
Abstract
Background:
Neonatal abstinence syndrome (NAS) occurs within the first days after birth in newborns of mothers with a history of drug abuse. It may also occur in newborns whose mothers are undergoing substitution therapy.
Objective:
To determine the presence of active ear acupuncture points in newborn infants with NAS.
Methods:
Among newborn infants with NAS admitted to the Division of Neonatology at the University Hospital Graz between March 2009 and November 2014, an acupuncture-point detector (PS3 Silberbauer, Vienna, Austria) was used to identify active ear acupuncture points. An integrated optical and acoustical signal detects the ear points, which were then assigned to the ear map. A total of 31 newborn infants were assessed; 1 infant was excluded, however, because the mother had already weaned herself off opiates before admission.
Results:
The excluded infant did not develop signs of NAS, had a low Finnegan score (3 points), and did not present any detectable active psychic ear acupuncture points. In all included newborn infants with NAS, active ear acupuncture points were identified: The psychovegetative rim was the most common active somatic area in each infant, followed by a few somatic and psychic ear acupuncture points. In all infants with symptoms of NAS, active psychic ear points were identified, of which the most frequently found points were the Frustration point and the R point.
Conclusion:
The activity of psychic ear acupuncture points may be specific for neonates with NAS.
Introduction
R
There are different methods to help localize ear acupuncture points: (1) the use of an acupuncture-point detector (based on the electric characteristics) and (2) the pulse-controlled method (reflex auriculo cardiale, also called vascular autonomic reflex). 5,7 It is almost impossible to use the pulse-controlled method on newborn infants, however, because they respond to a pain impulse with mass movements; this makes the detection of any single specific pulse wave uncertain. 8 Several studies assessed active somatic and functional ear acupuncture points on the adult ear. 1,9 –11 Healthy adults usually have no electrically active ear acupuncture points, while the number of active ear acupuncture points correlates with disease severity. In comparison, evidence concerning ear acupuncture points in newborn infants is limited. 12,13 However, somatic active ear acupuncture points were identified showing a correlation between the disease of inner organs and the corresponding ear acupuncture point. The authors are the only group that has described psychic active ear acupuncture points in newborn infants, although these points are typically detectable in adults. 14,15
Intrauterine opioid exposure due to maternal opioid abuse or maternal opioid maintenance therapy during pregnancy can result in transient neonatal withdrawal or acute toxicity and is referred to as neonatal abstinence syndrome (NAS). 16 Most NAS cases develop on the background of intrauterine opioid exposure, 17 with the first symptoms usually occurring between 24 and 72 hours after birth.
In a small case series, Raith et al. identified active somatic and psychic ear acupuncture points in newborns with NAS. Withdrawal can be interpreted as a disorder composed of somatic and psychic symptoms.
Neonates with potential or confirmed exposure to intrauterine opioids can be assessed by using special scores, mainly the Finnegan score. 18 The Finnegan score consists of 20 different clinical parameter, including the central (e.g., irritability, high-pitched crying) and autonomic (e.g., sniffing, yawning) nervous system and the gastrointestinal (e.g., excessive sucking, reflux, diarrhea) and respiratory (e.g., tachypnea, apnea) systems, with a maximal score of 45. 18
The aim of this study was to (1) identify whether active somatic and/or functional (e.g., psychic) ear acupuncture points are present in newborn infants with NAS, (2) determine whether there is a correlation between the number of identified active ear acupuncture points and the health status of the newborn infant, and (3) ascertain whether these active ear acupuncture points are specific to newborn infants with NAS.
Materials and Methods
Patients and setting
Eligible for this research were all newborn infants who were born to mothers undergoing opioid substitution treatment with the potential to develop NAS and were admitted to the Division of Neonatology, University Hospital of Graz, a tertiary neonatal intensive care unit (NICU). This is an analysis of secondary outcome data of a randomized controlled trial (RCT) comparing laser acupuncture with pharmacologic therapy (acupuncture group) to pharmacologic therapy alone (control group). 19 The active ear acupuncture point analysis has not yet been published. The trial was conducted between March 2009 and November 2014 (Registry DRKS-ID: DRKS00004302).
Infants were excluded in cases of maternal polysubstance abuse, excessive alcohol consumption causing fetal alcohol syndrome, and a congenital abnormality that might have adversely affected the neurologic status of the infants. The Ethics Committee of the Medical University of Graz approved the trial. The parents of the infants were comprehensively informed about the study and gave informed consent.
Finnegan score
All members of the NICU involved in the study were trained to recognize signs of NAS and were familiar with the Finnegan scoring system. By using the Finnegan score, the infant was assessed three times daily by the bedside nurse and the physician in charge.
Once the Finnegan score totaled greater than 24 on three consecutive assessments or there was a single Finnegan score greater than 12, pharmacologic treatment was started in both groups, according to the standardized treatment protocol.
Acupuncture-point detector
The commercially available acupuncture-point detector PS3 (Silberbauer, Vienna, Austria) was used to identify active ear acupuncture points. The PS3 has an integrated optical and acoustical signal to detect active ear points. Once these active ear points were identified, they were assigned to the ear map according to Chinese and French nomenclature. 20
Data collection and analysis
The demographic and clinical characteristics of the study infants were recorded. The data are presented as mean (± standard deviation) for normally distributed continuous variables and median (± interquartile range [IQR]) when the distribution was skewed. The Mann-Whitney U test was used for comparisons between sexes, and the Spearman rank-correlation coefficient was calculated to analyze associations between the number of active ear points and the Finnegan score. SPSS software, version 20 (IBM SPSS Statistics, Chicago, IL) was used for the data analysis. A p-value less than 0.05 was considered to represent a statistically significant difference.
Results
Forty newborn infants with a diagnosis of NAS were admitted to the NICU during the study period. Nine newborn infants were not enrolled because of substance misuse (n = 4), refusal to consent (n = 4), and the fact that one mother (n = 1) was in trusteeship and therefore unable to give consent for the study within the time frame.
The study flow chart is presented in Figure 1. Baseline demographic characteristics, Finnegan score at time of examination, administration of oral morphine, and number of active ear points are presented in Table 1. One infant did not exhibit clinical signs for NAS at the time of examination. No active ear acupuncture points were detectable in this infant. The mother, who had been referred for substitution therapy, explained that she had weaned herself off opiates during pregnancy; the neonate was thus excluded. The excluded newborn had a low Finnegan score (3 points) and did not develop signs of NAS during hospitalization. Thirty infants enrolled in the initial RCT were further analyzed in the current study.
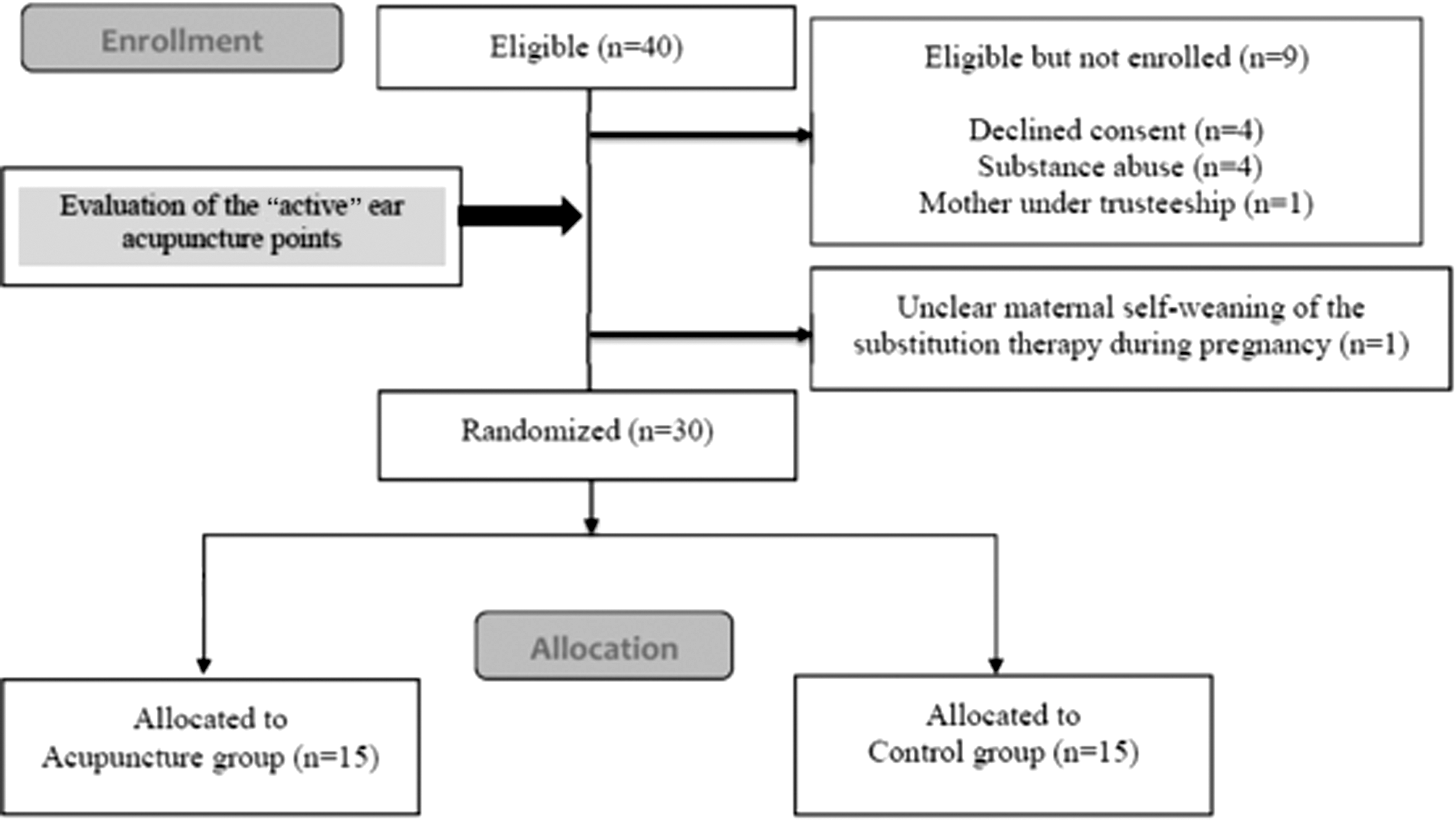
Study flowchart.
Values with ranges in parentheses are median (interquartile range).
Timepoint after birth when the examination was performed, given in hours pp (postpartum).
Section, cesarean section; NA pH, umbilical artery pH.
In the initial trial, before randomization all the newborns included were assessed for active ear acupuncture points. Active ear acupuncture points were identified in all the newborn infants; however, in two infants they were identified only in one ear (left ear frustration point in one of these infants and right ear frustration point and PT 1 in the other). The median (IQR) number of active ear acupuncture points did not differ for male (10.5 [5–13]) or female (10 [6–15]) infants (p = 0.913). The data are presented in Table 2.
Neonate no. 22 was excluded.
Somatic ear acupuncture points
The psychovegetative rim was the most frequently detected active somatic ear acupuncture point in newborn infants with NAS (n = 30/30). The psychovegetative rim is described as an area lateral to the scaphoid fossa below the helical flange (Table 3; Figs. 2 and 3).
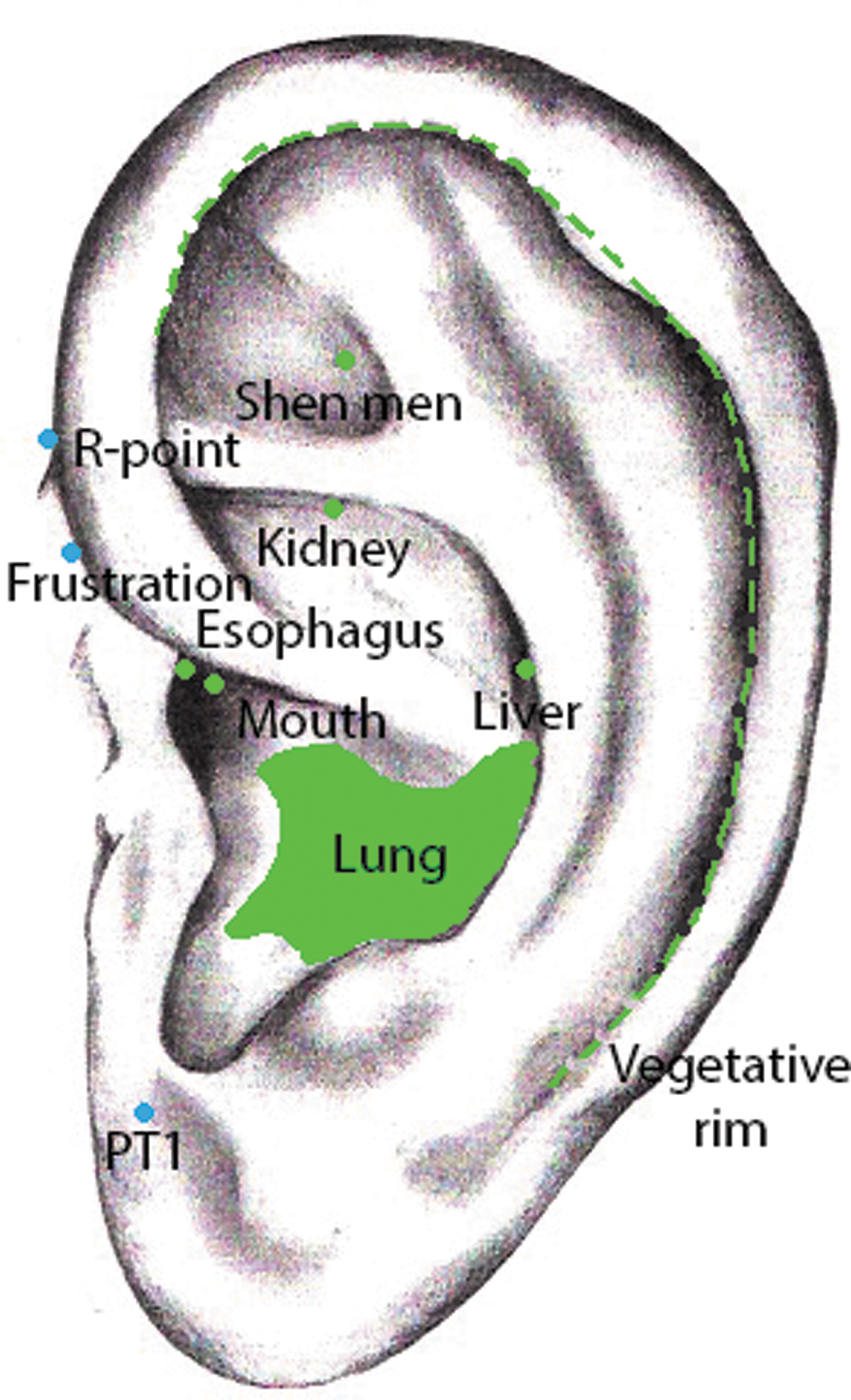
Topography of the most commonly found somatic and psychic active ear acupuncture points. Green, somatic ear points; blue, psychic ear points. Color images available online at
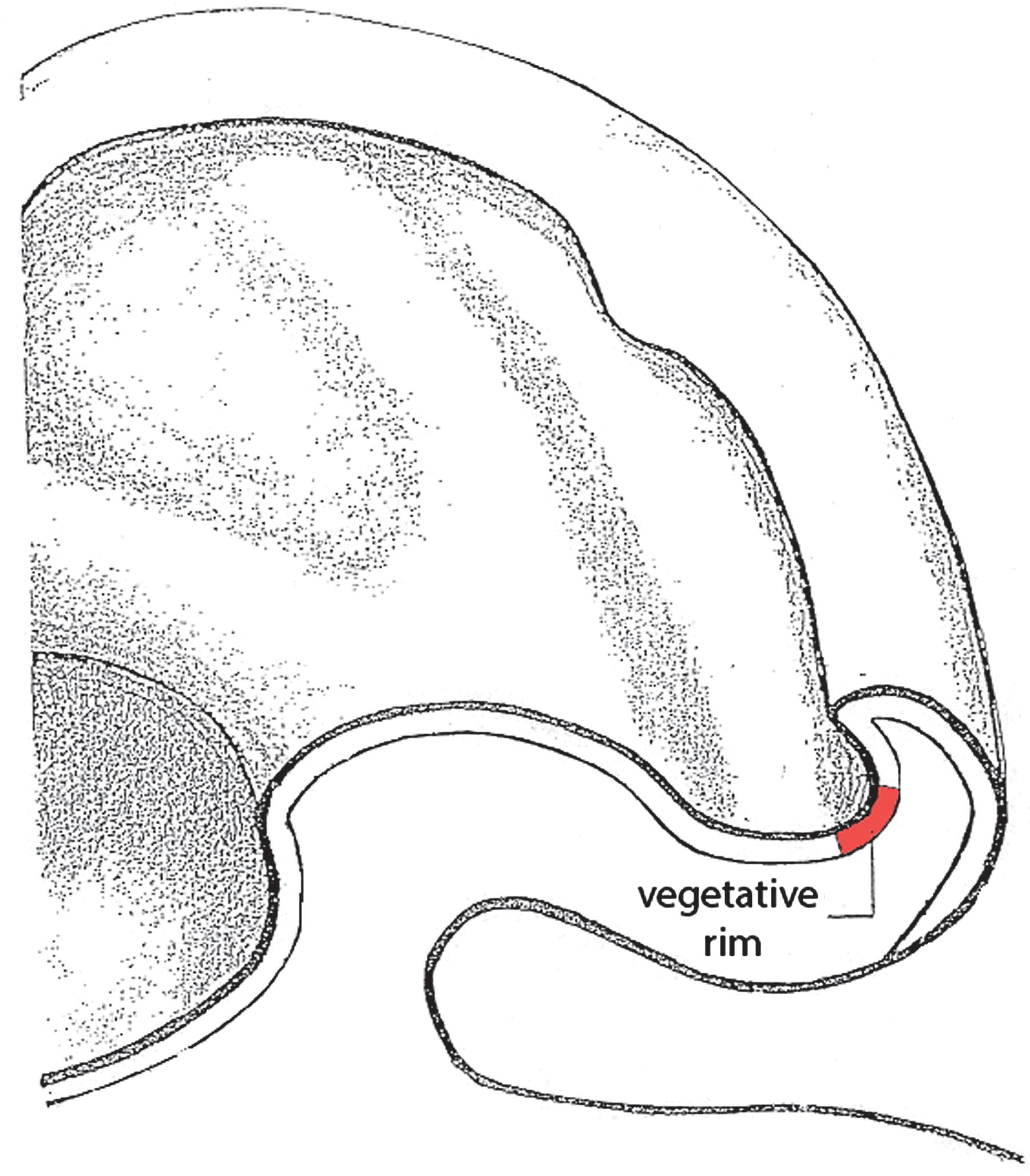
Cross-sectional display of the ear showing the area of the vegetative rim. Color images available online at
Values are expressed as number (percentage).
Functional ear acupuncture points
Psychic ear acupuncture points were found in all newborn infants diagnosed with NAS. The following active psychic ear acupuncture points were identified: R point (27 of 30), frustration point (23 of 30) and PT 1 (10 of 30) (Table 3; Fig. 2).
Discussion
The present study is an analysis of secondary outcome data of an RCT comparing laser acupuncture and pharmacologic therapy versus pharmacologic therapy alone in newborn infants with NAS. 19 In newborn infants with NAS, active somatic and functional (e.g., psychic) ear acupuncture points were detected, but no correlation between the severity of NAS and number of active ear acupuncture points was observed, and there was a trend toward a higher Finnegan score with more active ear acupuncture points (r = 0.338; p = 0.073). It is possible that the activity of the psychic ear acupuncture points is specific for neonates with NAS.
The psychovegetative rim was the most frequently detected active somatic ear acupuncture area, which was identified in all the newborn infants included in the study. The term “vegetative rim,” used mainly by German-speaking authors, was probably introduced in 1971 by Günter Lange, who assumed that the line of points located on the scaphoid groove very close to the internal border of the helix was essential for regulating the functions of a disturbed segment of the body according to Nogier's principle of alignment. 21 Nogier hypothesized that this part of the auricle could represent the intermediolateral nuclei of the lateral horn, the cells of which give rise to the preganglionic sympathetic outflow. He never, however, designated this line of points the “vegetative” rim or groove. Furthermore, Chinese authors have never included this term in their standardized auricular map from 1993 to 2008. 22
Further active somatically active ear acupuncture points were the lung (15 of 30), the esophagus (9 of 30), and the mouth (6 of 30). Similar results have been previously reported by van Amerongen et al. in healthy neonates. 12,13
Several psychic ear acupuncture points, including R point (27 of 30), frustration point (23 of 30), and PT 1 (10 of 30), were identified. This study illustrates that active psychic ear acupuncture points are present in infants with NAS. The overall clinical profile of an NAS neonate includes central nervous, gastrointestinal, respiratory, and vegetative symptoms. In most cases, a relationship between symptoms of NAS as identified on the Finnegan scale and the active auricular acupuncture points was determined, but no correlation between the severity of NAS and the number of active ear acupuncture points was observed.
One infant did not develop NAS because of maternal self-weaning of her substitution therapy at 6 months of pregnancy. The investigator was unaware of this at the time of the assessment. During the assessment, no active psychic ear acupuncture points were identified, and the newborn infant was in relatively good clinical condition, not presenting any withdrawal symptoms. This suggests that active psychic active ear acupuncture points might be present only in infants with NAS.
The active ear acupuncture points most frequently identified in the newborn infants in this study resemble active ear acupuncture points used by the National Acupuncture Detoxification Association (NADA) for withdrawal treatment in adults. 23,24 The NADA uses the ear acupuncture points (Shen Men, sympathetic, Liver, Kidney, and Lung) in the setting of a standardized protocol. However, the data on NADA acupuncture treatment in newborn infants with NAS are limited.
For example, Schwartz et al. 25 reported a trend toward less pharmacologic support in the acupressure-treated infants following the NADA points compared with standard treatment. Janssen et al. randomly assigned pregnant women to NADA acupuncture or standard care and found no difference in the average length of morphine treatment with morphine for newborn infants and the newborns with NAS. However, a post hoc analysis among newborn infants of women who were adherent to the acupuncture regimen, compared with the nonadherent and control groups, showed a potentially shorter duration of NAS. But these differences were not statistically significant.
In the recently published RCT, NADA ear acupuncture was combined with body acupuncture; the duration of oral morphine therapy and the length of stay were significantly reduced in the acupuncture group compared with the control group. 19,26
The current study had some limitations. The small number of included cases is related to the low incidence of NAS in Austria compared with other European countries or North America. 27,28 In addition, all the newborn infants included in the study were examined just once. Furthermore, the assessor of the active ear acupuncture points was aware that all the infants had been diagnosed with NAS.
Yet another limitation is the so-called acupuncture-point detector itself. As mentioned earlier, there are different methods for identifying active ear acupuncture points, and the sensitivity and positive predictive value of the acupuncture-point detectors have been questioned. 5 Because of the immature pain perception in newborn infants, however, it would appear to be impracticable to use the pulse-controlled method. 8
Conclusion
Most active ear acupuncture points were found in the psychovegetative rim. However, some active somatic ear acupuncture points could also be identified. The activity of psychic ear acupuncture points may be specific for neonates with NAS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.