
Abstract
Objectives:
To observe the effects of transcutaneous electrical acupoint stimulation (TEAS) in improving motor functions and self-care abilities in children with cerebral palsy in their early childhood.
Design:
A preliminary, prospective, cohort study.
Settings/Location:
Multicenter.
Subjects:
Children aged 2–6 years old.
Interventions:
Twenty-three children were included in the study and randomly assigned to a control group ([CG] N = 11) or a therapeutic group ([TG] N = 12). In the TG, children were treated with TEAS (Shousanli [LI10] and Waiguan [SJ5]) plus the exercise therapy, while in the control group, they were treated with sham TEAS plus exercise therapy. Therapies were performed five days per week for eight weeks.
Outcome measures:
The Gross Motor Function Measure (GMFM) and the Functional Independent Measurement for children (WeeFIM) were used to evaluate motor functions and self-care abilities before and after the therapies.
Results:
Greater improvements were observed in the TG concerning all the measurements, although without statistical differences. The increments of the GMFM score and the WeeFIM motor, self-care and total scores were 36.08 ± 18.34 (26%), 16.17 ± 8.21 (33%), 7.67 ± 3.42 (40%) and 20.33 ± 10.08 (28%) in the TG, while 22.73 ± 16.54 (17%), 9.09 ± 9.43 (19%), 5.64 ± 6.73 (29%) and 12.82 ± 11.77 (18%) in the CG, respectively. No statistically significant correlations were shown between functional improvements and the demographics in the TG or the CG. The GMFM improvement was not statistically correlated with the improvements of the WeeFIM motor, self-care or total scores. However, the WeeFIM motor, self-care and total score were significantly positively correlated with one another in both groups (P < 0.01). No adverse effect was recorded during the study.
Conclusion:
TEAS may be effective in improving motor functions and self-care abilities in children with cerebral palsy, in addition to conventional exercise therapy. Larger samples are required to confirm the efficacies.
Introduction
C
Transcutaneous electrical nerve stimulation (TENS) provokes the nerve or the muscle over skin through electrical currents generated by a portable device. It may or may not cause muscle contraction depending on the pulse frequency and intensity, generating various therapeutic effects. 7 It was effective in treating various medical conditions, for example, pain, paralysis, even gastroparesis and wound healing in previous studies. 8 –11 The development of transcutaneous electrical acupoint stimulation (TEAS) was based on the application of TENS combined with the Chinese traditional acupuncture theory. Acupuncture points are believed to possess special electrical properties with increased conductance, reduced resistance, and elevated electrical potential. 12 By performing TENS on the acupuncture points, acupuncture-like effects could be elicited. The de qi sensation is considered to be the hallmark of successful needling. 13 TEAS was able to generate the sensation of acupuncture, de qi, thus validly mimicking the effects of acupuncture. 14 Benefits of acupuncture have been reported in treating CP. 15 One study showed the effects of acupuncture at Taichong (Liv3) in spastic CP using functional magnetic resonance imaging (fMRI), with the evidence of acupuncture-lead changes of activation in the brain, for which the author postulated it was resulted from blockage of the liver meridian. 16 Researchers revealed that acupuncture activated multiple signaling pathways to restore the brain functions. 17 Some experts also suggested that the effectiveness of acupuncture was resulted from adjusting the balance in the autonomic nervous system. 18
TEAS is a noninvasive approach, making it a novel alternative for acupuncture. It has been used in treating asthma and chronic obstructive pulmonary disease, relieving pain, enhancing muscle force, and improving motor functions after stroke. 19 –21 A recent study revealed that TEAS was safe and effective in ameliorating spasticity after brain injury. 21 Concerning its application in children, one study adopted TEAS in treating children with autism and found it effective in those who showed passive and aloof behaviors. 22 Currently, limited evidence was found for the effectiveness of TEAS in CP. Because of its beneficial effects on improving motor functions plus its noninvasive feature, TEAS could be a potential modality for children with CP. Earlier interventions yield better outcome because of better spasticity control and brain development. 1 Therefore, the study aimed preliminarily at observing whether TEAS was effective in improving motor functions and self-care abilities in children with CP in their early childhood.
Materials and Methods
Participants
The study was a preliminary, prospective, cohort study. All subjects met the diagnostic criteria for CP made by the National Conference of Cerebral Palsy in 2004. 23,24 The diagnostic criteria include (1) functional impairments only caused by nonprogressive and noncontagious brain lesions, confirmed with the imaging study of the brain; (2) symptoms, such as hemiplegia, triplegia, or tetraplegia, presented since infancy. The inclusion criteria of this study were (1) meeting the mentioned diagnostic criteria of CP and being classified into the spastic subtype; (2) presenting with motor disability with Modified Ashworth Scale (MAS) ≥Grade 1 in the wrist; (3) aged between 2 and 6 years old; (4) no other muscular skeletal disorders that could affect motor functions (e.g., hereditary muscular atrophy); (5) able to follow the instructions; and (6) signing the consent form. Finally, 23 patients were enrolled from five healthcare facilities in Shanghai (Huashan Hospital, Huashan Hospital Yonghe Branch, Shanghai Children's Hospital, Baoshan Community Health Center, Shanghai Yangguang Rehabilitation Center) between September 1, 2012, and March 1, 2013. They were assigned to either a therapeutic group (TG) receiving routine exercise therapy plus TEAS (N = 12) or a control group (CG) receiving routine exercise therapy plus sham TEAS (N = 11). At the inclusion visit, rehabilitation physicians documented the demographic data of gender, age, level of the Gross Motor Function Classification System (GMFCS), level of the Manual Ability Classification System (MACS), level of the Communication Function Classification System (CFCS) level, type of paralysis, and the MAS grade. Adverse effects were documented in both groups during the study.
If one of the following criteria was met, the patient, who (1) skipped the treatment for consecutive 3 or 4 days in a week; (2) was using other electrical stimulation therapy; (3) received intramuscular injections of botulinum toxin; (4) used antispasticity drugs (e.g., baclofen) or drugs that may induce spasticity (e.g., metoclopramide), would be regarded as violation and be excluded from the study.
The consent form was signed by a legal guardian of the child under free will. Approval was obtained from the ethical committee of Huashan Hospital. The study has been registered in the Chinese Clinical Trial Registry (ChiCTR-TRC-12002336).
Exercise therapy
The individualized therapeutic exercise was provided to all children included in the study. The exercise therapy was customized based on age and functional deficits of each child. Aiming at improving the functions of the upper extremities and the abilities of ADLs, the therapy included passive and active movement of the limbs, programs for improving muscle strength and the function of hands in daily activities (e.g., grasping small glass beads, moving cups from one place to another, pushing against the wall, flapping hands, and lifting up the arm). Bobath and Vojta maneuvers were also used based on the neural developmental order of the children. Experienced PTs and OTs performed the exercise therapy that lasted for 40 min per day, 5 days per week for 8 weeks.
TEAS therapy
Two acupuncture points were selected as the target acupoints: Shousanli (LI10) and Waiguan (SJ5). According to the theory of Traditional Chinese Medicine, Shousanli (LI10) is an acupuncture point on the large intestine meridian, which is considered to be effective in clearing the meridian and promoting motor functions. It is located at 2 cun (6.7 cm) below the lateral end of the transverse cubital crease when the elbow is flexed and the forearm is pronated. Waiguan (SJ5) is an acupuncture point on the triple heater meridian, which is considered to be effective in treating motor impairment in upper extremities. It is located at 2 cun (6.7 cm) above the transverse wrist crease on the dorsal surface of the forearm, between the radius and the ulna. The children in the TG were given TEAS therapy on one affected upper limb, with the anode being placed on Waiguan (SJ5) and the cathode being placed on Shousanli (LI10) (Fig. 1). In the CG, the electrodes were placed in the same sites as those in the TG. The device was kept open; however, the current was set at 0 mA throughout the treatment.

The dual channel portable TENS device and the placement of electrodes when TEAS was applied. The anode was placed on Waiguan (SJ5) and the cathode was placed on Shousanli (LI10). TEAS, transcutaneous electrical acupoint stimulation; TENS, transcutaneous electrical nerve stimulation.
A dual channel portable TENS device (MyoNet AOW; Shanghai NCC Medical Co., Ltd, China) is used in the study. The pulse frequency was set to 2 Hz and the pulse width was set to 200 μs as previously suggested. 25,26 Each pulse cycle consisted of 2-sec rise time, then 5-sec work time, then 2-sec fall time, and 10-sec rest time. The current was increased to an individual's maximum tolerated level, most likely between 12 and 18 mA, causing no reported discomfort. The TEAS was performed 20 min per day, 5 days per week, and lasted for 8 weeks.
Functional measurements
The Gross Motor Function Measurement-88 (GMFM-88) was used to evaluate children's ability to perform gross motor functions. The GMFM-88 consists of 88 items with 5 dimensions: supine/rolling (51 points), sitting (60 points), crawling/kneeling (42 points), standing (39 points), and walking/running/jumping (72 points). Each item was 0, 1, 2, and 3 points based on the performance. Higher scores indicate better performance.
The Functional Independent Measurement for Children (WeeFIM) was used to evaluate children's performance on daily activities. 27 The WeeFIM is an internationally useful instrument to evaluate disability in children aged 6 months to 7 years. 28 It contains a motor function domain (13 items) and a cognitive function domain (5 items). The self-care is a subdomain under motor function domain, consisting of six items, which are (1) eating, (2) grooming, (3) bathing, (4) dressing (upper limb), (5) dressing (lower limb), and (6) toileting. Each item was scored 1–7 points based on the performance. Higher scores indicate better performance. The maximum score of the WeeFIM is 126 points, including motor function domain 91 points and cognitive function domain 35 points. One study suggested that self-care, motor, and cognitive domains could be treated as separate scales in children with spastic CP. 27 Therefore, the WeeFIM (self-care) was adopted as a measurement of motor function and self-care ability independently.
All the evaluations were recorded by qualified assessors at enrollment and at the end of the 8th week. All the assessors from different hospitals were trained to maintain consistency in evaluation. The assessors were not aware of the group division and did not involve in any medical care for the children.
Statistical analysis
The data were analyzed using SPSS 20.0 (PASW; IBM, Armonk, NY). For measurement data, Kolmogorove–Smirnov test was performed for normality and Levene's test for homogeneity of the variances. When normal distribution and equal variances assumed, independent t-test was used, otherwise, Mann–Whitney test was used to compare the differences between groups. Fisher's exact tests were used to test statistical differences of the gender, type of paralysis, GMFCS level, MACS level, CSCF level, and MAS grade between groups. The correlations between functional improvements and the demographics within a group and the correlations between functional improvements within a group were obtained with a two-tailed Spearman correlation analysis. The level of statistical significance was set at p < 0.05.
Results
Demographics
The demographics of all cases in the study are presented in Table 1. The average age, gender, GMFCS level, MACS level, CFCS level, and types of paralysis were not statistically different between groups (p > 0.05). p Value was 0.049 in MAS grades between groups, possibly due to uneven distribution of the number of cases in each level in the TG. The study flow is presented in Figure 2.
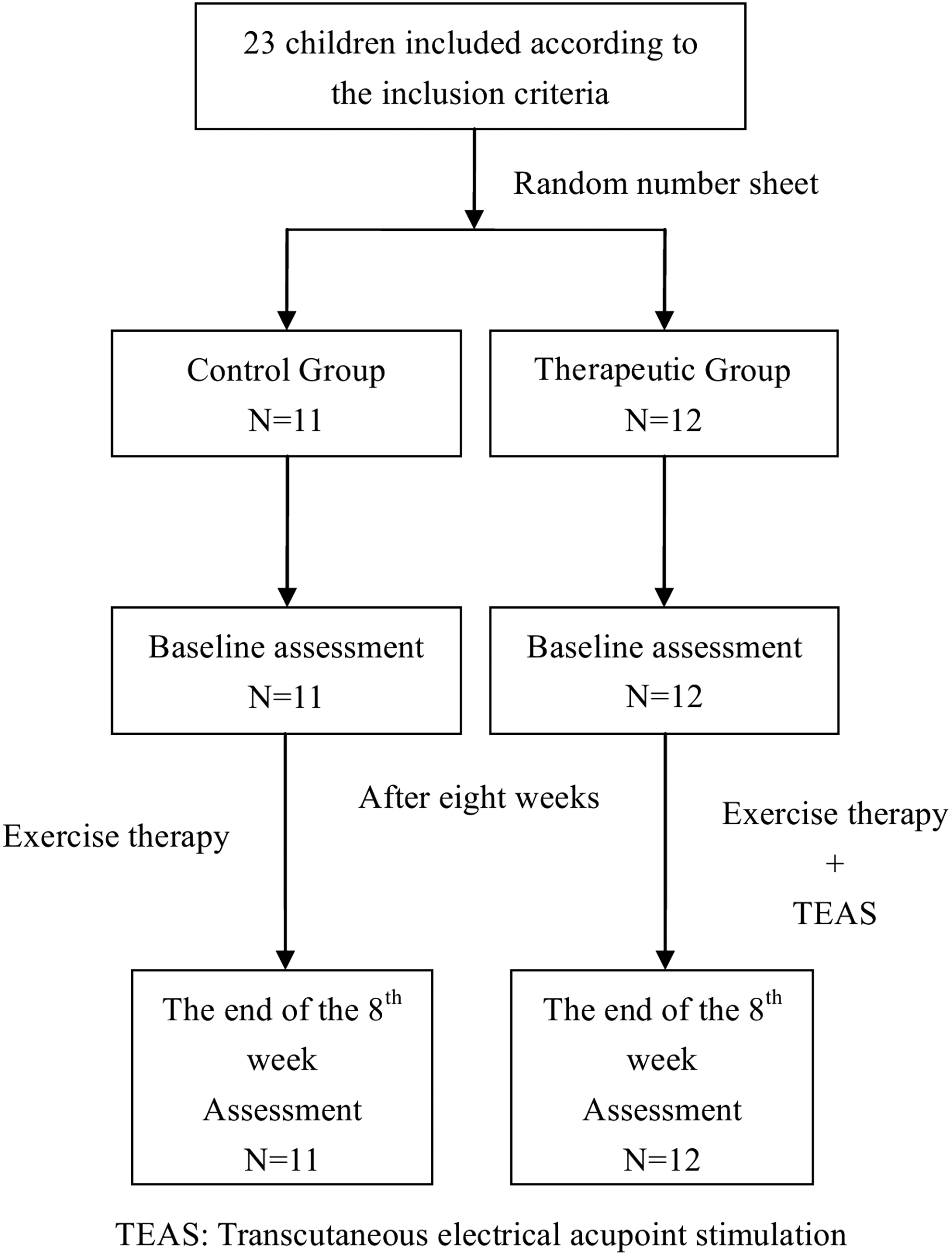
The study flow.
The distribution is statistically different at the 0.05 level (two-tailed).
CG, control group; GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification System; MAS, Modified Ashworth Scale; TG, therapeutic group; CSCF, Communication Function Classification System.
Comparisons of GMFM and WeeFIM scores between groups
The scores of GMFM and WeeFIM are presented in Table 2. No statistical significance was found between groups before and after the therapies (p > 0.05). The increment of each measurement was presented as a percentage in Figure 3. It was calculated from the ratio of the increment of the score of each measurement before and after the therapies to the initial score before the therapies, which was (after−before)/before in each group. The increments of the GMFM score and the WeeFIM motor, self-care, and total scores were 26%, 33%, 40%, and 28% in the TG, whereas they were 17%, 19%, 29%, and 18% in the CG, respectively. Greater improvements were observed in the TG concerning all the measurements, although without statistical significance (p > 0.05). No adverse effect was recorded during the study in both groups.
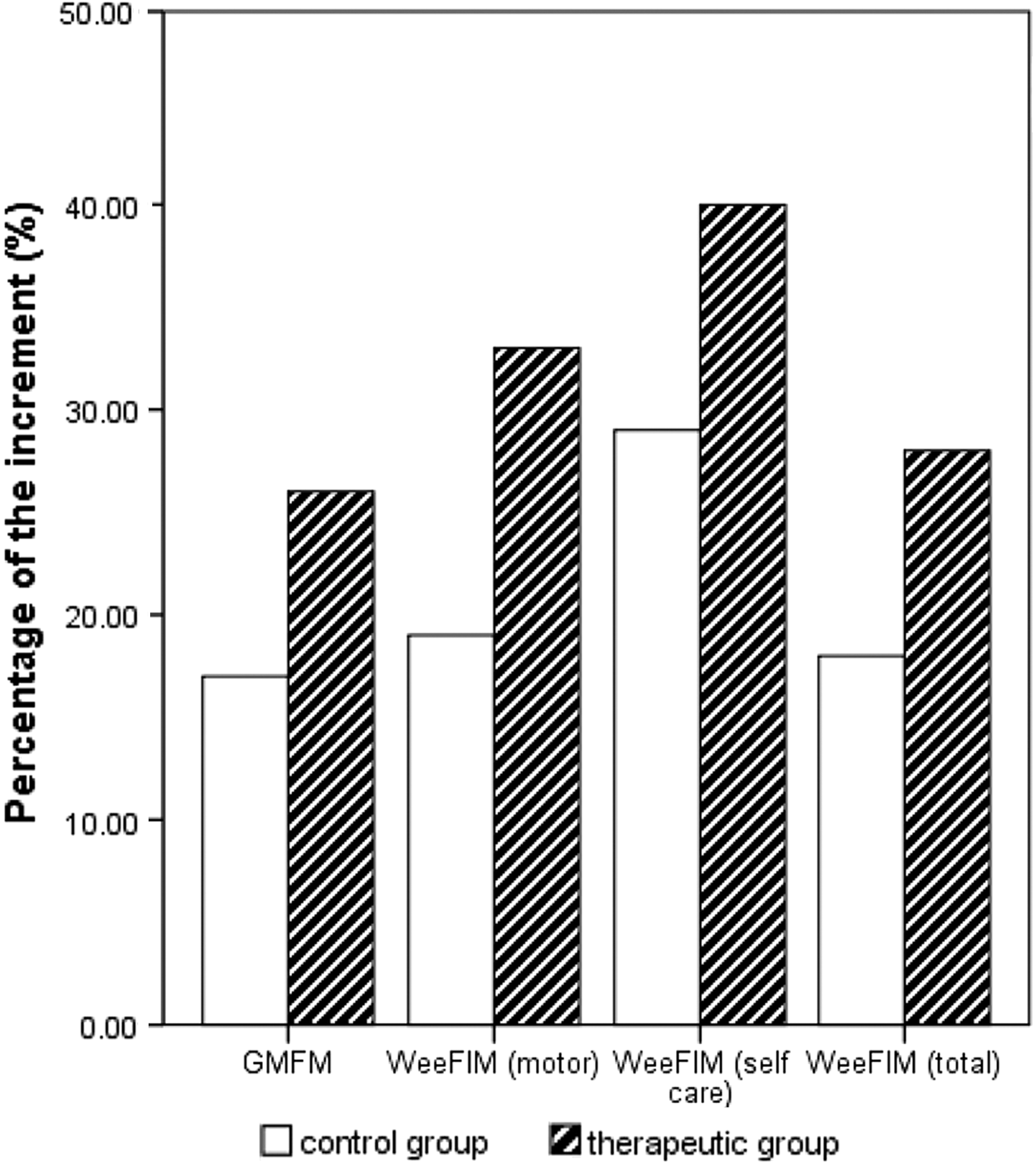
Percentages of the increments of the measurements. The increments of the GMFM, the WeeFIM (motor), WeeFIM (self-care), and WeeFIM (total) were 26%, 33%, 40%, and 28% in the TG, whereas they were 17%, 19%, 29%, and 18% in the control group, respectively. GMFM, Gross Motor Function Measure; WeeFIM, Functional Independent Measurement for children; TG, therapeutic group.
GMFM, Gross Motor Function Measure;
Correlations between functional improvements and the demographics
The correlations between functional improvements and the demographics are presented in Table 3. No statistically significant correlation was shown between the parameters in the TG (p > 0.05), neither in the CG (p > 0.05).
(R) indicates it is the correlation coefficients provided in the table.
Correlations between functional improvements
The correlations between functional improvements in each group are presented in Table 4. The GMFM improvement was not significantly correlated with the improvements in the WeeFIM motor, self-care domain, and total score. It is found that the WeeFIM motor score was positively correlated with the WeeFIM self-care score (r = 0.891 in the TG, p < 0.01 and r = 0.935 in the CG, p < 0.01); the WeeFIM self-care score was positively correlated with the WeeFIM total score (r = 0.894 in the TG, p < 0.01 and r = 0.971 in the CG, p < 0.01); and the WeeFIM motor score was positively correlated with the WeeFIM total score (r = 0.951 in the TG, p < 0.01 and r = 0.930 in the CG, p < 0.01).
The correlation is significant at the 0.01 level (two-tailed).
Discussion
As a new technique, the definition of TEAS remains debated. The International Association for the Study of Pain described acupuncture-like TENS as “low frequency (2–4 Hz), higher intensity (to tolerance threshold), and longer pulse width (100–400 μs),” whereas conventional TENS is “high frequency (50–100 Hz), low intensity (paresthesia, not painful), and small pulse width (50–200 μs).” 7 However, various protocols have been carried out in clinical application of TEAS. Typically, two types of pulse frequencies, 2 and 100 Hz, have been used as acupuncture-like TENS. 29 One study revealed that the mechanisms of low- (2 Hz) and high-frequency (100 Hz) TEAS were distinct. For analgesia, the low-frequency TEAS exerted its effects on default mode network and other cortical regions, whereas the high-frequency TEAS was on ventral striatum and dorsal anterior cingulate cortex. 29 Two or 100 Hz TEAS at Hegu (LI 4) increased the amplitude of H-reflex; however, a higher electrical frequency such as 100 Hz TEAS led to habituation easily. 26 On the contrary, one recent study revealed that 100 Hz TEAS helped reduce wrist spasticity significantly compared with 2 Hz TEAS, after brain injury. 21 Therefore, 2 Hz of the pulse frequency and 200 μs of the pulse width were a reasonable protocol. Whether it is the preferable protocol remains controversial, requiring further investigation.
In the theory of Traditional Chinese Medicine, stimulation of Shousanli (LI10) and Waiguan (SJ5) was thought to be effective in treating upper extremity paralysis by Traditional Chinese Medicine practitioners. 30 Based on Chen's study, application of acupuncture on the SJ5 modulated the synchronization of different brain networks, which help cooperate bilateral hemispheres to facilitate sensorimotor function of the affected side of the body. 31 Research showed marked activation of the anterior lobe of the cerebellum and limbic lobe was observed after de qi sensation on SJ5. 32 To the best of the authors' knowledge, no study using fMRI was performed and revealed any results with acupuncture on LI10. The electrodes placed on Shousanli (LI10) and Waiguan (SJ5) were also on the surface of the digital and wrist extensors and part of the brachioradialis. Potential effects on activation of these muscles may be involved in restoring balancing between the extensors and the flexors. However, the assumption needs to be further studied. It is believed that application of TEAS on these acupuncture points led to an integrated effect as already mentioned.
Other rehabilitation modalities were reported effective in improving motor functions and self-care abilities in CP, such as constraint-induced therapy (CIT), task-oriented approach, neuromuscular electrical stimulation, and taping technique. In Chen's study, greater improvement was discovered in the WeeFIM self-care domain (mean increased 3 points after 4 weeks therapy) in children aged around 8 years old who were treated in a home-based CIT program than those in the traditional rehabilitation group. 33 In Song's study, after a 6 weeks task-oriented training, the average improvement in the WeeFIM (total) score was 7 points (109 points pretreatment vs. 116 points post-treatment), however, without control. 34 In Ilkay's study (children aged around 6–8 years old), after 12 weeks Kinesio taping, greater improvements in GMFM and WeeFIM were shown in the treatment group (mean increased 8 points and 4 points, respectively) compared with those in the CG (mean increased 3 points and 0 points, respectively). 35 In this study (children aged average 3 years old), after 8 weeks TEAS, greater improvements in GMFM and WeeFIM (self-care) were shown in the TG (mean increased 36 points and 8 points, respectively) than in those in the CG (mean increased 22 points and 6 points, respectively), however, without statistical significances. As reported, younger age was related to clinically meaningful improvements in self-care activities. 36
Numerous studies showed correlations between motor functions and self-care abilities. 36 –38 The MACS level was the strongest predictor of self-care skills, whereas the GMFCS level was the strongest predictor of mobility skills. 38,39 No demographic factor that could affect motor functions and self-care abilities was determined in the study, possibly due to the insufficient number of samples. However, in both groups, the improvement in the WeeFIM motor score was positively correlated with that of the self-care score, as well as in the total score. The results indicated a strong positive relationship between motor functions and self-care abilities in CP patients.
The sample size of the preliminary study was relatively small. The results revealed a tendency of TEAS on promoting motor function recovery and improving the ability of self-care in children with CP. However, statistical significances were not found in the study. Pertinent scales for hand dexterity, upper extremity function, self-care ability, and ADLs, such as the Quality of Upper Extremity Skills Test and the Pediatric Evaluation of Disability Inventory, should be used in future studies to confirm the results. 40
In conclusion, TEAS could be helpful in improving motor functions and self-care abilities in children with CP, in addition to conventional exercise therapy. Larger samples are required to confirm the efficacies.
Footnotes
Acknowledgments
The authors sincerely thank the following persons for their contributions to this study: Yongshan Hu, MD, MSc, Huashan Hospital; Fanhua Huang, Huashan Hospital; Baoying Cheng, Fan Wang, Yonghe Branch of Huashan Hospital; Huiyu Zhou, Shanghai Children's Hospital; Xiaoyi Sun, Baoshan Community Health Center; and Beihua Zhang, Shanghai Yangguang Rehabilitation Center. This study was supported by the health research program in the Zhabei District, Shanghai (No. 2011ZD07), and the socialized rehabilitation program for children with cerebral palsy in the Zhabei District, Shanghai, China (shzbcl-2012-05).
Author Disclosure Statement
No competing financial interests exist.