
Abstract
Background:
A recent study showed that Gynura pseudochina DC. var. hispida Thv. leaf extract (GP) can reduce the activation of the nuclear factor κB (NF-κB) pathway and suppress the release of interleukin (IL)-1β, IL-6, and tumor necrosis factor -α, which play an important role in the pathogenesis of psoriasis.
Methods:
Twenty-five patients with mild to moderate plaque psoriasis completed a 4-week trial. Twice daily, they applied the GP ointment on psoriatic lesions on one side of the body, and they applied 0.1% triamcinolone (TA) cream on the other side. The Targeted Area Score (TAS), Psoriasis Severity Index (PSI) scores, and Physician's Global Assessment (PGA) scores were assessed at baseline and at weeks 1, 2, 3, and 4. Pre- and post-treatment skin samples were taken. Phosphorylation of NF-κB p65, Ki-67, and epidermal thickness were analyzed through immunohistochemistry.
Results:
The TAS for erythema, scaling, and induration and PSI scores decreased on both treated sides. A statistically significant difference was observed beginning at the first week of treatment. The GP ointment significantly decreased scaling scores. However, no significant differences were observed between the TAS for erythema and induration or the PSI and PGA scores. Immunohistochemical staining revealed diminution of phosphorylated NF-κB p65, Ki-67, and epidermal thickness in the lesions treated with the GP ointment. The ointment was well tolerated, with minimal side effects. No laboratory abnormalities were detected.
Conclusions:
The GP ointment demonstrated efficacy similar to that of 0.1% TA cream for mild to moderate chronic plaque psoriasis. In addition, its short-term side effects were minimal.
Introduction
P
Many cytokines, chemokines, and immune cells play a role in the initiation and maintenance phases of psoriasis. 3 Among these factors, the nuclear factor κB (NF-κB) signalling pathway plays an important role. 4 There is evidence that upregulation of active NF-κB is detected in psoriatic lesions, and its presence is diminished as the lesions resolve. In contrast, active NF-κB is not present in normal skin cells. 5
Gynura pseudochina DC. var. hispida Thv., a medicinal plant, is grown in many tropical regions, including Southeast Asia and Africa. Its leaves, rhizome, and roots have long been used as traditional medication against several conditions, such as herpes zoster infection, abscesses, and thermal burn. 6,7 A recent study has demonstrated that the methanol extract from its leaves exhibits an in vitro NF-κB inhibitory effect 8,9 as well as anti-inflammatory effects on human monocytes. 9
On the basis of this previous supporting evidence, the current study investigated the efficacy of G. pseudochina DC. var. hispida Thv. leaf extract (GP) ointment in patients with mild to moderate chronic plaque psoriasis, as well as its safety profile and a possible in vivo mechanism of action.
Materials and Methods
This randomized controlled study was approved by the institutional review board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. The data were collected at King Chulalongkorn Memorial Hospital from March to August 2013. The inclusion criteria included patients 18–80 years of age who had mild to moderate chronic plaque psoriasis with lesions that were distributed equally on both sides of the body and who had been stable for at least 8 weeks. Patients who had received any topical treatments or phototherapy within the 2 weeks before the study period, systemic treatments within the past 4 weeks, or biologic agents within the 6 months before the study period were excluded. Pregnant and lactating women, patients with immunodeficiency diseases or those currently taking immunosuppressive drugs, patients with abnormal liver and/or kidney functions (aspartate aminotransferase, alanine aminotransferase, and alkaline phosphatase) more than three times the normal limits and/or serum creatinine levels greater than 2 mg/dL and patients with an allergy to G. pseudochina DC. var. hispida Thv. were also excluded.
Psoriatic lesions from each side of the body were block-randomized to receive GP ointment or 0.1% triamcinolone (TA) cream (an in-house formulation, King Chulalongkorn Memorial Hospital). Both medications were filled in containers designated as right or left. The patients were instructed to apply each topical medication on the allocated side twice daily for 4 weeks. To avoid cross-contamination, the patients were advised to wash their hands thoroughly before rubbing in the topical treatments. Other topical therapies were prohibited during the study period.
The patients were evaluated at baseline and every week for 4 consecutive weeks. At each visit, a clinical examination of both treated sides was performed by an experienced dermatologist to obtain the Targeted Area Score (TAS) and Psoriasis Severity Index (PSI) scores. Digital photographs of the lesions were taken by using a standard digital camera (DSLR D90, Nikon, Tokyo, Japan). To obtain the Physician's Global Assessment (PGA) scores, a blinded analysis of the photographs was performed by three dermatologists. In addition, the patients were interviewed to obtain the Self-Assessment Score (SAS). Complete blood counts and liver function tests were performed, and blood urea nitrogen and creatinine levels were measured at baseline and at the end of the study. Any treatment side effects were recorded, along with their durations and severities.
Outcome measurements
The TAS consisted of an individual assessment of erythema, scaling, and induration. The scores ranged from 0 to 4 for each aspect. The summation of all 3 TAS aspects, termed the Psoriasis Severity Index (PSI) or modified Psoriasis Area and Severity Index score, ranged from 0 to 12. 10,11 The PGA score used a 6-point ordinal rating that was based on comparing the treated lesion with the baseline. 12 Finally, the SAS was obtained by interviewing the patients to evaluate their responses to their treatments. 12
Histologic analysis
Punch biopsy specimens from psoriasis plaques treated with the GP ointment were obtained at baseline (week 0) and post-treatment (week 4) from two patients. The skin samples were fixed in 10% formalin and embedded in paraffin. The sections were cut and stained with hematoxylin and eosin. Additionally, immunohistochemistry was performed for NF-κB p65 and Ki-67. For NF-κB p65, Ventana Benchmark XT (Ventana, Tucson, AZ), an automated slide staining system, was used. Antigen retrieval was achieved with a mild CC1 protocol, and rabbit polyclonal anti–NF-kB p65 (Abcam, Cambridge, MA) was used at a dilution of 1:800. For detection, an ultraView Universal DAB Detection Kit (Ventana) was used. Staining with monoclonal mouse anti-human Ki-67 (Dako, Glostrup, Denmark) was performed with Autostainer Link 48 (Dako). For visualization, EnVision FLEX, High pH (Dako) was used. Three to four sections from the patients at each time point were cut, stained, and analyzed.
The percentage of positive nuclear staining with anti–NF-κB p65 and Ki-67 in the epidermis was obtained by using Aperio ImageScope software, version 11 (Leica Biosystems, Nussloch, Germany). In brief, each slide was scanned using an Aperio Scanscope CS (Leica Biosystems). The area across the whole epidermis (except the stratum corneum) was analyzed, and the percentage of positive nuclear staining cells was determined by using a nuclear analysis algorithm. The epidermal thickness in the hematoxylin and eosin sections was evaluated by a certified dermatopathologist (J.W.) by measuring three × 40 fields in each section, and the mean value was calculated for each patient.
G. pseudochina DC. var. hispida Thv. leaf extract ointment and 0.1% triamcinolone cream preparation
G. pseudochina DC. var. hispida Thv. (Asteraceae) leaves were harvested. The dry powdered leaves were extracted through maceration in 95% ethanol, and the extract was dried by using a rotary evaporator to obtain the green thickening mass (yield: 17.8% wt/wt). An ointment was prepared from a mixture of the extract and vehicle (1:10). The vehicle consisted of white beeswax, white soft paraffin, wool fat, dimethicone, isopropyl myristate, and ethanol at a ratio of 1.9:4:0.5:0.6:1:1. The 0.1% triamcinolone cream comprised 0.1% of triamcinolone acetonide in vehicle containing cetyl alcohol, stearic acid, glycerol monostearate, mineral oil, propylene glycol, carbomer, methylparaben, propylparaben, polysorbate 80, and water.
Statistical analysis
All statistical analyses were performed by using SPSS software, version 17 (IBM Inc., Armonk, NY). The outcome measurements, including the TAS, PSI scores, PGA scores, and SAS, were analyzed by using the Wilcoxon signed-rank test. Values were considered statistically significant with p < 0.05. A sample size of 25 was determined to provide 90% power to detect a difference between the treatment groups at an α of 0.05.
Results
Twenty-five patients (13 men and 12 women; mean age, 48.6 ± 14 years) completed the study. There were no dropouts. The baseline characteristics of the patients are shown in Table 1.
SD, standard deviation; PASI, Psoriasis Area and Severity Index; MTX, methotrexate; NB-UVB, narrow-band ultraviolet-B phototherapy.
There were no between-group differences in the initial mean TAS for erythema, scaling, induration, and PSI (1.96 ± 0.45, 1.64 ± 0.70, 1.68 ± 0.48, and 5.28 ± 1.10 in the GP ointment group versus 1.96 ± 0.45, 1.64 ± 0.70, 1.68 ± 0.48, and 5.28 ± 1.06 in the TA cream group, respectively). After treatment, the mean TAS and PSI scores decreased on both sides. A statistically significant improvement was observed in both groups starting at the first week of treatments. At week 4, the mean TAS and PSI scores were greatly reduced to 1.08 ± 0.57, 0.44 ± 0.58, 0.68 ± 0.48, and 2.2 ± 1.08 on the GP ointment side versus 1.12 ± 0.44, 0.80 ± 0.71, 0.76 ± 0.52, and 2.68 ± 1.44 on the TA cream side (Fig. 1).
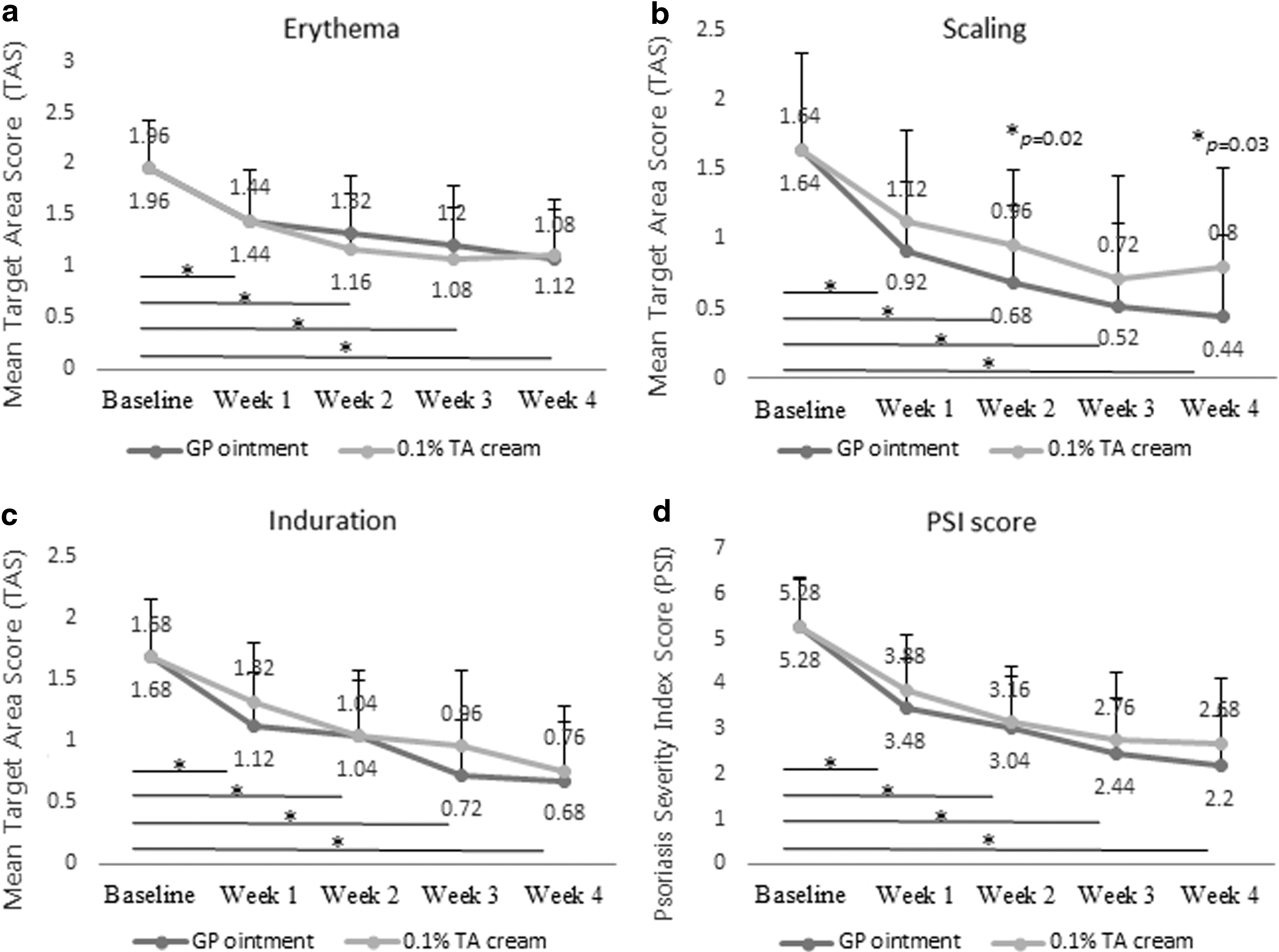
Targeted Area Score (TAS) and Psoriasis Severity Index (PSI) scores.
When the two treatments were compared, the GP ointment significantly decreased the scaling scores at week 2 (0.68 ± 0.56 versus 0.96 ± 0.54 for GP ointment versus TA cream, respectively;, p = 0.02) and week 4 of the therapy (0.44 ± 0.58 vs. 0.80 ± 0.71, respectively; p = 0.03) (Fig. 1b). However, there were no significant between-group differences in erythema and induration. Although a greater reduction in the mean PSI scores was achieved with the GP ointment, this difference was not statistically significant (Fig. 1d).
The results of the PGA score aligned with the TAS and PSI scores. The PGA scores in both groups showed improvement compared with the first treatment week. At week 4, 72% of the lesions treated with the GP ointment demonstrated at least moderate improvement (50% improvement) compared with 60% of those treated with the 0.1% TA cream (Fig. 2a). There were no significant (p = 0.375) between-group differences in the PGA scores. However, the SASs were statistically significantly higher in the group treated with the GP ointment (p = 0.034) (Fig. 2b).
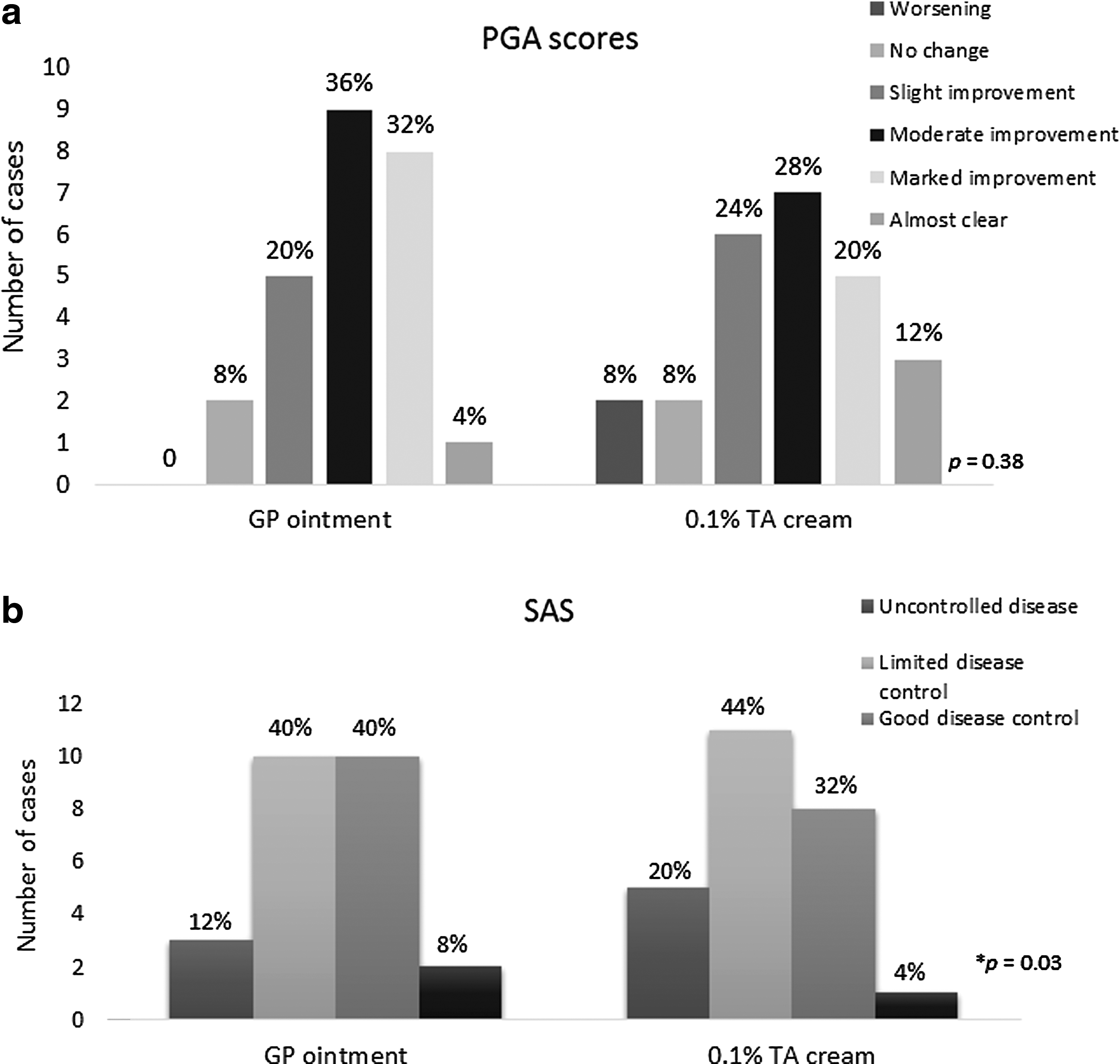
The Physician's Global Assessment (PGA) scores and Self-Assessment Score (SAS).
Clinical photographs of the psoriatic lesions treated with GP ointment and 0.1% TA cream are shown in Figure 3.

Psoriatic lesions on breasts.
Histologic analysis of the lesions treated with the GP ointment was performed by using a total of 15 skin sections from two patients. Before the treatment, 81.82% ± 5.77% of the cells in the epidermis exhibited positive nuclear staining with anti–NF-κB p65. Intriguingly, after the treatment, the percentage was reduced to 72.58% ± 3.87%. In alignment with the anti–NF-κB p65 results, staining with Ki-67 (which signified cell proliferation) was also reduced (from 52.91% ± 5.41% at baseline to 20.93% ± 14.66% at week 4). Epidermal thickness also decreased, with a mean reduction of 42.69% ± 31.07% from baseline. The immunohistochemistry staining results are shown in Figure 4.
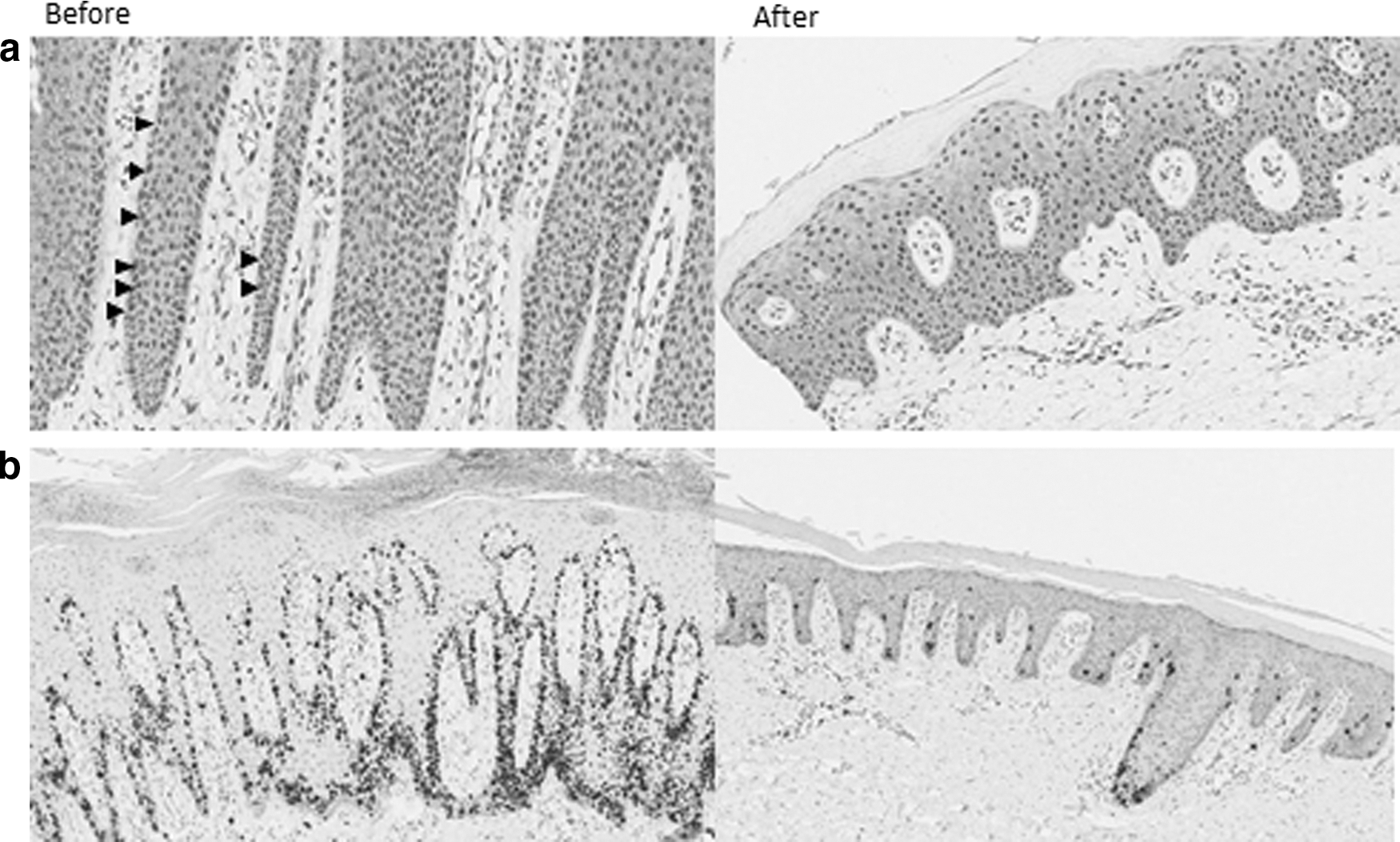
Immunohistochemistry study of the skin specimens at baseline and 4 weeks after treatment with GP ointment.
Safety
The side effects from both treatments are detailed in Table 2. The most common adverse event (i.e., found in 96% of the lesions treated with the GP ointment) was yellowish staining. This effect was temporary and could be washed off with water. Other side effects included a mild stinging sensation lasting less than 30 minutes and itch. Twelve percent of the lesions treated with 0.1% TA cream exhibited hypopigmentation in the treated area.
GP, Gynura pseudochina DC. var. hispida Thv. leaf extract; TA, 0.1% triamcinolone.
Laboratory investigations revealed no abnormalities in any patients before and after treatment.
Discussion
Gynura pseudochina DC. var. hispida Thv. has long been used in traditional medicine in Southeast Asian countries. However, no studies have proven its efficacy, and its mechanism of action is still unknown. Recently, using spectroscopic and mass spectrometric methods, Siriwatanametanon et al. have identified four compounds in the methanol extract from the leaves of G. pseudochina var. hispida. These compounds demonstrated an in vitro NF-κB inhibitory effect 8,9 as well as inhibition of the release of interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF)-α from cultured human monocytes. 9
NF-κB is a transcription factor that plays an essential role in psoriasis, as it orchestrates innate and adaptive immunity, as well as the cell cycle underlying the pathogenesis of the disease. Members of innate immune systems, namely toll-like receptor 2 and caspase-5, largely depend on NF-κB pathway to initiate proinflammatory cytokines. 13,14 Additionally, there are many cytokines in the TH-1 and TH-17/interleukin (IL)-23 pathways, and chemokines CCL20, CCL27, and IL-8, which are important in recruiting dendritic cells, TH-17 cells, and neutrophils in the skin, are produced through NF-κB activation. 15 –18 Furthermore, NF-κB is also responsible for the antiapoptotic activity of keratinocytes by controlling apoptosis inhibitors, such as Bcl-XL and survivin. 19,20 Currently, several psoriasis medications that target this signalling pathway are being developed. 3,15
NF-κB is composed of members that include p50, p52, p65 (RelA), c-Rel, and RelB. 4 The most abundant form is a heterodimer of a p50 or p52 subunit and p65. 18 During the resting stage, NF-κB is sequestered in the cytoplasm with inhibitors of κB. When an activation takes place, phosphorylation of inhibitors of κB results in the release of NF-κB and its translocation into the nucleus, where proinflammatory gene transcription is induced. 15 Through immunohistochemistry with anti–NF-κB p65, we could demonstrate the nuclear expression of NF-κB in psoriasis skin lesions. The results align with previous reports and confirm the importance of this transcription factor family in the pathogenesis of psoriasis. 5,20 Interestingly, after a month-long treatment with GP ointment, the nuclear expression of NF-κB p65 was reduced.
In addition to inhibiting the NF-κB pathway, G. pseudochina var. hispida leaf extract has been reported to suppress the release of IL-1β, IL-6, and TNF-α. These proinflammatory cytokines play important roles in the development and maintenance of psoriasis. 3,21 TNF-α is increased in the skin lesions and sera of patients with psoriasis, and its level correlated with the disease severity. 22,23 IL-1β and IL-6 are mandatory for the differentiation of Th17 cells and for the augmentation of the IL-23/IL-17A/IL-22 axis. 24 –26 Both of these mechanisms may explain the clinical improvement observed with the use of GP ointment. However, additional detailed studies are needed to clarify the exact mechanism of actions.
This study demonstrated similar efficacy between the GP ointment and the 0.1% TA cream, a class 4 mid-strength topical corticosteroid that is commonly used for chronic plaque psoriasis, 27 particularly in Thailand. Furthermore, the GP ointment demonstrated superiority in improving desquamation, which might lead to higher patient satisfaction scores because scaling is easily noticeable by patients.
Concerning the safety of G. pseudochina, the plant contains pyrrolizidine alkaloids, which may have a risk for hepatotoxicity; 8 therefore, it seems more appropriate to use topical treatment to minimize systemic adverse events. In this study, laboratory investigations, including liver function tests, did not show any abnormalities. In addition, the observed side effects consisted solely of local adverse events, which were mild and transient.
This study was conducted to assess the potential clinical benefits and safety of GP ointment in an effort to provide evidence-based support for this traditional herbal medicine. This randomized controlled trial used left-to-right comparisons with the same patients; thus, many confounding factors were eliminated. However, the study limitations include insufficient blinding for the evaluators and patients because the herbal ointment bears a characteristic yellow color, which makes it challenging to conduct a double-blinded clinical trial. In addition, the number of participants was small, and the follow-up time was relatively short. Only a limited number of skin specimens could be obtained for the histologic examinations because of ethical considerations. Finally, the difference in the vehicles used in the topical medications may have affected the results. It is important to note that GP ointment contains beeswax and wool lanolin, both of which are known to have beneficial effects, including anti-inflammation and serving as an effective moisturizer on the skin. 28 However, the inhibitory effect of lanolin and beeswax on NF-κB pathway has never been reported. A further research using a similar base between the two groups will minimize this problem and confirm the efficacy of G. pseudochina var. Hispida extract.
In summary, GP ointment can improve psoriasis lesions, similarly to 0.1% TA cream, with minimal short-term side effects. Further in vitro and in vivo investigations into the mechanisms of action as well as larger cohort studies with long-term follow-ups are warranted to support the potential use of GP ointment as a treatment for psoriasis.
Footnotes
Acknowledgments
Funding for this work was provided by the Cerebos Awards, a nonprofit research fund. The authors gratefully thank the Special Task Force for Activating Research (STAR), Chulalongkorn University, for their support.
Author Disclosure Statement
No competing financial interests exist.