
Abstract
Background:
Traditional Chinese Medicine (TCM) uses a sophisticated diagnostic system called pattern differentiation, which allows for the tailor-made treatment of individuals.
Objective:
This study aimed to identify the commonly used TCM patterns for lateral elbow pain (LEP), as well as the clinical features associated with these patterns.
Method:
Journal literature in 15 major Chinese and English databases and textbooks from five medical libraries as well as Chinamaxx were reviewed.
Results:
Five hundred and fifty-five full-text journal articles, as well as 465 textbooks, were retrieved for further assessment, but only eight studies and seven books that mentioned LEP patterns could be identified and included in this study. The top four patterns that were identified were the wind-cold-dampness pattern, the qi stagnation and blood stasis pattern, the dual deficiency of qi and blood pattern, and the retained dampness-heat pattern, each of which was associated with unique features that were made up of distinct signs and symptoms.
Conclusions:
The unique features identified for each of the major patterns might be the key to understanding TCM individualized treatment based on pattern differentiation. Furthermore, the approach taken in studying TCM pattern of LEP may also be useful for studying the TCM patterns of other musculoskeletal conditions.
Introduction
M
Lateral elbow pain (LEP) or tennis elbow is a common musculoskeletal pain condition with a prevalence of at least 1–3%, and acupuncture, among other TCM therapies, is frequently used to treat LEP. 7,8 Pattern differentiation is frequently used in TCM and particularly in acupuncture practice. However, a recent systematic review on the efficacy of acupuncture for LEP found that pattern differentiation was rarely described in clinical trial studies. This may be due to the lack of standardization and disagreement on the method of pattern differentiation, which may hamper clinical efficacy and the generalizability of TCM clinical trials. 9,10 An investigation of common symptoms of TCM patterns for LEP and, moreover, standardizing these LEP patterns could generate new knowledge about the pathophysiological mechanisms for the disease subtypes. This would not only be useful for TCM practitioners, but also Western medicine physicians, who may be able to use these insights to distinguish subtypes of LEP in clinical practice. This study, therefore, set out to investigate the textual evidence (publications and texts) of pattern differentiation for LEP in TCM. This aim will be achieved by conducting a systematic review, including a review of journal articles and a review of TCM textbooks to identify the commonly encountered TCM patterns and their associated symptoms in LEP in the literature. The study also aimed to explore potential biological mechanisms that may underlie different TCM patterns.
Materials and Methods
This systematic review was separated into a journal article review and a textbook review, with the goal of identifying what both academics and clinical researchers have found about LEP patterns and their associated clinical features. This may help the generalizability and representativeness of the findings.
Journal articles review
Eligibility criteria
Included articles were randomized clinical trials and case-series studies, with a minimum number of 20 participants, in the English or Chinese language, of subjects with a primary diagnosis of lateral epicondylitis or lateral epicondyle pain in which any TCM treatment (acupuncture, moxibustion, cupping, TCM herbal therapy, etc.) was used alone, in combination with each other, or in combination with Western medicine and/or physiotherapy. Articles were excluded if they did not deal with first-hand patient information, such as discussion papers, or did not mention that pattern diagnosis was performed.
Search strategies
For the journal article review, the following databases were searched from their inception to January 2015: PubMed (from 1948), MEDLINE (from January 1966), Cochrane Neuromuscular Disease Group Trials Register for randomized trials, the Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE (from January 1974), LILACS (Latin American and Caribbean Health Sciences), Allied and Complementary Medicine (AMED, from 1985), Index to Chinese Periodicals of Hong Kong (HKInChiP, from 1990), and the Chinese Biomedical Literature Database (CBM, from 1979). Search was also made in China National Knowledge Infrastructure (CNKI, from 1915),  ) or syndrome differentiation (
) or syndrome differentiation ( ) AND lateral epicondylitis or lateral epicondylalgia (
) AND lateral epicondylitis or lateral epicondylalgia ( ), or tennis elbow (
), or tennis elbow ( ), or lateral epicondyle (
), or lateral epicondyle ( ), or external humeral epicondylitis (
), or external humeral epicondylitis ( ), or lateral elbow (
), or lateral elbow ( ) AND acupunc* (
) AND acupunc* ( *), or mox* (
*), or mox* ( *), or electro-acupunc* (
*), or electro-acupunc* ( *), or needle (
*), or needle ( ), or TCM or Chinese medicine (
), or TCM or Chinese medicine ( ), or tuina (
), or tuina ( ), or acupress* (
), or acupress* ( *), or scalpel therapy (
*), or scalpel therapy ( ), or scraping (
), or scraping ( ), or cupping (
), or cupping ( ), or auricular* (
), or auricular* ( *).
*).
Study selection
M.G. and H.Y.Y. searched the databases and assessed potentially relevant articles against the inclusion criteria independently. Any disagreement regarding the eligibility of a study was resolved by discussion.
Data extraction
M.G. extracted the data. For each study, the following variables were extracted: study design; treatment regime and control intervention, if any; sample size; mode of recruitment; sampling and diagnostic procedure; diagnostic criteria for LEP; inclusion and exclusion criteria; participants' characteristics, including age, sex, and duration of condition; and information regarding the TCM pattern, including symptoms and signs of each TCM pattern and number of subjects belonging to each pattern. All Chinese to English translations were deduced primarily from the World Health Organization (WHO) International Standard Terminologies on Traditional Medicine in the Western Pacific Region. 4
TCM textbook literature review
The textbook literature review was conducted mostly within the Chinese literature using the Chinamaxx database. This is the world's largest and most complete online database of Chinese publications, with >700.000 titles of Chinese books published since 1949. It also contains the Medical Library Collections (MLC), which is an online union collection of medical materials indexed in the online catalogues of five academic medical libraries in Hong Kong, including the Hong Kong Baptist University (HKBU) Chinese Medicine Library, which alone has >31,000 volumes of TCM books.
TCM textbooks (reprints of classic books, teaching material, clinical practice-orientated books) published after 1949 were searched for the following titles: TCM diagnosis ( ) or acupuncture therapy (
) or acupuncture therapy ( ) or orthopedics (
) or orthopedics ( ). A search was also made for the following keywords in both the Chinese and English language: lateral epicondylitis (
). A search was also made for the following keywords in both the Chinese and English language: lateral epicondylitis ( ) or tennis elbow (
) or tennis elbow ( ) or painful elbow (
) or painful elbow ( or
or  ). Relevant literature was retrieved and hand-searched for the terms lateral epicondylitis (
). Relevant literature was retrieved and hand-searched for the terms lateral epicondylitis ( ) or tennis elbow (
) or tennis elbow ( ) or painful elbow (
) or painful elbow ( or
or  ). Books were included if they at least mentioned possible patterns underlying LEP. Patterns and their associated signs and symptoms were then extracted. Diagnostic criteria were also recorded.
). Books were included if they at least mentioned possible patterns underlying LEP. Patterns and their associated signs and symptoms were then extracted. Diagnostic criteria were also recorded.
Results
Journal articles review
General description of reviewed articles
The search identified 580 English and 1232 Chinese potentially relevant citations for review. After removal of duplicates and studies not fulfilling inclusion criteria, 26 English and 529 Chinese citations remained (Fig. 1). All 555 full-text articles were retrieved for further assessment. Finally, eight Chinese 11 –18 and no English studies met the inclusion criteria and were included in the review. An overview of the characteristics of these studies, including the patterns that were identified and the acupuncture-point protocols that were used, is presented in Table 1.

Flowchart journal review process.
TCM, acupoint selection based on Traditional Chinese Medicine theory; LEP, lateral elbow pain; RCT, randomized controlled trial; N, not performed; NA, not applicable; NR, not reported; Y, reported.
The sample size of the eight studies ranged from 30 to 112. The total sample size of all studies was 488. The average age of all subjects included in the eight studies was 43.5 years; 39.4% of the subjects where sex was reported were male. The duration of the condition reported ranged from 1 day to 12 years. All studies included were conducted in China and published in Chinese-language journals. The criteria used for the diagnosis of tennis elbow or LEP were based on the Criteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine 19 in four studies (50%). 11,13,15,18 One study (12.5%) 16 based its diagnosis on an untitled textbook's criteria. The remaining three studies (37.5%) 12,14,17 did not report the diagnostic criteria used, but mentioned primary symptoms such as pain and tenderness at lateral epicondyle or pain upon rotation of the forearm and pronation of the wrist.
TCM patterns
Sixteen different TCM patterns were reported in the eight studies, namely: (1) wind-cold obstructing the collaterals ( ), (2) cold-dampness exterior attack (
), (2) cold-dampness exterior attack ( ), (3) wind-cold (
), (3) wind-cold ( ), (4) retained dampness-heat (
), (4) retained dampness-heat ( ), (5) dual deficiency of qi and blood (
), (5) dual deficiency of qi and blood ( ), (6) qi and blood deficiency (
), (6) qi and blood deficiency ( ), (7) qi stagnation and blood stasis (
), (7) qi stagnation and blood stasis ( ), (8) qi and blood stasis (
), (8) qi and blood stasis ( ), (9) yang qi deficiency (
), (9) yang qi deficiency ( ), (10) hand yang brightness meridian sinew pattern (
), (10) hand yang brightness meridian sinew pattern ( ), (11) hand lesser yang meridian sinew pattern (
), (11) hand lesser yang meridian sinew pattern ( ), (12) hand lesser yang meridian pattern (
), (12) hand lesser yang meridian pattern ( ), (13) dual deficiency of liver and kidney (
), (13) dual deficiency of liver and kidney ( ), (14) blood failing to nourish the tendons (
), (14) blood failing to nourish the tendons ( ), (15) deficiency of yin and blood (
), (15) deficiency of yin and blood ( ), and (16) retained dampness-heat and blood stasis (
), and (16) retained dampness-heat and blood stasis ( ) (Table 2). The diagnoses of these patterns were based on: eight-principle pattern differentiation (1–4); qi-blood pattern differentiation (5–9); meridian pattern differentiation (10–12); visceral pattern differentiation (13), and various pattern differentiation (14–16). English translations of pattern names as well as stated categories of pattern differentiation method were based on the WHO standard terminologies on TCM.
4
) (Table 2). The diagnoses of these patterns were based on: eight-principle pattern differentiation (1–4); qi-blood pattern differentiation (5–9); meridian pattern differentiation (10–12); visceral pattern differentiation (13), and various pattern differentiation (14–16). English translations of pattern names as well as stated categories of pattern differentiation method were based on the WHO standard terminologies on TCM.
4


As shown in Table 3, some patterns share similar TCM pathophysiology and have largely overlapping symptoms, and therefore may be considered as a more general pattern. The (1) wind-cold obstructing the collaterals pattern, the (2) cold-dampness exterior attack pattern, the (3) wind-cold pattern share nine overlapping symptoms, and were grouped together under the generalized wind-cold-dampness pattern ( ). The (5) dual deficiency of qi and blood pattern and the (6) deficiency of qi and blood pattern share six overlapping symptoms and the terminologies used for the pattern names were almost identical and could be used interchangeably, and it was therefore decided to present them as the generalized dual deficiency of qi and blood pattern (
). The (5) dual deficiency of qi and blood pattern and the (6) deficiency of qi and blood pattern share six overlapping symptoms and the terminologies used for the pattern names were almost identical and could be used interchangeably, and it was therefore decided to present them as the generalized dual deficiency of qi and blood pattern ( ). Furthermore, the (7) qi stagnation and blood stasis pattern and the (8) qi and blood stasis pattern were grouped together as the generalized qi stagnation and blood stasis pattern (
). Furthermore, the (7) qi stagnation and blood stasis pattern and the (8) qi and blood stasis pattern were grouped together as the generalized qi stagnation and blood stasis pattern ( ) because the pattern names were almost identical (Table 2). The wording of these generalized patterns was chosen on the basis of authoritative texts.
4,19
) because the pattern names were almost identical (Table 2). The wording of these generalized patterns was chosen on the basis of authoritative texts.
4,19
Pathogeneses between the two patterns were the same or very similar.
By counting the number of studies in which a certain pattern appeared, the most frequently mentioned patterns were: the wind-cold-dampness pattern (five studies), the qi stagnation and blood stasis (four studies), the dual deficiency of qi and blood pattern (four studies), and the retained dampness-heat pattern (three studies). These top four patterns also account for 82.1% of the 318 subjects, whose pattern diagnoses were reported (Table 4).
Generalized patterns are marked in bold.
Although the (13) dual deficiency of liver and kidney pattern has a higher proportion of reported subjects than the retained dampness-heat pattern, it was not included as part of the top four patterns because the number of publications was used as the criteria for ranking the most frequent patterns, and the (13) dual deficiency of liver and kidney pattern only appeared in one study (Table 4).
Symptoms and signs associated with the patterns
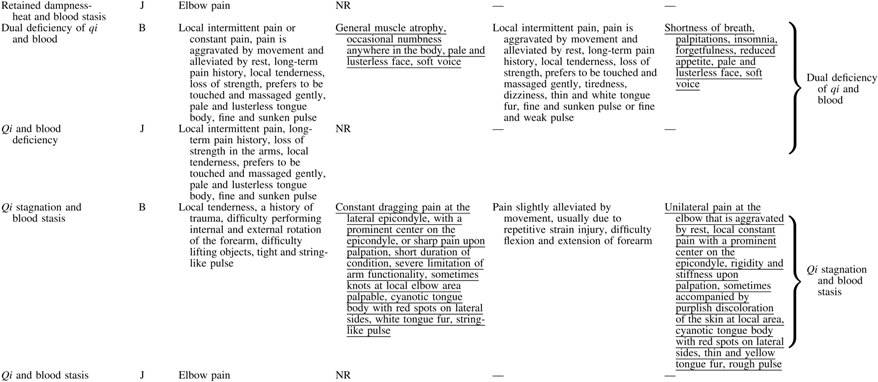
Table 2 (journal studies are on the left side) shows the signs and symptoms described with each pattern. Four of the eight (50%) included studies provided clinical features for 6/16 (37.5%) included TCM patterns. For the remaining 10 patterns, only the name of the pattern was mentioned, but no symptoms and signs were reported, except elbow pain. Local symptoms, systemic symptoms, as well as tongue and pulse features for the patterns were investigated. A total of 28 local symptoms were mentioned. Some symptoms were similar, such as “sensitive to pressure,” “tenderness,” “tender upon pressure,” and “dislikes pressure,” and therefore they were grouped together as “local tenderness.” Other symptoms appeared similar but were distinctively different upon further examination, and were therefore not grouped together. For example, pain at the elbow, dragging pain, constant pain, pain that comes and goes, sharp pain upon touch, numbing pain at the elbow, and occasional numbness at elbow were considered as individually distinct symptoms. The most frequently mentioned symptom was pain (of different nature) at the local elbow area.
Table 2 shows a summary of how different signs and symptoms make up the patterns. As displayed in the table, the majority of signs and symptoms were mentioned in more than one pattern. However, there are some signs and symptoms that are unique to a particular pattern.
Four out of the included 16 patterns were associated with five systemic symptoms. The remaining 12 patterns did not report any systemic symptoms. Seven types of tongue features were associated, and six types of pulse features were mentioned in six patterns. Common tongue and pulse features may be found in several patterns; for example, a pale and lusterless tongue body with a fine, or a fine and sunken pulse were mentioned in the (5) dual deficiency of qi and blood pattern and the (6) extreme dual deficiency of qi and blood pattern.
Unique signs and symptoms were found to be associated with five individual patterns: the (1) wind-cold obstructing the collaterals pattern, the (4) retained dampness-heat pattern, the (5) dual deficiency of qi and blood pattern, the (7) qi stagnation and blood stasis pattern, and the (15) blood failing to nourish the tendons pattern (Table 2). For example, local numbing pain was unique to the (1) wind-cold obstructing the collaterals pattern, whereas a pale and lusterless face, a soft voice, and muscle atrophy were only associated with the (5) dual deficiency of qi and blood pattern, and a thick and yellow tongue fur and a rapid and slippery pulse were unique to the (4) retained dampness-heat pattern.
Textbook literature review
General description of reviewed literature
The search yielded a total of 1011 potentially relevant books and e-books. After removing duplicates and studies not fulfilling inclusion criteria, 438 Chinese and 27 English textbooks were retrieved for further assessment. In the selection process, titles that were commonly used by TCM universities in China for academic and clinical purposes were specifically included. Finally, only six Chinese 19 –24 and one English book 25 mentioned the actual pattern differentiation for LEP as well as the symptoms for each pattern (Fig. 2).

Flowchart textbook review process.
Even though a large amount of the retrieved books and e-books mentioned the term lateral epicondylitis or a variation thereof, for example “pain in the elbow or elbow strain ( )” along with describing commonly seen TCM pathogeneses as well as the TCM concept of LEP, they did not mention an actual pattern by mentioning a specific pattern name (
)” along with describing commonly seen TCM pathogeneses as well as the TCM concept of LEP, they did not mention an actual pattern by mentioning a specific pattern name ( ).
).
TCM patterns
The included seven textbooks mentioned 13 different patterns. Seven patterns from the journal review were not found in the textbooks review (Table 2). However, four additional patterns that were not previously identified in the journal review were found in the textbooks. These were: (17) cold-dampness invading the inside ( ), (18) cold-dampness leading to qi stagnation and blood stasis (
), (18) cold-dampness leading to qi stagnation and blood stasis ( ,
,  ), (19) dual deficiency of liver and kidney leading to dual deficiency of qi and blood (
), (19) dual deficiency of liver and kidney leading to dual deficiency of qi and blood ( ,
, ), and (20) strain of extensor tendons pattern (
), and (20) strain of extensor tendons pattern ( ).
).
The (17) cold-dampness invading the inside pattern was presented together with the (1) wind-cold obstructing the collaterals pattern, (2) cold-dampness exterior attack pattern, and (3) wind-cold pattern as the generalized wind-cold-dampness pattern due to their similarity in the chosen terminology of the pattern name, pathophysiologies of the patterns, and a large number of overlapping symptoms between these patterns (Table 3).
By counting the number of appearances in textbooks, the top four patterns were found to be identical to the top four patterns identified through the journal articles search, namely: the wind-cold-dampness pattern (five textbooks), the dual deficiency of qi and blood pattern (four textbooks), the retained dampness-heat pattern (three textbooks), and the qi stagnation and blood stasis (two textbooks; Table 4).
Symptoms and signs associated with the patterns
Table 2 shows the signs and symptoms associated with the 13 included patterns found in the textbook review. Two of 13 patterns did not state clinical signs and symptoms other than elbow pain. A total of 30 local symptoms were reported for 10 patterns. Whenever the same pattern was identified in both the journal studies as well as the textbook review, local signs and symptoms associated with these patterns were very similar. For example, in both the journal as well as the textbook review, the following signs and symptoms for the (1) wind-cold obstructing the collaterals pattern were found: pain aggravated by exposure to cold, alleviated by the application of heat, and difficulty in flexion and extension of the forearm.
Five of the 13 patterns stated an additional 20 systemic symptoms. Many systemic symptoms in the textbook review were different from the ones found in the journal review (Table 2). For example, for the (5) dual deficiency of qi and blood pattern, in the journal review, systemic signs and symptoms found were a pale and lusterless face, a soft voice, muscle atrophy, and occasional numbness. The textbooks also stated a pale and lusterless face and a soft voice, but additionally mentioned shortness of breath, palpitations, insomnia, forgetfulness, tiredness, reduced appetite, and dizziness.
Nine of the 13 patterns reported a total of nine tongue features and eight pulse features. For the patterns identified by both the journal and the textbook review, the tongue and pulse presentations found were very similar or the same for most patterns; for example, the (4) retained dampness-heat pattern was associated with a thick, yellow tongue fur and a rapid, slippery pulse.
Unique signs and symptoms were found for nine patterns and were largely overlapping with the unique signs and symptoms identified in the journal review (Table 2). For example, redness and elevated temperature of the skin at the lateral epicondyle would be unique for the (4) retained dampness-heat pattern, while cramps in the hand and feet were only associated with the (13) dual deficiency of liver and kidney pattern, and a dark tongue body with red spots, a thick and white tongue fur, and a tight and fine pulse was indicative for the (18) cold-dampness leading to qi stagnation and blood stasis pattern.
Discussion
The aim of this study was to identify TCM patterns and symptoms commonly associated with LEP. To the best of the authors' knowledge, this is the first systematic review of TCM pattern differentiation for LEP and for musculoskeletal conditions in general. Out of 555 potentially relevant full-text citations and 465 textbooks reviewed, only eight studies (1.4%) and seven textbooks (1.5%) matching the inclusion criteria were found. The surprisingly low number of articles identified in the literature highlights the need for more studies on the use of TCM pattern differentiation for LEP and other musculoskeletal conditions because an important element of reporting clinical acupuncture trials is to provide a rationale for the treatment provided, and pattern differentiation is a necessary step to formulate an acupuncture treatment rationale. 26 Therefore, without a standardized system of pattern differentiation, the quality of any acupuncture study may be hampered.
No assessment of the methodological quality of the studies included was performed and neither was any meta-analysis because the aim of the study was directed at investigating TCM patterns associated with LEP rather than assessing the efficacy of the interventions. By combining the findings from the journal articles and the textbook review, a total of 20 patterns, 34 local signs and symptoms, 20 systemic signs and symptoms, 10 tongue features, and nine pulse features were identified in LEP pattern differentiation (Table 2).
The signs and symptoms of LEP patterns reflect the loss of homeostasis and the pathological changes associated with the individual TCM pattern. For example, a pale and lusterless facial complexion, which frequently appears with dual deficiency of qi and blood, may be associated with parasympathetic excitation, 27 and pain accompanied by redness, swelling, and heat as seen in the retained dampness-heat pattern are often associated with acute inflammation and sympathetic excitation. 28 Pattern differentiation could therefore be beneficial in developing new research directions for the pathogeneses as well as the treatment of different diseases. 29
The most frequently mentioned patterns identified in both the journal studies as well as the textbook reviews were: the wind-cold-dampness pattern, the qi stagnation and blood stasis pattern, the dual deficiency of qi and blood pattern, and the retained dampness-heat pattern. Of the reported subjects in the included studies, these four patterns cover >80% of all subjects. The textbooks 19,21,22,24,25 that listed these four patterns are standard TCM textbooks used in TCM universities in China and in the West, and may therefore be considered to represent an academic consensus. The fact that the findings from the journal articles review and the textbook review showed such similarities suggests that TCM physicians most commonly consider these four patterns in pattern differentiation of LEP as well.
However, it should be noted that meridian pattern differentiation, commonly used for musculoskeletal pain conditions, might also play an important role in LEP pattern differentiation. 20 While there were only two studies 11,13 and one textbook 20 that mentioned meridian pattern differentiation in the current review, there may be a much higher number of studies that used such method, as meridian pattern differentiation is often implicit in the method of acupoint selection in acupuncture studies. Interestingly, in the study of Deng and Lun, 11 meridian differentiation and other systems of differentiation were used together. The use of meridian pattern differentiation may help to guide the choice of acupoints (along the meridian) and the use of other systems (e.g., the eight-principle pattern differentiation and the qi-blood pattern differentiation) may guide other aspects of the treatment, such as needling technique and the choice of treatment modality (e.g., whether to use moxibustion). From this example, it can be seen that the use of pattern differentiation in TCM is to guide the choice of treatment modalities, and pattern differentiation may not be limited to a single system. The differentiation of LEP may use the meridian system in conjunction with the differentiation of one of the top four patterns, which were identified in this review. This highlights the flexibility and pragmatic approach of pattern differentiation in TCM, which gives Chinese medicine the ability to be a highly individualized medicine.
There were also unique features, which were made of distinct signs and symptoms, associated with a specific pattern. The unique features of the four most common patterns are as follows. LEP co-appearing with one or more of the following features would be indicative of the wind-cold-dampness pattern: a sensation of heaviness in the entire body, fatigued limbs, aversion to cold, loose stools, clear urine, and a tight and sunken pulse. For the dual deficiency of qi and blood pattern, it would be LEP conjointly with a pale, lusterless face, a soft voice, muscle atrophy, occasional numbness, shortness of breath, palpitation, insomnia, forgetfulness, tiredness, and a reduced appetite. The unique features of the qi stagnation and blood stasis pattern are LEP conjointly with knots palpable at local elbow area, rigidity and stiffness upon palpation, purplish discoloration of the skin at local elbow area, a cyanotic tongue body with red spots along the lateral sides, a white tongue fur or thin and yellow tongue fur, and a string-like pulse or a rough pulse. Finally, LEP conjointly with one or more of the following features would be indicative of the retained dampness-heat pattern: redness and heat of the joint, thirst without the desire to drink, a thick and yellow tongue fur, and a rapid and slippery pulse (Table 2: underlined signs and symptoms).
These identified unique features of a pattern are of highly clinical significance, as they help to simplify pattern differentiation in clinical practice. Indeed, it had already been pointed out 2000 years ago by the famous physician Zhang Zhong Jing that a pattern could be determined once the main symptoms were found, without the need for finding other (secondary) symptoms. 30 The identified unique features should therefore be included in the development of future instruments for pattern diagnosis.
They may also be explained bio-physiologically. For example, the unique features seen in the qi stagnation and blood stasis pattern have been linked to the accumulation of senescent red blood cells (RBCs). 31 This process leads to impaired deformability of RBCs and thrombosis, causing an increase in blood flow resistance, which may result in a string-like pulse or a rough pulse. 32 Local rigidity and stiffness upon palpation and a constant dragging pain at the lateral epicondyle may be caused by methemoglobin elevation along with thrombosis and vasoconstriction, 33,34 and a cyanotic tongue body with red spots on lateral sides and the purplish discoloration of the skin at local elbow area may also be a result of methemoglobinemia, all associated with accelerated RBC senescence. 35
Unique features seen in the dual deficiency of qi and blood pattern such as tiredness, muscle atrophy (emaciation), reduced appetite, and palpitations have been linked to hypoxia (as a result of anemia in most cases). 36 Hypoxia causes a disturbance of the circadian rhythms, which induces changes in the locomotive activity (tiredness, lassitude) as well as an abnormal cardiogram (palpitations). 37,38 Hypoxia has also been shown to trigger hypoxia-inducible factor 1 (HIF-1) expression that indirectly regulates food intake and energy expenditure resulting in reduced appetite and muscle atrophy (emaciation). 39 –44
On the other hand, heat (as in the retained dampness-heat pattern) and cold (as in the wind-cold-dampness pattern) patterns have been found to be associated with activation of distinct signal pathways, and specific biomarkers have been identified for these two patterns. 45,46 For example, in rheumatoid arthritis (RA), different genes and distinct signaling pathways were activated in subjects belonging to either cold or hot pattern groups. 47,48 Also, heat and cold patterns in RA patients were found to be associated with different levels of C-reactive protein expression. 49,50 Key signs and symptoms of the wind-cold-dampness pattern and retained dampness-heat pattern could be explained by the regulative processes of the nervous system. 51 For the heat pattern, local signs of redness and increased joint temperature have been attributed to enhanced microcirculation and capillary perfusion; a rapid and slippery pulse as well as thirst and a dry mouth may be due to a volume shift of fluids in the direction of the peripheral tissues and a relative lack of fluid in the in the larger central vasculature, leading to sympathetic excitation and a higher heart rate, together with activation of water-intake regulatory responses. 52 On the other hand, in the cold pattern, the sensation of coldness and aversion to cold as well as stiffness and fatigued limbs may be associated with reduced microcirculation and decreased capillary perfusion, resulting in a lack of oxygen and nutrient supplies and loss of muscular strength. 53
It is not clear why LEP is typically associated with the four most common TCM patterns, as identified by this study. However, the Western medicine etiology for LEP itself is also unclear. 54,55 It is probable that factors causing specific TCM patterns predispose the patient to LEP. 56 In this regard, it is worth noting that LEP is characterized as either a tendinitis, or a tendinosis, or both. 57,58 It would be interesting to determine if Western medicine pathophysiological changes seen in certain TCM patterns are more likely to be associated with tendinitis or tendinosis, respectively. For example, the retained dampness-heat pattern may be more consistent with tendinitis, whereas the wind-cold-dampness pattern and the dual deficiency of qi and blood pattern may be more linked to tendinosis, and the qi stagnation and blood stasis pattern may involve both tendinitis and tendinosis. Further research is certainly warranted to test the above hypotheses.
During this analysis, it was found that several terminologies were chosen to describe the same or extremely similar set of symptoms or pathogeneses, and they were grouped together for simplicity (Table 2: generalized patterns are on the very right side of the table). A similar approach has been taken in previous reviews of TCM patterns. 59,60 It was also found that different sources mentioned different clinical features of the same patterns, in which case all features for one pattern were listed. Grouping similar patterns for LEP together under a generalized pattern name, as well as grouping different clinical features from several sources under the same pattern, realizes the first step toward the standardization of terminology for pattern differentiation in LEP. However, further studies are necessary to assess the validity of these patterns and their features.
Several approaches have been taken in the process of validating and standardizing TCM patterns, but general agreements have not yet been reached. One approach is the use of biological markers, which can provide an objective basis for different patterns. 10,61,62 Another approach is to perform data mining of data from clinical trials or epidemiological surveys, which allow the identification of patterns (or syndromes) using factor analysis, cluster analysis, or latent tree models. 63 –66 The Delphi method has also been used in recent studies to find consensus on standardized TCM treatment principles, which were based on TCM pattern differentiation, so it could also be used for the standardization of TCM patterns. 67,68 However, all the above approaches should be guided by the existing practice of pattern differentiation, which is best established through a systematic review such as this one. In other words, the results from this review will provide a basis for further studies of TCM patterns in LEP. Data mining for TCM pattern differentiation of LEP was performed in this study, but no meaningful results were obtained. Thus, the details of the data mining are not presented in this article. The identified LEP patterns will be further validated using a Delphi method. As LEP shares many of the pathogeneses found in other musculoskeletal diseases, these approaches may also be useful for the study of pattern diagnosis for other musculoskeletal diseases. 69
The major drawbacks of TCM diagnoses are the absence of a standard in terminology, as well as poor diagnostic and inter-rater reliability. 9,70 –76 Poor diagnostic reliability can be commonly traced to information variance as well as criterion variance. 77 The current TCM diagnostic system is exposed to these variabilities because different practitioners/researchers collect different sets of information (information variance), as well as use different diagnostic criteria (criterion variance) in order to arrive at a specific pattern diagnosis. In this review, these variabilities were also found. For example, a variety of very similar terms that referred to same underlying LEP pattern, for example the (7) qi stagnation and blood stasis pattern and the (8) qi and blood stasis pattern, both referred to qi stagnation and blood stasis pattern. It was also found that many similar terms were used to describe fundamentally the same symptoms, for example “sensitive to pressure,” “tenderness,” “tender upon pressure,” and “dislikes pressure,” all denoting local tenderness.
One way to reduce information variance is to develop standardized instruments, which collect similar sets of information using standardized terminology. Unison diagnostic criteria could also improve diagnostic, as well as inter-rater reliability and intra-rater reproducibility, thus reducing criterion variance. This would help to overcome some of the shortcomings in TCM research and practice. 78
There are certain methodological strengths and limitations of this study. This review is rather comprehensive, as an exhaustive search of journals and textbooks was included, which augments the generalizability of the findings. A limitation was that literature from other foreign language sources was not included. Another limitation was the lack of diagnostic criteria in some of the included studies, and the inconsistency of the diagnostic criteria provided for LEP in the textbooks. 12,14,17 Thus, this review is not able to provide an in-depth review of the diagnostic criteria used for LEP in previous TCM literature. Finally, pattern differentiation for LEP has only been found in a small number of studies and textbooks, thus veiling the rationale for treatment choices for the majority of literature that has been reviewed in uncertainty. Nevertheless, it is important to note that in a recent study, complete agreement was found in the four most commonly seen patterns of LEP between this literature review and expert consensus on clinical practice. 79
Conclusions
This review found that consistent methods of pattern differentiation exist for LEP in the TCM literature. The major patterns of LEP—the wind-cold-dampness pattern, the dual deficiency of qi and blood pattern, the retained dampness-heat pattern, and the qi stagnation and blood stasis pattern—are characterized by certain unique symptoms and signs, which constitute their unique features. These unique features with distinct bio-physiological correlations may hold the key to understanding TCM individualized treatment based on pattern differentiation. The findings of this study as well as the approach to identifying patterns and their unique features may be useful for studying TCM treatment of LEP and other musculoskeletal disorders in general.
Footnotes
Acknowledgments
M.G. was supported by the UGC's Hong Kong PhD fellowship scheme 2013/14 (PF12-16701). This study was partially supported by HKBU faculty research grants to S.P.Z. (FRG1/14-15/056).
Author Disclosure Statement
The authors declare that they have no competing interests. No competing financial or non-financial interests from the funders exist.