
Abstract
Objectives:
Neuropathy and its associated pain pose great therapeutic challenges. While there has been a recent surge in acupuncture use and research, little remains known about its effects on nerve function. This review aims to assess the efficacy of acupuncture in the treatment of neuropathy of various etiologies.
Methods:
The Medline, AMED, Cochrane, Scopus, CINAHL, and
Results:
Fifteen studies were included: 13 original RCTs, a long-term follow-up, and a re-analysis of a prior RCT. The selected RCTs studied acupuncture for neuropathy caused by diabetes, Bell's palsy, carpal tunnel syndrome, human immunodeficiency virus (HIV), and idiopathic conditions. Acupuncture regimens, control conditions, and outcome measures differed among studies, and various methodological issues were identified. Still, the majority of RCTs showed benefit for acupuncture over control in the treatment of diabetic neuropathy, Bell's palsy, and carpal tunnel syndrome. Acupuncture is probably effective in the treatment of HIV-related neuropathy, and there is insufficient evidence for its benefits in idiopathic neuropathy. Acupuncture appears to improve nerve conduction study parameters in both sensory and motor nerves. Meta-analyses were conducted on all diabetic neuropathy and Bell's palsy individual subject data (six RCTs; a total of 680 subjects) using a summary estimate random effects model, which showed combined odds ratio of 4.23 (95% confidence interval 2.3–7.8; p < 0.001) favoring acupuncture over control for neuropathic symptoms.
Conclusions:
Acupuncture is beneficial in some peripheral neuropathies, but more rigorously designed studies using sham-acupuncture control are needed to characterize its effect and optimal use better.
Introduction
A
Peripheral neuropathy (PN) is broadly defined as damage to the peripheral nervous system caused by a primary lesion or dysfunction, 10 with polyneuropathy involving multiple nerves and mononeuropathy involving a single nerve. The most common causes of polyneuropathy are diabetes, thyroid disorders, vitamin B12 deficiency, alcohol abuse, chemotherapy, and human immunodeficiency virus (HIV) infection. 10,11 In spite of exhaustive workups, no cause is identified in one third of PN cases, and they are considered idiopathic. 11,12 The most common mononeuropathies are carpal tunnel syndrome (CTS), which is caused by demyelination of the median nerve at the wrist, 10 and Bell's palsy, which involves the facial nerve and causes facial weakness. 13 PN is often accompanied by painful paresthesias, which present a great therapeutic challenge. 10,14 Integrative treatments such as acupuncture are used in pain clinics with increasing popularity and are gaining acceptance among the U.S. public and academic community. 15,16 This acceptance of acupuncture has prompted growing research into integrative therapies for the challenging treatment of neuropathic pain. To the authors' knowledge, there has been no critical, systematic appraisal of the effects of acupuncture across all types of neuropathy, including both poly- and mononeuropathy.
Objectives
The objective of this review is to examine critically the evidence in the published literature for the safety and efficacy of acupuncture in the treatment of PN and associated symptoms compared to sham acupuncture or conventional medical therapy. Furthermore, acupuncture's effectiveness across various neuropathic conditions, as evidence permits, is also assessed.
Methods
Search strategy
The following electronic databases were searched from inception to July 2015: Medline, Cochrane Library, Scopus, AMED, CINAHL, and
Subject characteristics
Only adults (age >18 years) were included in the search parameters, as neuropathy, with the exception of Bell's palsy and hereditary neuropathies, is rare in children. The type of PN studied was further stratified by etiology as diabetic, chemotherapy-induced, HIV-induced, post-herpetic, idiopathic, or mononeuropathy such as CTS or Bell's palsy.
Intervention
Acupuncture was defined as the stimulation of acupuncture points by needles that pierce the skin, with or without electric stimulation, with or without moxibustion (heating with the mugwort herb). Methods of stimulating acupuncture points without needle insertion (laser, acupressure) were also searched. Controls needed to be active and included sham acupuncture or relevant medical treatments such as drugs or injections. Co-interventions were allowed only if they were given to both the intervention and the control group.
Outcome measures
One of the following outcome measures was required for inclusion: nerve conduction studies (NCS); validated questionnaires such as Symptom Severity Score, the Visual Analogue Scale, Global Symptom Score, or McGill Pain Questionnaire score; or clearly defined study-specific objective criteria distinguishing responders from non-responders.
Data extraction
The review team consisted of two neurologists with expertise in acupuncture, neuromuscular disorders, neurophysiology, and statistical methodology. Initially, an abstract review was performed to determine study eligibility. Studies were excluded if they were not RCTs or did not have acupuncture or PN as their focus. Other reasons for exclusion were the lack of a non-acupuncture control condition, such as comparing acupuncture with manual manipulation to acupuncture without manual manipulation or comparing acupuncture plus moxibustion to acupuncture alone. The remaining studies were reviewed in detail.
The Scale for Assessing Scientific Quality of Investigations in Complementary and Alternative Medicine Version (SAS-QI CAM), an instrument specifically designed to evaluate RCTs focused on integrative therapies, 17 was utilized. It assesses methodological problems and sources of bias commonly encountered in integrative medicine research, such as allocation concealment, investigator and subject blinding, blinded outcome assessment, reproducibility of experimental procedures, and sound statistical analysis. The two reviewers assigned each paper a SAS-QI CAM score independently and in a blinded fashion. As the two reviewers were in agreement, there was no need to use a third reviewed as tiebreaker. Based on a recent study by D'Silva et al., 18 a SAS-QI CAM score of >9 (out of 21) served as the cutoff for inclusion based on RCT overall scientific quality.
Data synthesis plan
All included RCTs on acupuncture for diabetic peripheral neuropathy (DPN) and Bell's palsy used composite improvement scales such as “markedly relieved/improved/failed” 19 or “marked effectiveness/effectiveness/failure,” 20 reported at the level of the individual subject. These were converted to dichotomous “no improvement” and “improvement” variables and included in meta-analysis using standard pooling procedures based on odds ratios. Contingency tables were developed with acupuncture as the treatment marginal and improvement from baseline as the outcome marginal. Fisher's exact test was used to calculate the odds ratios as the primary endpoints. Weights for the studies were calculated based on reciprocal of the variance and normalized based on the total sum of the weights used in the meta-analyses. In addition to a standard fixed-effects Mantel–Haenszel model, a random effects meta-analysis was done due to the expected increase in heterogeneity resulting from combining Bell's palsy and DPN studies. Beyond the basal evaluation, a separate meta-analysis was conducted exclusively on the DPN subjects. All statistical analyses were conducted using R v3.0.2 21 with additional utility from the “rmeta” package. 22
Results
Included studies
Initial searches generated 1008 records, and 772 remained after duplicate removal (Fig. 1). Of these, 726 studies were excluded after abstract review, leaving 46 to be reviewed in detail for eligibility. Initial searches identified studies with a focus on acupuncture for the treatment of DPN, chemotherapy-induced neuropathy, HIV-related neuropathy, idiopathic neuropathy, zoster neuralgia, traumatic peroneal neuropathy, and various cranial neuropathies such as Bell's palsy and trigeminal neuralgia. Of the 46 studies that underwent full review, 15 were excluded because they were not RCTs 23 –37 : three for an improper control condition, including verum acupuncture 38 –40 ; three because they did not focus on acupuncture/involved multiple interventions 41 –43 ; one 44 because it was identified as a duplicate to an included paper 45 ; one because it was descriptive only 46 ; and eight because of a low SAS-QI CAM score (<10). 47 –54
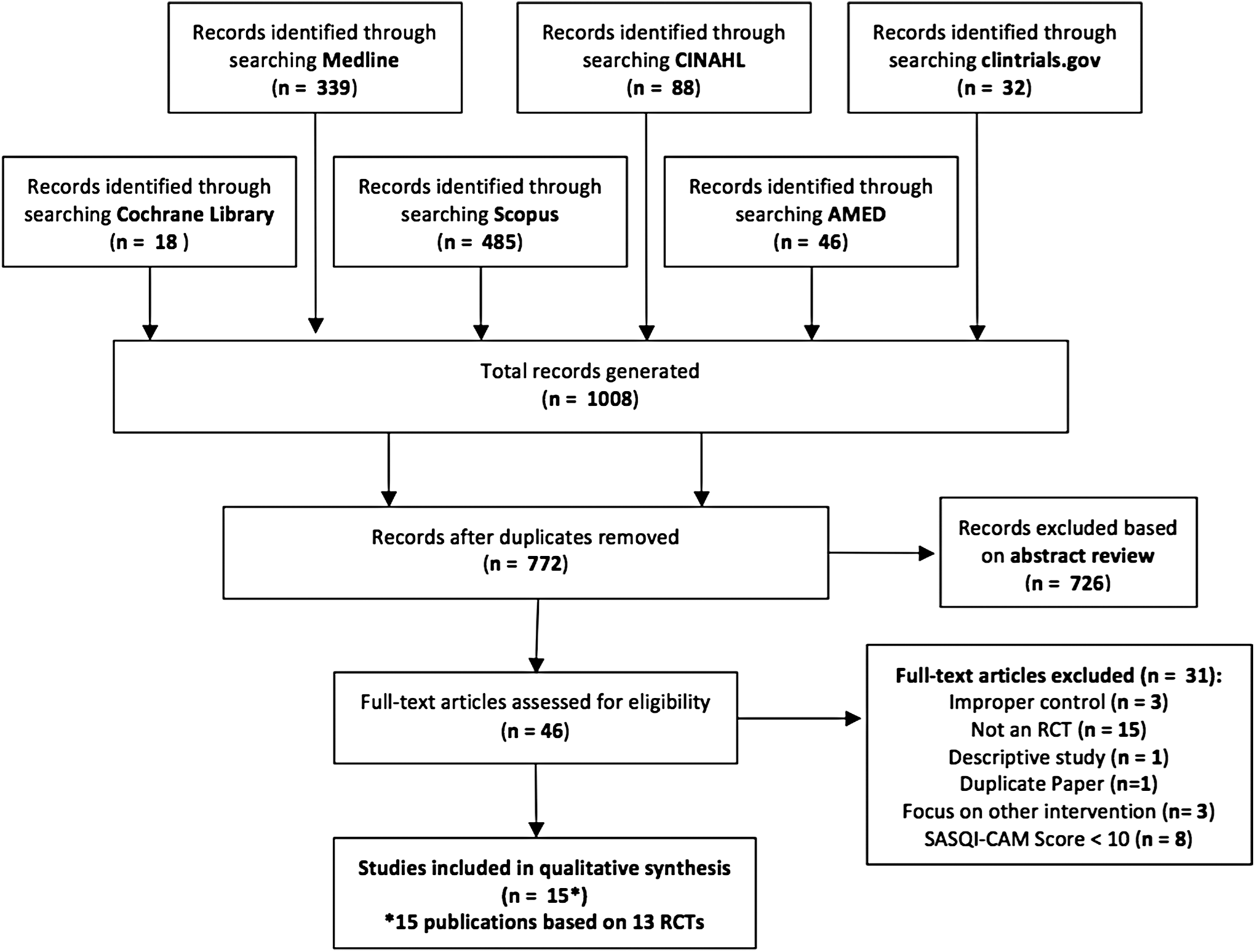
Database search flow diagram.
Following a detailed review, 15 papers met the final inclusion criteria (Table 1): 13 RCTs, a 13-month follow-up 55 of an original RCT, 56 and a re-analysis 57 of a previously published paper. 58 The selected studies focus on acupuncture for the treatment of neuropathy caused by Bell's palsy, 45,59 CTS, 55,56,60 –62 diabetes, 19,20,63,64 HIV, 57,58,65 and a combination of diabetes and idiopathic causes. 66 Of the included RCTs, nine studied manual acupuncture with or without moxibustion, three studied electroacupuncture, and one studied a combination of manual and electroacupuncture. Other active interventions included per os (P.O.) medications, intramuscular (i.m.)/intravenous (i.v.) injections, or splinting. As planned, all selected studies had an active control arm.
Control condition included in meta-analysis.
CTS, carpal tunnel syndrome; DM, diabetes mellitus; i.m., intramuscular; P.O., per os (oral); HIV, human immunodeficiency virus; i.v., intravenous; IPN, idiopathic peripheral neuropathy; Tx, treatment; SASQI-CAM, scale for assessing scientific quality of investigations in complementary and alternative medicine.
All included RCTs studied adult male and female outpatients, with the exception of Yu et al. who studied diabetic neuropathy in the hospital setting 19 (Table 2). While most studies originated in China, 19,20,45,56,59,63,64 others involved outpatients in Iran, 60 Thailand, 61 and the United States. 58,62,65,66 Across studies, sample sizes ranged from 16 to 480 subjects, treatment courses ranged from 20 days to 3 months, and acupuncture frequency ranged from daily to weekly. There was significant variability in how neuropathy was diagnosed, including neurologic exam, symptom scales, NCS, and serologic testing. The same applied to outcome measures, which ranged from subjects' symptom ratings to validated clinical scales (Table 3), NCS (Table 4), serologic testing, and study-specific graded improvement scales.
Markedly relieved/improved/failed based on exam and symptoms.
Remarkable effectiveness/effectiveness/ineffectiveness based on symptom and clinical sign score.
Marked/some/none based on symptoms, exam, labs, NCVs.
Marked effectiveness/effectiveness/failure based on symptoms.
Cured/obviously improved/improved/no improvement based on House–Brackmann Scale and Facial Disability Index.
Global Pain Relief Score—complete/a lot/moderate/slight/none/worse.
BCTS, Boston Carpal Tunnel Score; BDI, Beck Depression Inventory; CMAP, Compound Muscle Action Potential; CSI, Combined Sensory Index; CTSAQ, Carpal Tunnel Self-Assessment Questionnaire; DML, distal motor latency, DSL, distal sensory latency; FDI, Facial Disability Index; FDIP, FDI Physical; FDIS, FDI Social; GPS, Gracely Pain Score; GSS, Global Symptom Scale; MNCV, motor nerve conduction velocities; NCS, nerve conduction studies; NCV, nerve conduction velocity; PN, peripheral neuropathy; QOL, quality of life; SNAP, sensory nerve action potential; SF-36 QOL, San Francisco-36 Quality of Life inventory; SNCV, sensory nerve conduction velocities; W-P SNCV, wrist–palmar sensory nerve conduction velocity; VAS, Visual Analog Scale.
⇑⇑, increased (p < 0.01); ↑,increased (p < 0.05); ⇔, no significant change (p > 0.05); ↓, decreased (p < 0.05); ⇓⇓, decreased (p < 0.01).
DPN
Four RCTs met the eligibility criteria. 19,20,63,64 These studies were conducted in China and used manual acupuncture 20,63,64 or electroacupuncture 19,64 in combination with snow lotus injection in acupuncture points 64 and i.v. vitamin B12. 20 All studies used P.O., i.m., or i.v. medication control (Table 2). Outcome measures included study-specific graded composite improvement scales based on symptoms, 19,20,63,64 clinical signs, 63 exam, 19,63 labs, 19 and NCS. 19,20 The included studies reported significant improvement in acupuncture groups compared with control in neurologic exam, 19,20,64 neuropathic symptoms, 19,63,64 composite improvement scales, 19,20,63,64 NCS, 19,20 and blood rheology. 19
HIV-related neuropathy
One included study of manual acupuncture for HIV-related neuropathy from the early-mid 1990s 58 had enrollment difficulties and a 20–35% dropout rate due to significant HIV morbidity. This led to a complicated “factorial option” design with eight trial arms, which made a direct comparison of amitriptyline to acupuncture impossible. The study found significantly higher pain relief in the acupuncture group (p = 0.03). However, this was not true after adjustment for multiple comparisons. Shiflett et al. 57 reanalyzed data from this trial using baseline pain as a covariate in a repeated-measures analysis of covariance and found that baseline pain intensity was significant (p < 0.001) and so was the interaction of acupuncture and amitriptyline over time (p < 0.017). Amitriptyline alone or acupuncture alone showed significant reduction in Gracely Pain Scale score at 6 weeks. However, only acupuncture sustained this effect at 14 weeks (Tables 2 and 3). When amitriptyline and acupuncture were combined, they did not differ from placebo.
Anastasi et al. 65 also found significant reduction in Gracely Pain Scale following a 6-week course of manual acupuncture/moxibustion compared to sham acupuncture/placebo moxibustion control (Table 2). Additionally, the acupuncture group had significant improvement on the Subjective Peripheral Neuropathy Screen compared to its pretreatment baseline.
Idiopathic neuropathy
One RCT on electroacupuncture for idiopathic neuropathy was included. 66 Four subjects with diabetic neuropathy and 12 with idiopathic neuropathy were enrolled in a double-blind crossover study comparing electroacupuncture to sham-electroacupuncture (eight subjects per group). There was no difference between acupuncture and control in any of the outcome measures used: Visual Analogue Scale, Patient's Global Impression of Change, Beck Depression Inventory, and the SF-36 Quality of Life Instrument (Table 3). Both groups showed no difference from baseline. The authors did not analyze data from the diabetic and idiopathic neuropathy subjects separately (Table 2).
CTS
All four RCTs 56,60,61,62 used validated CTS-specific scales (Table 2) and reported significant improvement with manual acupuncture 56,60,62 and electroacupuncture 61 compared with baseline in the Global Symptom Score, 56,60 Boston Carpal Tunnel Score, 61 Carpal Tunnel Self-assessment Questionnaire, 62 and Visual Analogue Scale 61 (Table 3). Three of the four RCTs included showed significantly greater effectiveness of acupuncture compared with night splinting, 61 sham acupuncture, 60 oral vitamin B1 and B6, 60 and oral prednisolone. 56 In contrast, Yao et al. 62 revealed no difference in CTS symptoms between acupuncture plus night splinting compared to sham acupuncture plus night splinting, with both groups improved from baseline. Most long-term follow-ups favored acupuncture at 4 weeks, 56,60 5 weeks, 61 7 months, and 13 months, 55 with only a single study showing no difference between acupuncture and control at 3 months. 62
Bell's palsy
Two RCTs with 480 45 and 119 59 subjects met the inclusion criteria (Table 2). Li et al. 45 included an intermediate treatment group, “Control 1,” which received both acupuncture and medical therapy, and a medical therapy “Control 2” group. Tong et al. 59 included an oral steroid group “Control 1” and a home exercises “Control 2” group (Table 2). Li et al. 45 found significant improvement in the House–Brackmann Scale and Facial Disability Index in the acupuncture group compared with medical therapy and of the acupuncture plus medical therapy “Control 1” over the medical therapy “Control 2.” In contrast, Tong et al. 59 found no significant difference on the House–Brackmann Scale, as all three groups had high improvement rates.
Acupuncture-induced changes in nerve conduction parameters
NCS were performed in included trials on DPN and CTS (Table 4). With respect to motor nerve function, acupuncture produced significant effects on median nerve compound muscle action potential (CMAP) amplitude, median nerve distal motor latency (DML), and motor nerve conduction velocity (NCV) of the median, ulnar, and peroneal nerves. Compared with medication control, acupuncture caused significantly greater improvement in DML and in median, ulnar, and motor NCV.
Sensory NCS revealed that acupuncture caused an increase in sensory nerve action potential (SNAP) amplitude in the median nerve, lowered median nerve distal sensory latency (DSL), and increased median and peroneal nerve NCV. However, compared to medication control, acupuncture showed significant improvement only in median nerve sensory NCV 60 (Table 4).
With respect to longer-term NCS changes, acupuncture-treated groups had faster sensory NCV, a trend (p = 0.07) toward shorter DSL 60 at 4 weeks, and shorter DML and motor NCV at 13 months. 55
Meta-analysis on acupuncture for Bell's palsy and diabetic neuropathy
Outcomes from all included trials on DPN and Bell's palsy were reported on the individual subject level and included in this meta-analysis. All trials used medication control. Data from Li et al.'s 45 “Control 1” were excluded because acupuncture was administered, and from Tong et al.'s 59 “Control 2” because it was not an active control. The third arms of both trials were included in the data synthesis. A forest plot for acupuncture against control treatment was constructed using contingency tables of acupuncture against the control condition (Fig. 2). Meta-analysis on the DPN subjects showed an overall increased effect of acupuncture over control, which was still present (p < 0.001) when correcting for study heterogeneity (mean odds ratio [OR] = 4.85; 95% confidence interval [CI] 2.2–11). Meta-analysis on the Bell's palsy subjects also showed an increased effect of acupuncture over control (p = 0.042) when correcting for heterogeneity (mean OR = 2.78; 95% CI 1–7.4). Similarly, the pooled meta-analysis of all trials studying diabetic neuropathy and Bell's palsy, when adjusting for study heterogeneity, found a mean OR of 4.23 in favor of acupuncture over control (95% CI 2.3–7.8, p < 0.001).
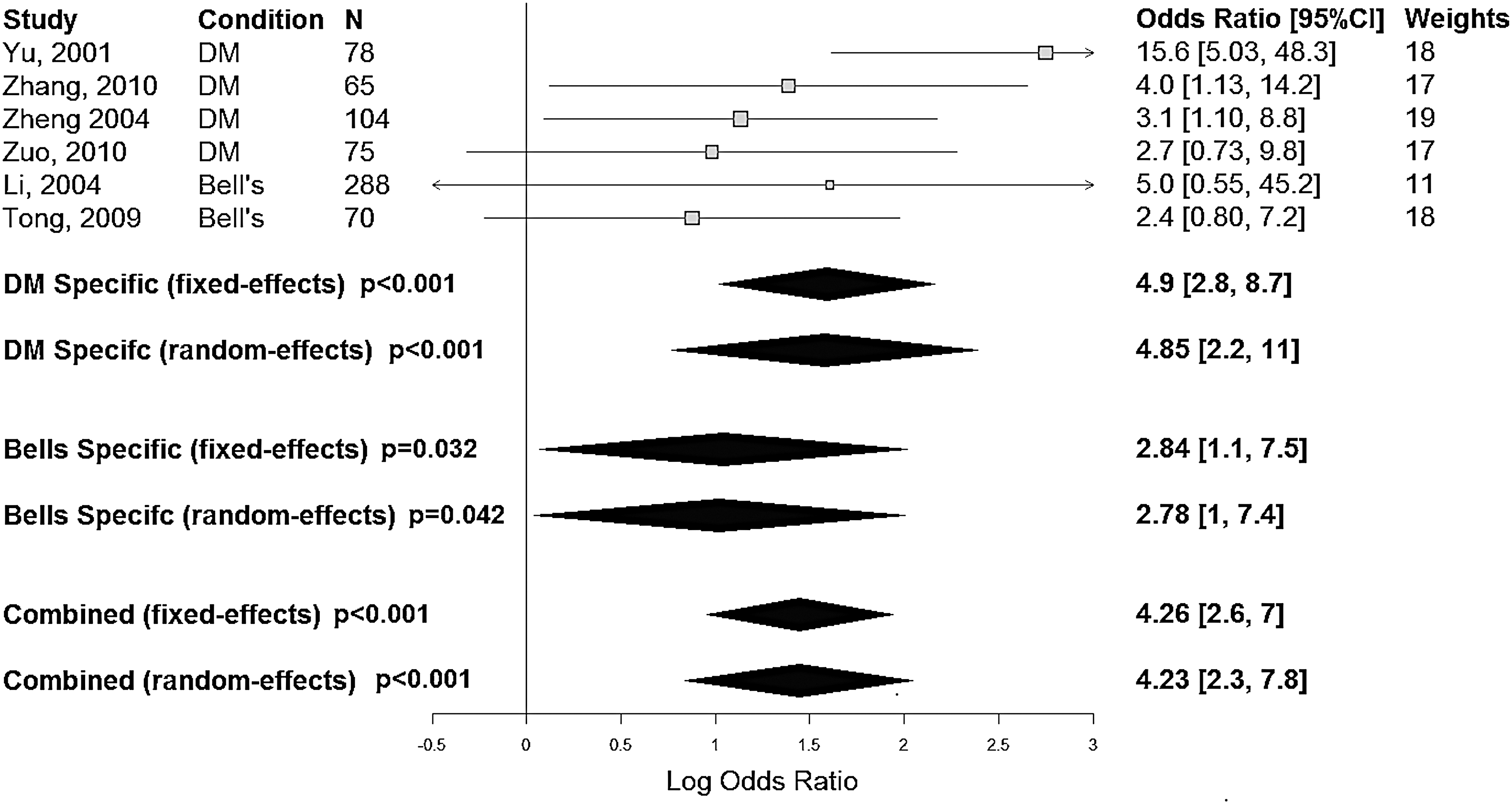
Meta-analysis results for diabetes mellitus and Bell's palsy.
Acupuncture safety, adverse events
The included studies varied greatly in how adverse events were defined and monitored. Overall acupuncture treatment appeared safe, without serious adverse events, except in the early study on HIV-related neuropathy 58 where both groups experienced significant morbidity. There was a trend toward lower rates of life-threatening events in the acupuncture group (3/58 subjects) compared with the control group (10/56; p = 0.06), with a high combined 2-year mortality rate (28.8%). The remaining studies reported no acupuncture-related serious adverse events. Minor adverse events included minor bruising with acupuncture, 56,59,65 which in one study was as common as 20% of subjects 61 ; local discomfort with needle insertion; pain following session; and uncomfortable paresthesias during acupuncture in 5% of subjects. 56
Discussion
To date, no critical appraisal of acupuncture's effect on PN of various etiologies has been conducted. Prior systematic reviews were published in the areas of acupuncture for DPN, CTS, and Bell's palsy. The evidence is summarized below, along with the authors' perspective.
Acupuncture for DPN
The included RCTs involved manual acupuncture 20,63 or electroacupuncture, 19 which were superior to control conditions in DPN, as was the combination of both therapies. 64 Further studies are needed to compare acupuncture to electroacupuncture in DPN.
By far the largest number of RCTs identified in preliminary searches dealt with acupuncture for DPN. However, only four RCTs met the inclusion criteria due to poor overall quality of the reviewed studies. In 2012, Bo et al. 67 attempted a systematic review and identified 75 RCTs (73 in Chinese) on acupuncture for DPN. They concluded that the majority of those were of low-moderate methodological quality, while none of the trials met all of the CONSORT 68 and STRICTA 69 criteria. A systematic review was thus not conducted.
In 2013, Chen et al. 70 reviewed 25 Chinese RCTs studying manual acupuncture for DPN. None of the included RCTs met all the CONSORT and STRICTA criteria, and there were no clear inclusion criteria. Meta-analysis on 23/25 RCTs suggested that acupuncture is more effective on a “global symptom improvement scale” than mecobalamin, vitamin B1 and B12, and no treatment. The authors identified multiple methodological problems and suggested that their findings were inconclusive. Neither study included the four English language trials on DPN identified in the present study. 19,20,63,64
Similar conclusions were reached in this study to those of Chen et al. 70 who found acupuncture to be superior to oral thiamine plus i.m. vitamin B12, 19 i.v. vitamin B12, 20 oral mecobalamin, 64 and oral inositol. 63 Similar to the above reviews, multiple methodological problems were encountered.
Acupuncture for Bell's palsy
The same six Chinese RCTs 71 –76 were included in two Cochrane reviews on Bell's palsy 77,78 and in a systematic review 79 published by the same group. Collectively, these six RCTs suggested that acupuncture leads to improved facial nerve recovery. However, the authors warned that the conclusions cannot be trusted due to multiple methodological flaws. Tong et al. 59 was not referenced. Li et al. 45 was excluded from the Cochrane reviews due to use of moxibustion. Moxibustion is the stimulation caused by burning the herb Artemisia vulgaris over an acupuncture point and is widely regarded as an acupuncture modality. Trials using moxibustion were included in the present review, as long as acupuncture was also used as active intervention.
In 2012, Kim et al. 80 reviewed eight RCTs, among them Tong et al., 59 two studies included in the Cochrane reviews, 72,74 and additional five Chinese language RCTs, 81 –85 all published prior to 2010, which were not included in the Cochrane 2010 review for unclear reasons. The authors excluded moxibustion, and this may be why Li et al. 45 was not selected. The authors found that both acupuncture plus medication and acupuncture alone were more effective than medication alone. The authors concluded that acupuncture may be a useful adjunct or an alternative to drug therapy. However, they identified multiple methodological flaws.
The latest review on the subject included 14 RCTs 86 —all six RCTs from the Cochrane reviews, all RCTs reviewed by Kim et al., plus two additional Chinese language RCTs. 87,88 The authors did not critically assess RCT quality except for rating them “high,” “low,” and “unclear.” Meta-analysis pooled data from 1541 individual subjects, using “effective rate” as the outcome. Acupuncture was found to be superior to control interventions (risk ratio [RR] = 1.14; 95% CI 1.04–1.25). The authors felt that their results were inconclusive due to various methodological flaws.
As the present search was limited to the English language, only two trials on manual acupuncture for Bell's palsy were included, with 599 subjects combined, which had different results. Li et al. 45 found that acupuncture was more effective than a combination of acupuncture and medical therapy or medical therapy alone. Conversely, Tong et al. 59 found no difference between acupuncture and the two control groups—oral steroids and home facial exercises—as all three groups had high rates of improvement from baseline. Studying episodic, self-limiting conditions such as Bell's palsy presents a challenge because the remission rate is 85% within the first 3 weeks and close to 100% within 6 months. 89
Much has been written about the bias of acupuncture research coming from China. As early as 1998, Vickers et al. 90 cautioned about publishing bias and the lack of negative trials. While this study is almost 20 years old, there are no negative RCTs in any of the selected reviews, which raises questions about continued publication bias.
Acupuncture for CTS
The present review found that manual acupuncture 56,60 and electroacupuncture 61 were more effective than control in three of the four included RCTs on CTS. 56,60,61 Both acupuncture and sham-acupuncture groups improved significantly in the fourth included RCT. 62 A possible explanation may be that CTS has a relatively high remission rate, ranging from 33% at 6 months 91 to >50% at 1 year. 92
All four included studies on CTS involved needle placement near the median nerve. Yang et al. found this effect to be sustained at 13 months. 55 Further studies are needed on acupuncture's long-term effects. Similar to the present findings, Sim et al. 93 reviewed six RCTs and found acupuncture to be more effective than control in five RCTs. The authors cautioned that the selected RCTs had multiple methodological flaws and were underpowered.
Acupuncture point selection
In addition to varied acupuncture treatment courses, the included RCTs used a wide variety of acupuncture points (Table 5). Point selection rationale was not justified in any RCTs, except for one. 63
There was some consistency in point selection in the treatment of CTS and Bell's palsy. All included CTS trials involved points on the ipsilateral pericardium meridian: PC6, 56,60,62 PC7, 56,60 –62 and PC8. 61 Pericardium meridian points are commonly used in CTS treatment due to their close association with the median nerve, which is affected in CTS. Similarly, both of the included Bell's palsy trials used ipsilateral points on the stomach meridian—ST2, 59 ST4, 45,59 ST6, 45,59 ST7, 45 and GB1445,59—which are in close proximity to branches of the facial nerve. Both trials also included needling of bilateral LI4, which is one of the most commonly used points for facial pain.
The RCTs focused on acupuncture for diabetic, HIV-related, and idiopathic neuropathy used a greater variety of acupuncture points with little overlap. This may be because these conditions cause polyneuropathy with more complex symptoms compared with mononeuropathies.
Overview of statistical bias
Statistical bias within the larger meta-analysis was evaluated using assessments of study heterogeneity (I 2) both within each of the disease subsets and in the pooled cohort. This combined approach was utilized to evaluate any discrepancy among the studies both within and across disease states. In all cases, the heterogeneity is not significant (Bell's: I 2 = 6%, p = 0.55; diabetes mellitus [DM]: I 2 = 47%, p = 0.12; combined: I 2 = 28%, p = 0.22), indicating the effect of acupuncture intervention is appropriately similar among the studies. Even the comparatively high I 2 value for DM is an indication of “moderate” heterogeneity according to the Cochrane criteria. 94 The analysis of heterogeneity suggests that even in the absence of negative results, the effect of acupuncture treatment is moderately consistent within and across neuropathic conditions.
Suggested mechanism of action
While the selected trials employed varied acupuncture regimens, they all involved acupuncture points located near peripheral nerves, such as points close to the median nerve for CTS and close to the facial nerve for Bell's palsy (Table 5). It is possible that acupuncture needles exert direct effect on an underlying nerve and peri-neural tissues, either through manual manipulation or electric current. This could explain why acupuncture appears to have an effect not only on neuropathic symptoms, but also on NCS parameters (Table 4). These effects were sustained up to 13 months 55 in CTS and were significantly different from the control condition. Further studies are needed before any definitive conclusions can be drawn about acupuncture's effect on NCS parameters in neuropathic conditions.
Methodological problems with standardization
One common problem in acupuncture research is the lack of standardization of point selection, number of needles used, needle retention time, needling depth, needle manipulation, use of moxibustion, and electroacupuncture. The 13 RCTs reviewed varied greatly in acupuncture point selection and in number of sessions: from six weekly sessions for DPN 62 to 36 sessions in Bell's palsy. 59 Consideration was given to calculating the amount of acupuncture delivered (in minutes or hours). However, there is no clear concept of an appropriate acupuncture dose and how much treatment is needed for a given condition. 95 The relationship between number of needles and acupuncture effect is also unclear and probably not linear.
Lastly, isolating acupuncture's effect would be simpler in RCTs that study acupuncture alone as the intervention. Half of the included RCTs combined acupuncture with another intervention—moxibustion, medication or herbs, or splinting. This is further complicated by the use of various acupuncture modalities—manual acupuncture, 20,45,56,58 –60,62,63,65 electroacupuncture, 19,61,66 or a combination of both. 64 Manual and electroacupuncture may have different mechanisms of action and different effects on neuropathy and neuropathic pain. Unfortunately, not enough electroacupuncture trials were available to draw meaningful comparisons with manual acupuncture for each of the reviewed neuropathic conditions.
Methodological problems with sample size calculations
Only two of the included RCTs 58,65 contained a sample size calculation. Therefore, it is possible that the majority of the included trials are underpowered (Table 6). In particular Penza et al. 66 only enrolled eight subjects per group, and only 12 subjects had idiopathic neuropathy. There was no statistical rationalization for this sample size and this uneven split of patients with idiopathic and diabetic neuropathy.
Markedly relieved/improved/failed based on exam and symptoms.
Remarkable effectiveness/effectiveness/ineffectiveness based on symptom and clinical sign score.
Marked/some/none based on symptoms, exam, labs, NCVs.
Marked effectiveness/effectiveness/failure based on symptoms.
Cured/obviously improved/improved/no improvement based on House–Brackmann Scale and Facial Disability Index.
Global Pain Relief Score—complete/a lot/moderate/slight/none/worse.
—, no/none.
Methodological problems with improper control and blinding
In Traditional Chinese Medicine, there is a belief that a sensation called de qi is crucial to acupuncture's therapeutic benefit. De qi has been described as aching, soreness, heaviness, warmth, coolness, tingling, numbness at the site of the needle, 96 or as radiating paresthesias. 97 Because of this belief, many RCTs from China are designed to compare de qi elicited by needle manipulation to manipulation-free needling of an acupuncture point. 39,40 Any studies that involved passive needle insertion in acupuncture point as control were excluded.
Lack of blinding of both subjects and investigators was a common methodological flaw of the selected studies. None of the studies originating in China 19,20,45,56,59,63,64 used sham acupuncture, and the subjects were not blinded (Table 6). In 7 of the 13 included studies, 19,20,45,56,59,63,64 the outcome assessors were not blinded to treatment assignment, which is source of investigator bias.
Methodological problems with placebo and expectancy
Most of the included RCTs carried out a greater number of visits or interventions in the acupuncture groups (Table 2), which may have affected subject expectancy. In many cases, the authors alluded to positive subject expectations from acupuncture, including higher dropout rates in the control condition and subjects seeking acupuncture independently. 56,59 Subject expectations and the role of placebo in general were not addressed. It is well known that positive expectation amplifies acupuncture-induced analgesia in both subjective pain ratings and objective fMRI signal changes. 98
Methodological problems with outcome measures
The 13 included RCTs contained a wide array of outcome measures, as should be expected with trials on various neuropathic conditions, involving both poly- and mononeuropathy. Overall, most trials assessed subject-reported measures of improvement, which are intrinsically subjective. Only four of the 13 RCTs used NCS for baseline and outcome measures (Table 4). More studies of neuropathy should use NCS or other objective measures of improvement such as somatosensory evoked potentials.
Several included studies used arbitrary, investigator-created scales of improvement (Table 6), such as “complete/a lot/moderate/slight/none/worse,” 58 based on a combination of symptoms, neurologic exam, and improvement on disease-specific, validated scales. These could be a significant source of bias, particularly if the outcome assessors are not blinded to treatment assignment. With the exception of Zhang et al., 63 all RCTs using investigator-created scales of improvement also used validated outcome measures.
Conclusions
This systematic review suggests that acupuncture is effective in diabetic neuropathy, Bell's palsy, and CTS, under the conditions of the included studies. Acupuncture may be effective in HIV-related neuropathy. However, further studies are needed to explore its potential therapeutic role in this population. There is a need for future studies that address point selection, acupuncture modality, and frequency. Further studies should also aim to minimize methodological flaws by incorporating proper subject and investigator blinding, standardization of acupuncture intervention, use of validated, objective outcome assessments, a priori hypotheses with proper sample and effect size calculations, and appropriate statistical analyses.
Footnotes
Acknowledgments
This study is funded by the following grants: NIH K23 AT008405 (A.D.), NIH 5T32 AT002688 (B.O.). The authors wish to thank Prof. Marian McDonagh, PharmD, from OHSU's department of Medical Informatics and Clinical Epidemiology for her contribution to this manuscript.
Author Disclosure Statement
No competing financial interests exist.