
Abstract
Objectives:
The objective of this study was to examine the potential relationship between different forms of complementary and alternative medicine (CAM) use and falls among older adults in New York City (NYC).
Design:
This cross-sectional study of data from the NYC Health Indicators Project survey used modified questionnaire items from several national surveys.
Settings:
Participants were recruited from 56 senior centers located in the 5 boroughs of NYC.
Participants:
There were 1273 participants aged 60 years or older included in the final analysis.
Outcome measures:
Of particular interest to the researchers was a dichotomous outcome variable for falls, indicating that an individual had experienced no falls during the past year or one or more falls. Also of interest in the analyses were five CAM therapy types: alternative medical systems, biologically based therapies, manipulative and body-based therapies, mind–body therapies, and movement therapies.
Results:
Prevalence of falls in NYC was 26.8%, which is consistent with the national average. Prevalence of CAM use was 92%. Participants who had tried manipulative and body-based therapies were more likely to report falling in the past 12 months (odds ratio, 1.65; 95% confidence interval, 1.26–2.15), after adjustment for age and sex. This observed association may reflect older adults with chronic pain who are already at risk for falling and are seeking therapy for this pain. None of the other CAM types were significantly associated with falls.
Conclusions:
Because of the growing popularity of CAM use within this population, CAM practitioners should be included in falls prevention strategies. Particular attention should be taken to include practitioners who provide manipulative and body-based therapies (e.g., chiropractors, osteopaths, physical and massage therapists) because of the high risk for falls observed among individuals who use these therapies.
Introduction
F
Use of complementary and alternative medicine (CAM) has been increasing steadily in the United States among those aged 65 years and older according to data from the 2002, 2007, and 2012 National Health Interview Survey (NHIS). 4 CAM includes a wide array of approaches for preventing or treating disease that are not part of conventional medicine. 5 According to data from the 2002 NHIS survey, the chronic conditions for which CAM was most often used included back, neck, or other joint pain; anxiety; and depression. 6 CAM types have been previously categorized into the following four categories: alternative medical systems, biologically based therapies, manipulative and body-based therapies, and mind–body therapies. 5 The objective of this study was to determine whether overall CAM use and specific CAM modalities are associated with falling.
Materials and Methods
Data
This paper presents findings from a secondary analysis conducted on data collected from April through November 2008 from a cross-sectional survey of older adults aged 60 years and older attending NYC senior centers. The Health Indicators Project was conducted by the Brookdale Center for Healthy Aging and Longevity at Hunter College, funded by the Mayor's Office, and administered by the Department for the Aging. This was the first health and social assessment of older adults aged 60 years and older attending senior centers in NYC. The initial assessment included a representative sample of 1870 older adults, recruited by a systematic selection process, who were attending 56 senior centers across the five boroughs: 10 in the Bronx, 16 in Brooklyn, 13 in Manhattan, 14 in Queens, and 3 in Staten Island. The stratified random sampling design was based on borough, senior center size, and race/ethnicity. Exclusion criteria included being younger than 60 years, having overt mental illness, not cooperating, being too ill to participate, or not speaking the selected languages. At each senior center, prospective participants registered as they entered the center, and then every third person was selected for participation.
The comprehensive, structured survey instrument consisted of standardized questionnaire items from validated national and local surveys, such as the Behavioral Risk Factor Surveillance System, the NHIS, the Medicare Current Beneficiary Survey, and the New York City Community Health Survey. The full survey instrument can be found in Appendix 3 of the 2010 NYC Senior Center Survey Final Report, titled “Brookdale Demonstration Initiative in Healthy Urban Aging: Bridging the Divide Between Public Health & Healthy Aging” (
Study sample
Originally, 1870 responders were interviewed. There were 597 participants excluded from our analyses for missing responses to our variables of interest: demographic, clinical characteristics, and CAM use variables. The final analytic sample presented here was restricted to 1273 participants with complete data on all of these included study variables.
Measures
Variables representing the different CAM categories were modifications based on the report from the National Center for Complementary and Integrative Health and National Center for Health Statistics using data from the 2007 NHIS and are further described in Figure 1. Final CAM modalities included alternative medical systems, biologically based therapies, manipulative and body-based therapies, mind–body therapies, and movement therapies. The 2007 NHIS categorized yoga, t'ai chi, and qi gong under mind–body therapies and included movement therapies (Feldenkrais, Alexander technique, Pilates, and Trager psychophysical integration) as a subcategory within the manipulative and body-based therapies category. For this study, movement therapy was considered its own therapy category and included only yoga, t'ai chi, and qi gong. For each therapy, a positive response to having ever tried any one of the CAM types described resulted in a positive response to the composite variable.
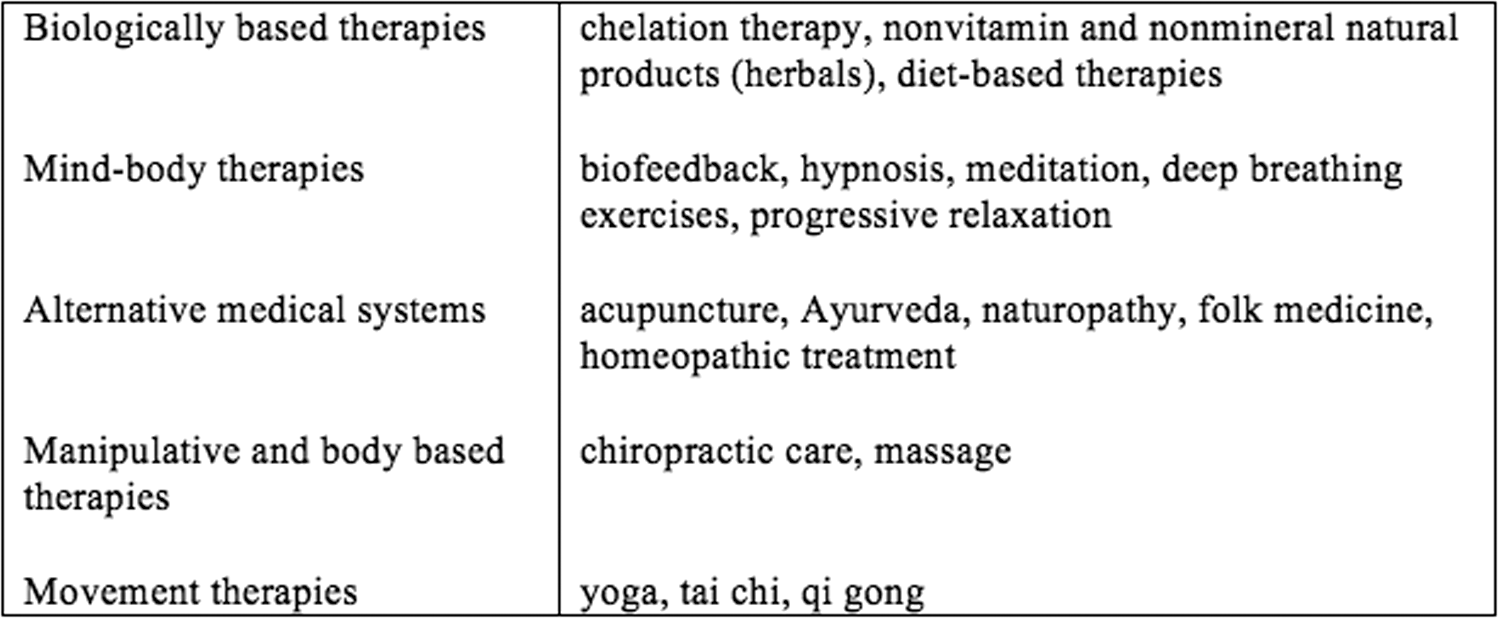
Types of complementary and alternative medicine. Modified from the report from the National Center for Complementary and Integrative Health and the National Center for Health Statistics. 5
The outcome of interest was whether the respondent had fallen in the last year. The final falls variable included both participants reporting a single fall or multiple falls in the year before the interview. Various demographic and clinical characteristics were collected. Composite variables for chronic conditions were created on the basis of classifications by Freedman et al. to account for the effects of related factors on functional impairment. 7 These variables are described in Table 1.
A scale variable was created to determine the combined level of difficulty individuals had with IADLs and ADLs.
Composite variables: medication-related risk factors (polypharmacy defined as the use of four or more medications or taking medications for anxiety, depression, or stress), metabolic conditions (diabetes or obesity), musculoskeletal conditions (neck, back, or other joint pain or arthritis), heart and circulatory problems (coronary heart disease, heart attack, or other), mental and emotional problems (mild depression, moderate to severe depression, or anxiety), sensory impairment (hearing- or vision-related).
Complementary and alternative medicine composite variables previously described in Figure 1.
SD, standard deviation; IADL, instrumental activities of daily living (i.e., shopping and preparing meals); ADL, basic activities of daily living (i.e., walking and bathing).
Analysis
Frequencies with percentages and means with standard deviations were used to describe the sample. A separate logistic regression model was created for each CAM therapy category to examine the potential relationship to the falls outcome. All logistic models were adjusted for age and sex. Data were analyzed using SAS v9.3 (SAS Institute, Cary, NC).
Results
Demographic characteristics, clinical variables, and CAM use for the full cohort are reported in Table 1. Of the 1273 participants with complete data, 223 respondents reported one fall and 118 reported two or more falls in the last 12 months, totaling 341 (26.8%) fallers in the sample. Almost 92% of the sample reported having tried any one CAM modality, with around half of the respondents having tried mind–body therapies and biologically based therapies, and about one quarter having tried alternative medical systems, manipulative and body-based therapies, and movement therapies.
Logistic regression models for each CAM modality to assess the association of falling are reported in Table 2. Among the five CAM modalities, manipulative and body-based therapies was the only one significantly associated with falling (odds ratio, 1.65; 95% confidence interval, 1.26–2.15), after adjustment for age and sex.
All CAM logistic regression models were adjusted for age and sex.
CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval.
Discussion
The prevalence of falls in older New Yorkers (26.8%) was similar to the national average of approximately one in three older adults. 1 Prevalence of ever using CAM (92%) was higher than the older adult population's national prevalence of 12-month CAM use (41%–63%). 8 This study evaluated the relationship between CAM use and risk for falling among older adults in NYC who were attending senior centers.
Chronic pain is associated with an increased risk for falls, and neck, back, and other chronic pain are primary reasons that older adults seek forms of manipulative and body-based therapies (defined here as chiropractic care or massage). 9 In the current analysis, having tried manipulative and body-based therapies was associated with falling. The observed association between falling and having tried manipulative and body-based therapies may reflect older adults with chronic pain (who are already at risk for falling) seeking therapy for this pain. Given the high prevalence of manipulative and body-based therapies use by high-risk older adults, all of the relevant practitioners using these therapies (e.g., chiropractors, osteopaths, physical therapists, and massage therapists) should be knowledgeable with current best practice in falls prevention and incorporate falls assessments and interventions into their practice. The Stopping Elderly Accidents, Deaths, and Injuries (STEADI) fall prevention toolkit is an example of a free, evidence-based resource that any practitioner can use to assess an individual's risk and to provide individualized fall interventions. 10
Several limitations must be considered. It was not the authors' intention, nor was it possible with a cross-sectional study, to infer causality from the results. Nearly 600 participants did not have complete data and were excluded from the analysis, so the results may be biased for including only completers. Falls were self-reported, which likely indicates that they were underreported. Regarding CAM use, the survey asked whether the respondents had “ever tried” the modalities and did not probe further as to whether the respondent continued use or when the last use was. This makes it difficult to compare CAM use among New Yorkers with data from the national population. CAM modalities were grouped variables; therefore, it cannot be determined from this analysis whether one specific CAM type was associated with self-report of a single fall or multiple falls. Further, the regression models presented here were adjusted only for age and sex and did not include all of the known risk factors for falls.
Conclusions
Both the prevalence of falls and CAM use are rising among the older adult population. Manipulative and body-based therapies are often used to mitigate symptoms of conditions that are associated with falling. Furthermore, because of their high access to patients/clients who self-report falls, CAM practitioners whose practices include manipulative and body-based therapies should be included in efforts to implement falls evidence-based strategies.
Footnotes
Acknowledgments
Funding for the Health Indicators Project was provided by the Mayor's Office and administered by the New York City Department for the Aging. This research is supported in part by grant 1 R49 CE002096-01 from the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, to the Center for Injury Epidemiology and Prevention at Columbia University. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. This research is also supported in part by the Malka Fund.
Author Disclosure Statement
No competing financial interests exist.