the cranial bones, sacrum, dura, central nervous system, and cerebrospinal fluid. The main difference between the two therapies is that cranial osteopathy, in addition to a phase that works in the direction of the lesion (called the functional phase), also uses a phase that worsens the injury, which is called structural phase. 5 –7
Craniosacral therapy has been used in the treatment of fibromyalgia, 8,9 temporomandibular disorders, 10 migraine, 11 lateral epicondilitis, 12 individuals with dementia, 13 lower urinary tract signs and symptoms in multiple sclerosis, 14 several types of disabilities, 15 and disabilities in children. 16 A preliminary report on the utility of craniosacral and trigger-point therapy in LBP claimed that further research with randomized samples is required to determine the mechanism by which craniosacral therapy may effectively reduce the intensity and frequency of pain in LBP. 17
The purpose of the current randomized clinical trial was to analyze the effectiveness of craniosacral therapy on disability, pain intensity, kinesiophobia, isometric endurance of trunk flexor muscles, mobility, oxygen saturation, blood pressure, cardiac index, and biochemical estimation of interstitial fluid in individuals with chronic LBP.
Materials and Methods
Participants
A single-blind randomized trial was conducted. Patients with chronic LBP who were referred for physical therapy to a clinical unit of the Health Science School of the University of Almeria in Spain were recruited for this study. Chronic nonspecific LBP was defined as tension, soreness, and/or stiffness below the costal margin persisting for at least 3 months, for which a specific disease or clear pathological cause of the pain could not be identified. To be eligible, patients had to meet the following inclusion criteria: (1) LBP for at least 3 months, (2) age 18–65 years, (3) a score of 4 or greater on the Roland Morris Disability Questionnaire (RMQ), and (4) not currently receiving physical therapy. Exclusion criteria were (1) presence of lumbar stenosis, (2) diagnosis of spondylolisthesis, (3) diagnosis of fibromyalgia, (4) treatment with corticosteroid or oral medication within the past 2 weeks, (5) a history of spinal surgery, and (6) disease of the central or peripheral nervous system.
The protocol was approved by the local human research committee of the University of Almeria (06/13/2015). It was conducted by following the Declaration of Helsinki, and all participants signed an informed consent form before inclusion in the study.
Outcome measures
Patients provided demographic and clinical information and also completed several self-report measures. The main variable used in this study was the RMQ, which assesses disability due to LBP. It consists of 24 items reflecting current limitations in different activities of daily living attributed to LBP. 18 –20 The total score ranges from 0 (no disability) to 24 (maximum possible disability). The Spanish version exhibits good test–retest reliability (intraclass correlation coefficient [ICC], 0.87) and good internal consistency (Cronbach α, 0.84–0.91). 21 Bombardier et al. 22 found that a change in 2–3 points represents a minimum clinically important difference (MCID), and Jordan et al. 23 concluded that MCID is shown if the RMQ score is reduced by 30% from baseline.
The second disability questionnaire was the Oswestry Low Back Pain Disability Index (ODI). 24 The ODI has 10 items also referring to activities of daily living that might be disrupted by LBP. The total score ranges from 0 (no problem at all) to 50 (not possible). The Spanish version has shown good test–retest reliability (ICC, 0.92) and favorable internal consistency (Cronbach α, 0.86). 25 Ostelo and de Vet 26 reported that a change of 10 points is considered the MCID for the ODI.
A 10-point numeric pain rating scale (NPRS; 0: no pain, 10: maximum pain) was used to assess the patients' current level of pain and the highest and lowest levels of pain experienced in the preceding 24 hours. 27 The mean value of 3 scores was used in the analysis. The MCID in patients with chronic LBP has been reported to be 2.5 points. 27
The Tampa Scale of Kinesiophobia is a 17-item questionnaire developed to measure kinesiophobia (the fear of movement and [re]injury). 28 The total score ranges from 17 to 68 points, where higher values reflect greater fear of (re)injury. Test–retest reliability of the Tampa Scale of Kinesiophobia ranged from 0.90 to 0.96 in patients with chronic LBP. 28 The Spanish version also obtained good reliability (internal consistency and stability) and validity (convergent and predictive). 29,30
To test isometric endurance of trunk flexor muscles, we used the McQuade test. 31 Participants were studied supine with their arms crossed over their chest, hands on opposite shoulders, hips bent, and knees and feet apart. They were asked to nod and continue to lift their head and shoulders until the inferior angle of the scapula lifted off the table and to maintain the position as long as possible. 32 We recorded the number of seconds that the position was maintained up to a maximum of 120 seconds.
Lumbar mobility in flexion was determined by measuring the finger-to-floor distance with a tape. Participants performed a straight-legged forward trunk flexion from a standing position. Both arms stretched towards the floor with the palms facing the legs. The distance (in centimeters) from the tip of the third finger to the floor was measured after 2 seconds. The finger-to-floor distance has excellent intra-rater reliability (ICC, 0.96–0.98). 33
Hemoglobin oxygen saturation, systolic blood pressure, diastolic blood pressure, hemodynamic measures (cardiac index), and interstitial fluid biochemical estimation (levels of sodium, serum potassium, chloride, phosphate, ionized or free calcium, magnesium, and lactic acid) were determined with the Electro Interstitial Scanner (SISTEMA E.S. Complex v.2.5; L.D. Technology, Miami, FL). 34,35
Randomization
After the baseline examination, patients were randomly assigned to receive craniosacral therapy (experimental group) or classic massage (control group). Concealed allocation was performed by using a computer-generated randomized table of numbers created before the start of data collection by a researcher not involved in the recruitment or treatment of patients. Individual and sequentially numbered index cards with the random assignment were prepared. The index cards were folded and placed in sealed opaque envelopes. Another therapist, blinded to baseline examination, opened the envelope and proceeded with treatment according to the group assignment.
Outcome measures were assessed before the first treatment session (baseline data), after the 10-week intervention period (immediately after), and 1 month after the last treatment session (follow-up) by an assessor blinded to the treatment allocation of the patients.
Intervention
All treatments were applied by two experienced therapists with a 10-year certification in manipulative therapy after completion of their physical therapy degree and more than 20 years of clinical experience with patients. All participants attended a physical therapy clinic once per week for 10 weeks (10 sessions).
Craniosacral therapy took 50 minutes and was conducted as follows: 36 –38
With pelvic diaphragm release, palms are placed in transverse position on the superior aspect of the pubic bone, under the L5–S1 sacrum, and finger pads are placed on spinal processes. With respiratory diaphragm release, palms are placed transverse under T12/L1 so that the spine lies along the start of fingers and the border of palm, and the anterior hand is placed on the breastbone. For thoracic inlet release, the thumb and index finger are placed on the opposite sides of the clavicle, with the posterior hand/palm of the hand cupping C7/T1. For the hyoid release, the thumb and index finger are placed on the hyoid, with the index finger on the occiput and the cupping finger pads on the cervical vertebrae. With the sacral technique for stabilizing L5/sacrum, the fingers contact the sulcus and the palm of the hand is in contact with the distal part of the sacral bone. The nondominant hand of the therapist rested over the pelvis, with one hand on one iliac crest and the elbow/forearm of the other side over the other iliac crest. For CV-4 still point induction, thenar pads are placed under the occipital protuberance, avoiding mastoid sutures.
Classic massage protocol was compounded by the following sequence techniques of soft tissue massage on the low back: effleurage, petrissage, friction, and kneading. The maneuvers are performed with surface pressure, followed by deep pressure and ending with surface pressure again. The techniques took 30 minutes. 39
Sample size
The sample size was calculated by using Ene 3.0 software (Autonomic University of Barcelona, Spain). The calculations were based on detecting differences of 2.5 points in the RMQ (MCID), 26 assuming a standard deviation (SD) of 2.5 points, a two-tailed test, an α-level of 0.05, and a desired power (β) of 85%. The estimated desired sample size was calculated to be 32 participants per group.
Statistical analysis
Statistical analysis was performed using SPSS statistical software, version 18.0, and it was conducted according to principles of intention-to-treat analysis. Mean, SD, and/or 95% confidence intervals were calculated for each variable. The Kolmogorov–Smirnov test showed a normal distribution of the data for all baseline variables (p > 0.05). Linearity was examined by using bivariate scatter plots of observed residual values against the expected values. Baseline demographic and clinical variables were compared between both groups using Student t-tests for continuous data and chi-square tests for categorical data. Analysis of covariance (ANCOVA) was used to analyze for differences between the two groups in all patient-rated outcomes (RMQ as primary outcome) at post-treatment and 1-month follow-up. Baseline values were used as covariates. A separate 2 × 2 mixed-model ANCOVA with repeated measurements had to be conducted in order to test the effect with time (baseline and 4-week follow-up) as a within-subject variable. Effect sizes were calculated by using the Cohen d coefficient. An effect size less than 0.2 reflects a negligible difference; 0.2 or greater and less than 0.5, a small difference; between 0.5 or greater and less than 0.8, a moderate difference, and 0.8 or greater, a large difference. A p-value less than 0.05 was considered to indicate a statistically significant difference.
Results
Sixty-four patients (mean age ± SD, 50 ± 12 years; 66% female) satisfied all the eligibility criteria and agreed to participate. Of total patients included in the study, 28% showed lumbar pain related to work injuries. No mental health or depression/anxiety was reported in any patient. Reason for ineligibility are shown in Figure 1, which provides a flow diagram of patient recruitment and retention. In both groups, all baseline characteristics were similar (Table 1).
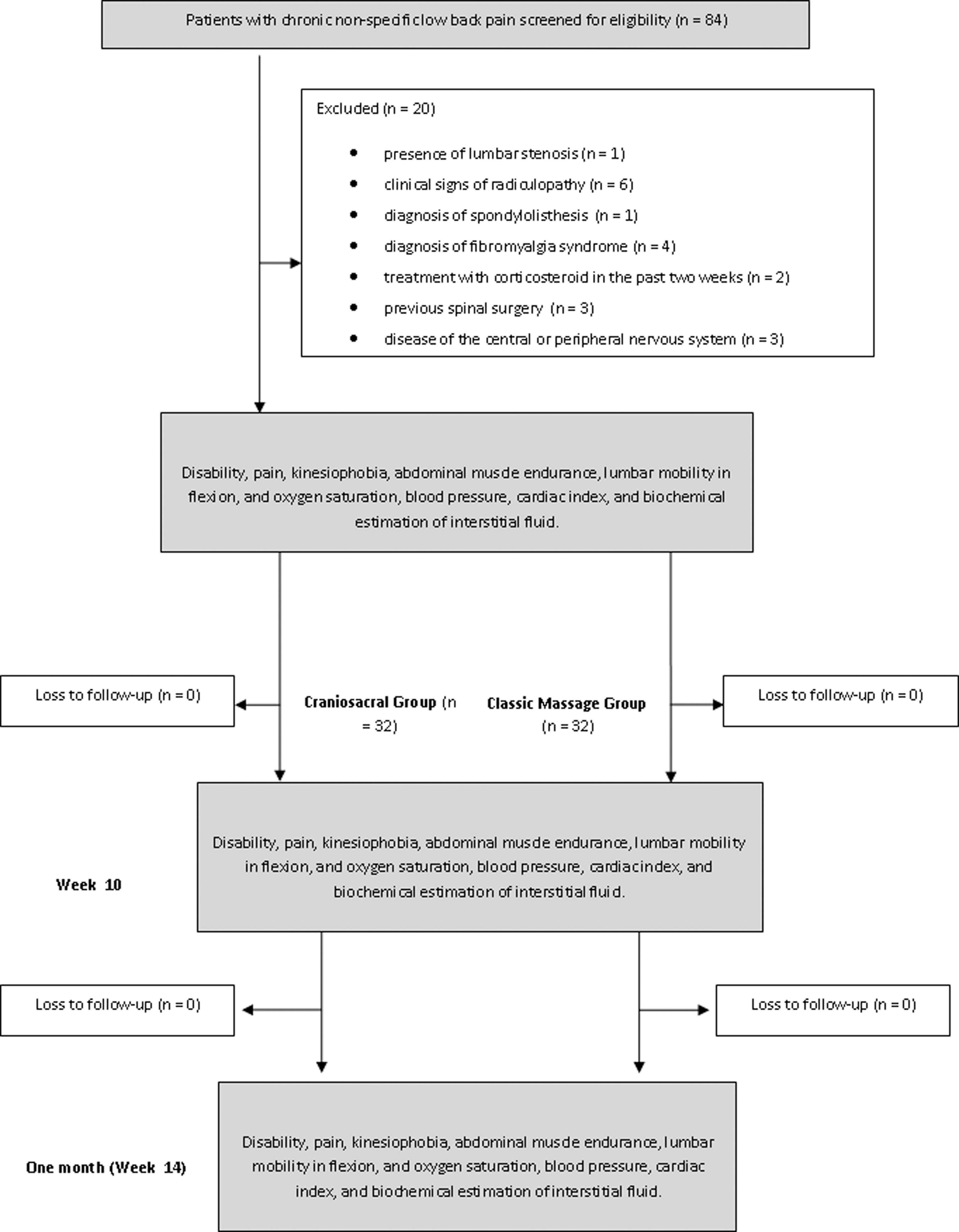
Flow diagram of patients throughout the study.
Unless otherwise noted, values are mean ± standard deviation.
Determined by chi-square test.
Determined by independent Student t-test.
RMQ, Roland-Morris Disability Questionnaire; ODI, Oswestry Low Back Pain Disability Index; NPRS, numeric pain rating scale; TSK, Tampa Scale of Kinesophobia.
The ANCOVA analysis did not show statistically significant differences between groups for the main outcome of the study, the RMQ (Table 2). The 2 × 2 repeated-measures analyses showed significant improvements in both groups over time (craniosacral: F = 8.11, p = 0.003; massage: F = 3.54, p = 0.034). After follow-up, RMQ decreased 1.81 points in patients receiving craniosacral therapy and0.81 in those receiving classic massage. Effect sizes were negligible (0.20) and small (0.31) after treatment in the control and experimental groups, respectively. At 1-month follow-up, effect sizes were small (0.28) and moderate (0.62) in the control and experimental groups, respectively.
Values are expressed as mean ± standard deviation for immediate post-treatment and 1-month follow-up and as mean (95% confidence interval) for between-group change scores.
p < .05, significant difference on analysis of covariance adjusted from baseline values for differences among groups.
CI, confidence interval.
Similarly, no statistically significant ANCOVA results were achieved for ODI in the between-groups analysis (Table 2). Repeated-measures analysis for ODI was also significantly for both groups (craniosacral: F = 73.13, p < 0.001; massage: F = 36.78, p < 0.001). At follow-up, disability scores decreased 11.81 points in patients who received craniosacral therapy and 9.10 points in those receiving classic massage. Effect sizes were large at post-treatment (craniosacral: 1.77; classic massage: 1.02) and follow-up (craniosacral: 1.51; classic massage: 1.02) in both groups.
ANCOVA analysis indicated statistically significant differences between groups for pain intensity (Table 2). The 2 × 2 repeated analysis for pain showed a significant reduction in both groups (craniosacral: F = 36.61, p < 0.001; massage: F = 11.92, p < 0.001); however, patients who received craniosacral therapy exhibited greater reduction in pain (within-group change score, 3.29) than those who received the classic massage intervention (within-group change score, 1.75) at follow-up. Effect size was large in both groups at all time points (post-treatment: craniosacral, 1.46; classic massage, 0.81; follow-up: craniosacral, 1.64; classic massage, 0.86).
ANCOVA analysis did not indicate statistically significant differences between groups for kinesiophobia, McQuade test, and finger-to-floor distance (Table 2). However, repeated-measures analysis showed a main effect over time within group experiencing similar decrease in McQuade test (craniosacral: F = 8.55, p = 0.001; massage: F = 4.91, p = 0.020) and finger-to-floor distance (craniosacral: F = 7.05, p = 0.002; massage: F = 6.39, p = 0.003) in both groups but not on kinesiophobia. Effect size was moderate in both groups for the McQuade test (post-treatment: craniosacral, 0.77; massage, 0.43; follow-up: craniosacral, 0.65; massage, 0.52) and small for finger-to-floor distance (post-treatment: craniosacral, 0.35; massage, 0.27; follow-up: craniosacral, 0.37; massage, 0.41).
ANCOVA analysis showed significant differences between groups in hemoglobin oxygen saturation and systolic blood pressure immediately after treatment and after follow up; however, differences for serum potassium, magnesium, and lactic acid were achieved only for the short term (Table 3). The 2 × 2 repeated-measures analysis showed a within-group effect over time only in the craniosacral group for hemoglobin oxygen saturation (F = 24.50, p = 0.021) and systolic blood pressure (F = 5.99, p = 0.008). Both groups showed changes from baseline in serum potassium (craniosacral: F = 3.79, p = 0.028; massage: F = 8.39, p = 0.001), magnesium (craniosacral: F = 4.67, p = 0.003; massage: F = 9.79, p = 0.001), and diastolic blood pressure (craniosacral: F = 3.58, p = 0.034; massage: F = 5.11, p = 0.009). Lactic acid (F = 6.75, p = 0.002) was increased significantly after treatment only in the massage group. Main changes over time were significantly better in the craniosacral group than in the massage group for potassium (craniosacral: 0.60–1.89; massage: 0.55–0.83) and magnesium (craniosacral: 0.70–1.92, massage: 0.58–0.83). Effect sizes were moderate for hemoglobin oxygen saturation (post-treatment: 0.58; follow-up: 0.49), systolic blood pressure (post-treatment: 0.43; follow-up: 0.45) and diastolic blood pressure (post-treatment: 0.24; follow-up: 0.39), serum potassium (post-treatment: 0.61; follow-up: 0.60), and magnesium (post-treatment: 0.64; follow-up: 0.63) in the craniosacral group. For the classic massage group, effect sizes were moderate for serum potassium (post-treatment: 0.07; follow-up: 0.49), magnesium (post-treatment: 0.006; follow-up: 0.55), and diastolic blood pressure (post-treatment: 0.006; follow-up: 0.42).
Values are expressed as mean ± standard deviation for immediate post-treatment and 1- month follow-up and as mean (95% confidence interval) for between-group change scores.
p < .05, significant difference on analysis of covariance adjusted from baseline values for differences among groups.
Discussion
The results of this randomized controlled trial suggest that 10 sessions of craniosacral therapy and 10 session of classic massage resulted in a statistically similar reduction in disability, pain intensity, isometric resistance of trunk flexors, spinal mobility, and diastolic blood pressure in patients with chronic LBP immediately after the intervention and at 1-month follow-up. However, the craniosacral therapy group showed better improvements in hemoglobin oxygen saturation, systolic blood pressure, serum potassium, and magnesium than did the massage therapy group.
Patients receiving craniosacral therapy experienced a greater reduction in disability RMQ (within-group change score, 1.81), but not significantly more so than those receiving classic massage (within-group change score, 0.81) at all follow-up periods. Nevertheless, these differences were below the MCID (≥2.5) established for RMQ, as identified by Bombardier et al. 22 Similarly, changes within groups for ODI did not reach the MCID (10 points) as identified previously by Ostelo and de Vet. 26 In addition, only minimal changes were found in isometric resistance of trunk flexors and spinal mobility. Cranial manipulations increase the mobility of the spinal dura mater, which may improve spinal mobility in patients with chronic overload. 38,39 However, disability in chronic LBP could be influenced by many other physical and psychological factors, and manual therapy on its own may not be enough to achieve clinical improvement. A multidisciplinary approach should thus be considered in future studies.
In this randomized controlled trial, both groups also experienced within-group reductions in pain intensity. However, the MCID for pain reduction established for patients with chronic LBP was surpassed only in the craniosacral group. 26 A similar report concluded that this therapy can reduce the intensity and frequency of pain in these patients. 17 In other studies among patients with fibromyalgia and lateral epicondylitis, pain levels decreased significantly after the application of craniosacral therapy. 8,9,12 However, these changes could be partially linked to a placebo effect, as reported by Xu et al. 40 in LBP patients treated with acupuncture. The current results agree with previous studies on craniosacral therapy in patients with fibromyalgia; however, intensity of pain and all quality-of-life dimensions except vitality showed statistically significant differences. 8,9
Finally, the current study also observed statistically significant differences between groups in hemoglobin oxygen saturation, systolic blood pressure, serum potassium, magnesium, and lactic acid. Craniosacral treatment focuses on the connective tissues of the skull and spine and on cerebrospinal fluid. These structures sustain the central nervous system from a physiologic point of view and influence the functioning of the autonomic nervous system. 41 A study on heart rate variability and the influence of craniosacral therapy on autonomous nervous system regulation in persons with subjective discomforts showed a favorable effect on autonomous nervous activity. 42 According to Greenman, 43 craniosacral treatment improves articular and membranous restrictions, reduces neural entrapment at the base of the skull, enhances the rate and amplitude of cranial rhythm, and reduces venous congestion. Several studies show that brain tissue and spinal cord motion appear to be related to the cardiac cycle. 44 However, the current results indicate that craniosacral therapy does not produce changes in the cardiac index.
The current study has several limitations. First, data were collected only at a short-term follow-up of 1 month. Second, only two clinicians performed the craniosacral therapy or classic massage interventions, which might limit the generalizability of the results. Third, the study did not include a no-treatment control group; therefore, it cannot be determined whether the improvements seen in both groups can be attributed to the interventions or simply the passage of time (Spanish legislation and the Declaration of Helsinki for clinical trials do not allow patients with a disabling illness to go untreated if other techniques that could improve the associated injury exist); however, this is unlikely because the patients' symptoms were chronic.
Conclusion
Ten sessions of craniosacral therapy and classic massage resulted in statistical (but not clinically meaningful) reductions in disability, pain intensity, isometric resistance of trunk flexors, spinal mobility, and diastolic blood pressure in patients with chronic LBP. However, craniosacral therapy showed better improvements in hemoglobin oxygen saturation, systolic blood pressure, serum potassium, and magnesium. Future trials should investigate the long-term effectiveness of these interventions in patients with LBP.
Footnotes
Acknowledgments
Investigators acknowledge with gratitude all patients who participated in this study. The authors declare no financial support. No funding was required for this study.
Author Disclosure Statement
No competing financial interests exist.