
Abstract
Objective:
There has be a large body of evidence on the pharmacological treatments for psoriasis, but whether nonpharmacological interventions are effective in managing psoriasis remains largely unclear. This systematic review conducted pairwise and network meta-analyses to determine the effects of acupuncture-related techniques on acupoint stimulation for the treatment of psoriasis and to determine the order of effectiveness of these remedies.
Methods:
This study searched the following databases from inception to March 15, 2016: Medline, PubMed, Cochrane Central Register of Controlled Trials, EBSCO (including Academic Search Premier, American Doctoral Dissertations, and CINAHL), Airiti Library, and China National Knowledge Infrastructure. Randomized controlled trials (RCTs) on the effects of acupuncture-related techniques on acupoint stimulation as intervention for psoriasis were independently reviewed by two researchers.
Results:
A total of 13 RCTs with 1,060 participants were included. The methodological quality of included studies was not rigorous. Acupoint stimulation, compared with nonacupoint stimulation, had a significant treatment for psoriasis. However, the most common adverse events were thirst and dry mouth. Subgroup analysis was further done to confirm that the short-term treatment effect was superior to that of the long-term effect in treating psoriasis. Network meta-analysis identified acupressure or acupoint catgut embedding, compared with medication, and had a significant effect for improving psoriasis. It was noted that acupressure was the most effective treatment.
Conclusions:
Acupuncture-related techniques could be considered as an alternative or adjuvant therapy for psoriasis in short term, especially of acupressure and acupoint catgut embedding. This study recommends further well-designed, methodologically rigorous, and more head-to-head randomized trials to explore the effects of acupuncture-related techniques for treating psoriasis.
Introduction
P
In addition to Western medicine, patients may seek complementary and alternative medicine to control psoriasis. 15 A previous study indicated that 13.1% of patients with psoriasis received Traditional Chinese Medicine (TCM). 5 Acupuncture-related techniques include the use of filiform needles, bloodletting or lancet needles, ear needles, and cutaneous needles; catgut embedding; medicine injection; moxibustion; acupressure; and cupping. 16 Acupuncture is an established TCM technique, which relies on the stimulation of acupoints, wherein the stimulation is transmitted to the brain and specific organs in the body to modulate physiological reactions. 17 Acupuncture treatment has fewer side effects and lower toxicity than do conventional treatments. 18 Acupoint stimulation provides an effective and safe therapy and a more pleasant patient–provider experience than does Western medicine. 19 Studies have shown that acupuncture is effective in treating psoriasis. 20,21 However, one study reported that acupuncture using filiform needles is not superior to sham acupuncture in treating psoriasis. 22
For evaluating the efficacy of psoriasis treatments, the Psoriasis Area and Severity Index (PASI) 23 as well as the criteria of diagnosis and therapeutic effects of TCM on diseases 24 have been used. The PASI is an objective measure that calculates the weighted sum score of the involved area (percentage) and severity (i.e., erythema, induration, and desquamation) of psoriasis. 23 The PASI score ranges from 0 to 72, with a higher score indicating more severe psoriasis. 25 Clinically, at least 75% reduction in the PASI score (PASI 75) is generally considered a successful treatment, whereas a 50% reduction in the PASI score (PASI 50) is considered a meaningful improvement. 26 Regarding the criteria of diagnosis and therapeutic effect of TCM on diseases, “efficacy” refers to skin lesions disappearing completely or subsiding by more than 95%, and a reduction of more than 50% is considered a meaningful improvement. 24
Acupuncture-related techniques have been used to treat psoriasis for several hundred years, and numerous studies have reported the effects of using acupuncture, acupressure, acupoint injection, bloodletting, catgut embedding, and moxibustion. 27 –32 However, detailed descriptions of techniques and outcomes are scant. 20 Therefore, this systematic review conducted pairwise and network meta-analyses to determine the effects of acupuncture-related techniques on acupoint stimulation for the treatment of psoriasis and to determine the order of effectiveness of these remedies.
Materials and Methods
Search strategy and study selection
Randomized controlled trials (RCTs) on the effects of acupuncture-related techniques on acupoint stimulation as intervention for psoriasis were independently identified by two researchers. This study searched the following databases from inception to March 15, 2016: Medline, PubMed, Cochrane Central Register of Controlled Trials, EBSCO (including Academic Search Premier, American Doctoral Dissertations, and CINAHL), Airiti Library, and China National Knowledge Infrastructure. The search strategy, which was designed for Medline and adapted for the other electronic databases, consisted of a combination of [“psoriasis” or “psoriatic”] and [“acupoint” or “complementary therapies” or “auricular stimulation” or “acupuncture” or “acupuncture therapy” or “electroacupuncture” or “stimulating the central nervous system” or “percutaneous electrical nerve stimulation” or “auricular therapy” or “electromagnetic” or “ear therapy”].
All RCTs published in English or Chinese that evaluated the effects of any form of acupuncture-related techniques in treating psoriasis were included. All duplicate articles were removed. Next, abstracts were evaluated using the PICO inclusion and exclusion criteria, following which the full text was examined. The control interventions included medication, sham, and narrow-band ultraviolet B phototherapy. This study excluded articles that involved interventions using Chinese herbal medicines or herbal medicines, participants younger than 18 years, or psoriatic arthritis. Animal studies and qualitative studies were also excluded. The outcome measures were the effective rate in treating psoriasis and adverse events. Subgroup analysis was used to determine the effects of treatment duration (1, 2, and 3 months) on the effectiveness of treatment and the type of acupuncture-related techniques (single and multiple techniques).
When two or more publications included the same, or some of the same, participants, the article that reported the largest number of participants was used. Articles in which the use of the same study population was suspected, because of similarities of participants and intervention characteristics, were excluded to prevent multiple publication bias. Two independent reviewers (S.-H.K. and Y.-C.C.) screened titles and abstracts for relevance, following which the reference lists of all identified studies were screened. Discrepancies in study selection were resolved through discussion and adjudication by two other reviewers (M.-L.Y. and C.-C.C.).
Data extraction and quality assessment
Data were independently extracted by two reviewers (S.-H.K and Y.-C.C.) from each RCT that met the criteria and entered into a systematic coding form that included the details of intervention, methods, participants, and outcomes. The following information was extracted from eligible RCTs: first author, publication year, number of participants at baseline and follow-up, mean age, dropouts, blinding, outcome measurements, and adverse events. The other two reviewers (M.-L.Y. and M.-H.W.) checked the extracted data and structured a hypothesized model of acupuncture-related techniques.
For determining the risk of bias, 33 the same reviewers assessed the methodological quality using the Jadad score 34 and the Cochrane Collaboration's tool by the same reviewers, separately. The Jadad score (0–5) contains three items, namely randomization, blinding, and follow-up, with higher scores indicating higher RCT quality. 35 The risks of bias were appraised in six domains, namely selection, performance, detection, attrition, reporting, and other resources. Each domain was classified as “low,” “high,” or “unclear” risk.
Data synthesis and analyses
Meta-analyses were performed using Comprehensive Meta-Analysis version 2.2, Stata SE version 14, and the risk for bias was assessed using Review Manager (RevMan) version 5.3. The Cochrane's Q and I 2 statistic were used to assess heterogeneity. 36 To synthesize direct and indirect evidence from the included RCTs, Bayesian meta-analytical techniques were used to perform network meta-analysis. 37 Meta-analyses were performed using random effect models of consistency 38 and side splitting. 39 Dichotomous data were compared and the results were recorded as odds ratios (ORs). Forest plots were used to present summary and individual study effect sizes with 95% confidence interval (CI). Publication bias was assessed through visual examination of the funnel plots and through Egger's asymmetry test. A p-value less than 0.05 was considered statistically significant. Funnel plots were analyzed only if at least 10 studies were included in the meta-analyses. Approximately symmetrical funnel plots were considered low risk, whereas asymmetrical funnel plots were considered having a high risk of publication bias. 40
Results
Study selection
Figure 1 depicts the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flowchart for selecting trials for this systematic review and meta-analysis. The search initially yielded 1,121 studies. After screening title and abstract, 826 were excluded due to not being relevant. Of the remaining 196 studies, 170 were excluded after the full-text screening, and the 26 potentially relevant studies were retrieved for further detailed information. Finally, 13 and 10 studies were included for pairwise and network meta-analysis, respectively.
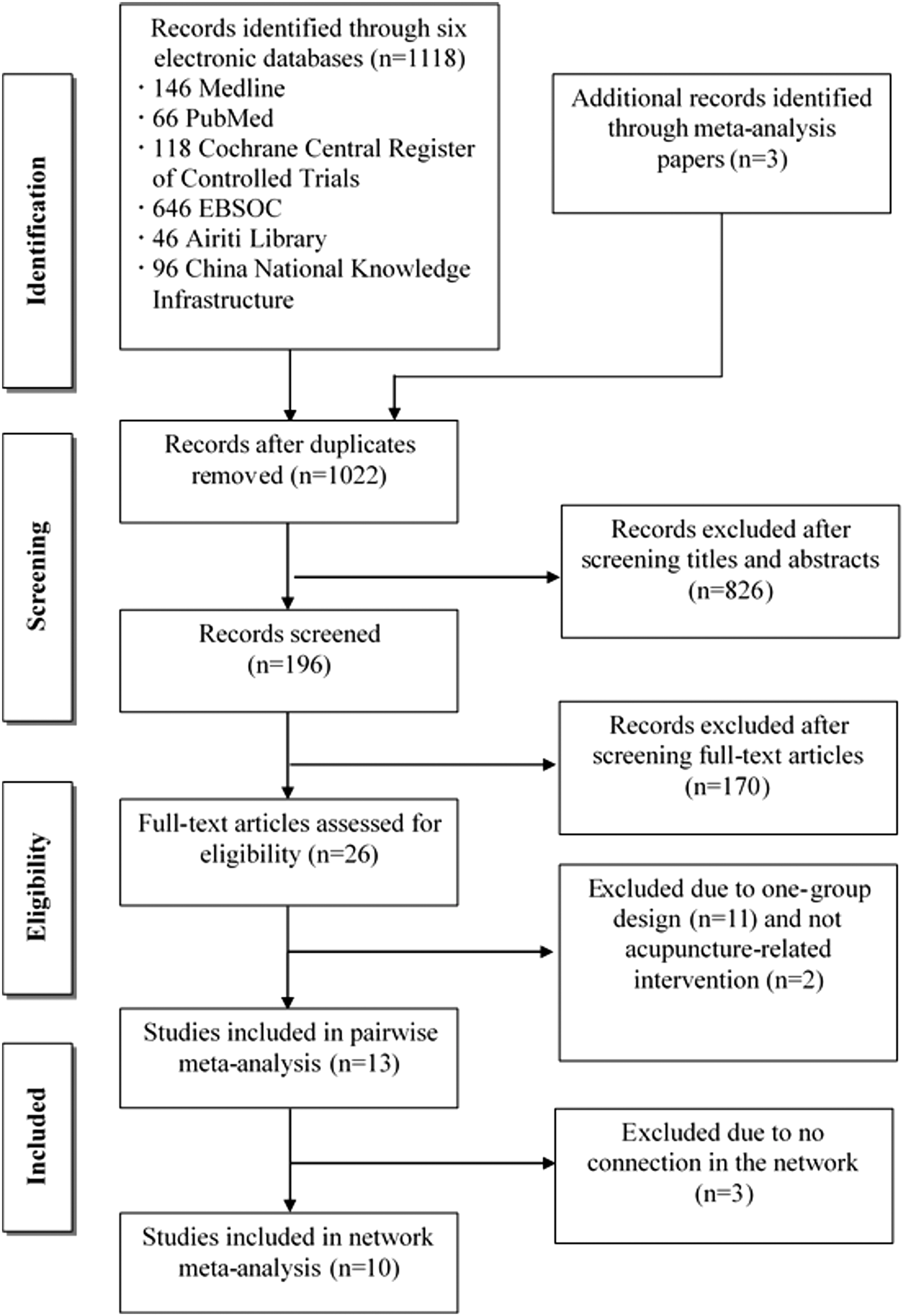
The process of selecting studies included for meta-analysis.
Study characteristics
Table 1 presents the characteristics and rigorous scores of 13 included RCTs published between 1997 and 2016. In a total of 1,060 participants, 590 participants (55.7%) were in the intervention groups of acupoint stimulation with different acupuncture-related techniques, 461 participants (43.5%) were in the control groups with no acupoint stimulation, and 9 participants (0.8%) dropped out. Eleven studies (85%) did not report dropouts. The participants included 410 men (38.7%) and 594 women (56%), whereas the sex of 56 participants (5.3%) was not reported. The average age was 37.32 ± 5.18 years and the age range was 18–77 years. The intervention duration was at least 2 months in seven studies, whereas in the other studies, it was less than 2 months. The follow-up periods ranged from 2 weeks to 2 years. Three (23%) studies were published in English and 10 (77%) in Chinese. The acupoint stimulation involved acupuncture-related techniques of acupuncture alone or combined (four RCTs), acupressure (one RCT), acupoint bloodletting alone or combined (four RCTs), acupoint catgut embedding (three RCTs), and acupoint injection (one RCT).
TCM = Criteria of diagnosis and therapeutic effect.
TCM, Traditional Chinese Medicine; PASI, Psoriasis Area and Severity Index.
Quality assessment among results
All included studies met the quality requirement (Jadad score ≥1); therefore, they were used for further analysis. The Jadad average score was 1.70 ± 0.95 (Table 1). Figure 2 and Table 2 present the risk of bias summary capturing the reviewers' judgments about each item and percentages across all included trials.
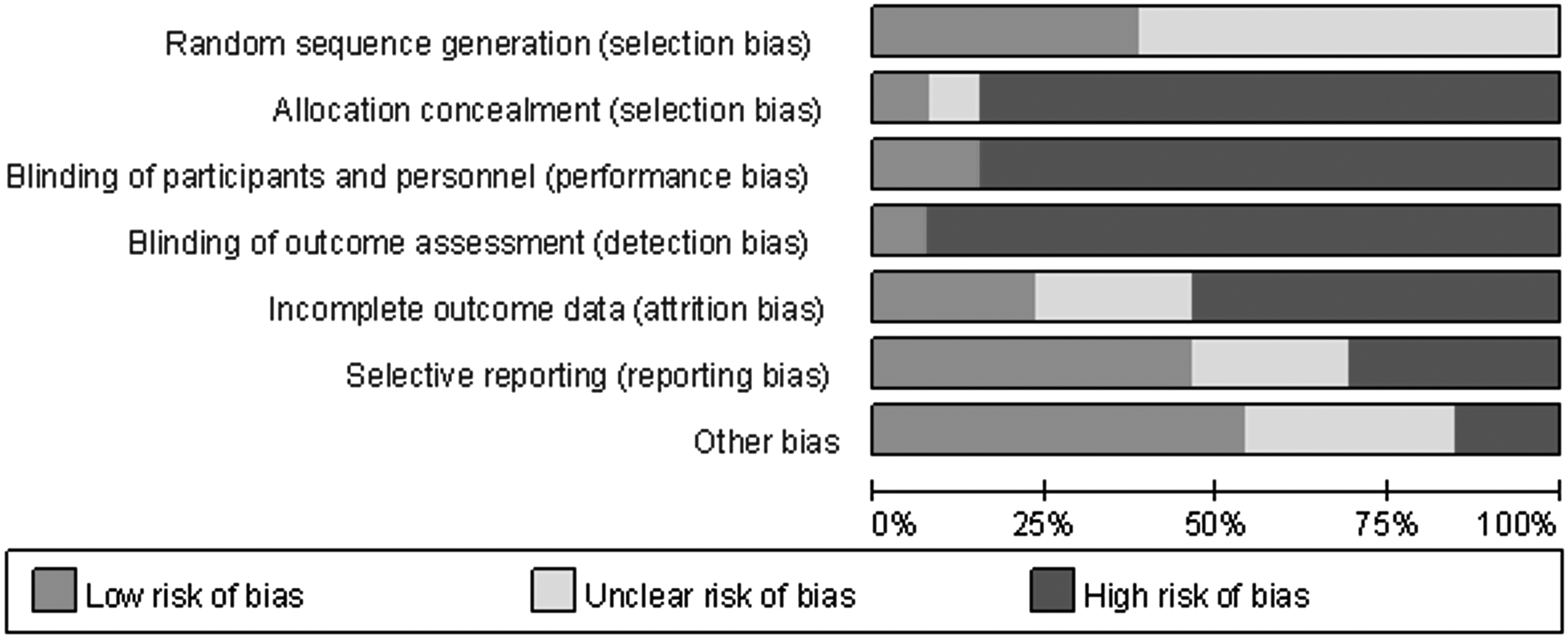
Risk of bias summary for bias within included studies.
H, high risk of bias; L, low risk of bias; U, uncertain risk of bias.
Effects of acupuncture-related techniques of acupoint stimulation
Pairwise meta-analysis
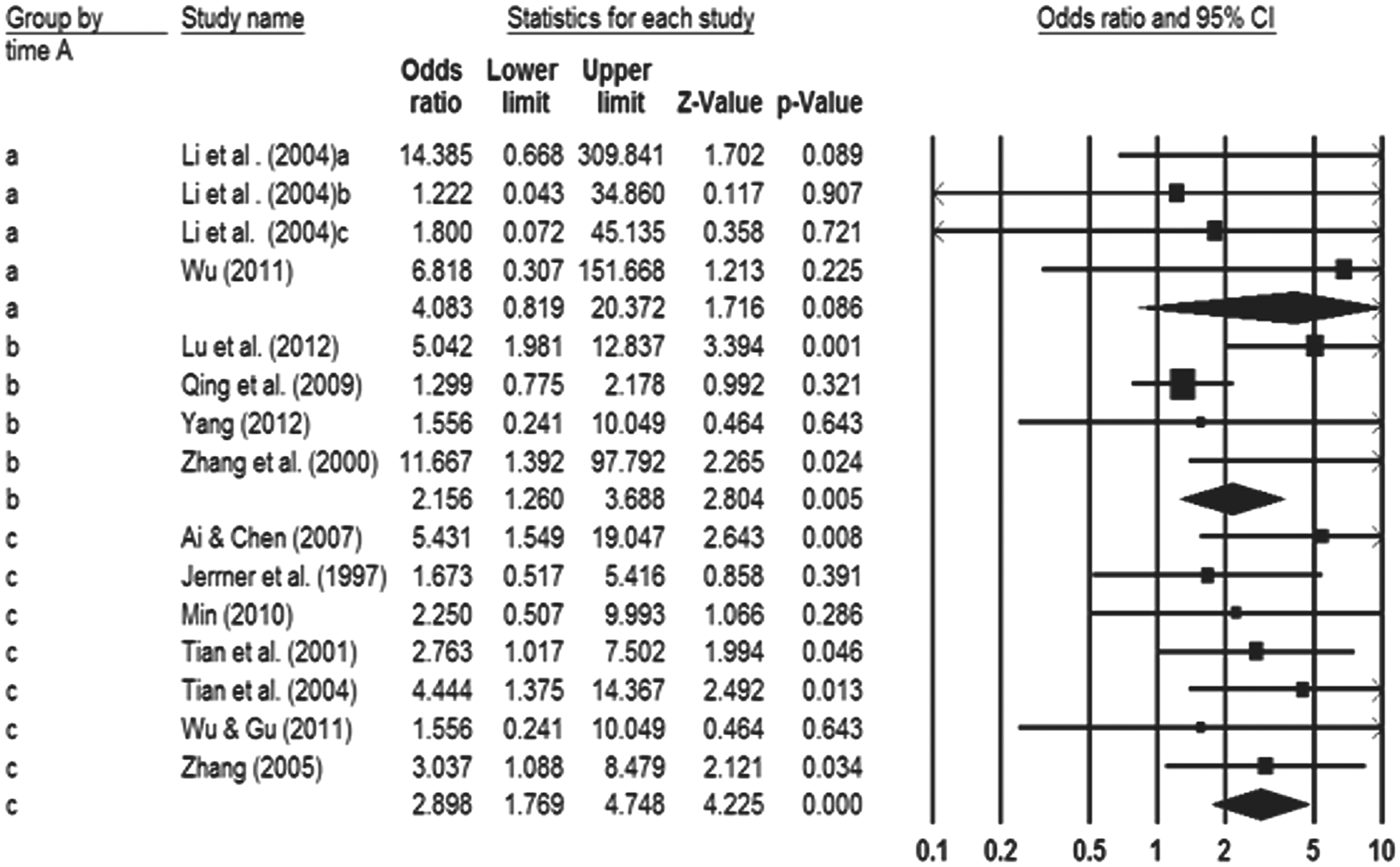
Figure 3 shows the meta-analysis results for the selected outcome. The effective rate (13 RCTs, 1,051 participants) indicated no evidence of heterogeneity (Q = 15.64, p = 0.34, I 2 = 10.50%). A visual inspection of the funnel plots (not shown) and Egger's test for asymmetry did not show significant differences (t = 1.92, SE = 0.51, p = 0.08). Pooling all data using a random effects model yielded a significant difference between the acupoint and nonacupoint stimulation (OR = 2.57, 95% CI 1.81–3.65). To determine whether methodological quality adversely affected the validity, a subgroup analysis was conducted. The studies were classified into three groups on the basis of the Jadad score. Figure 4 presents the heterogeneity and the total effective rate for the four groups: score 1 (a; Q = 6.93, p = 0.32, I 2 = 13.83%; publication bias p = 0.04; OR = 2.08, 95% CI 1.31–3.31, p = 0.002), score 2 (b; Q = 2.62, p = 0.76, I 2 = 0%; publication bias p = 0.51; OR = 3.90, 95% CI 1.90–8.00, p < 0.001), and score 3–4 (c; Q = 2.08, p = 0.15, I 2 = 51.82%; OR = 3.08, 95% CI 1.05–9.03, p = 0.04).
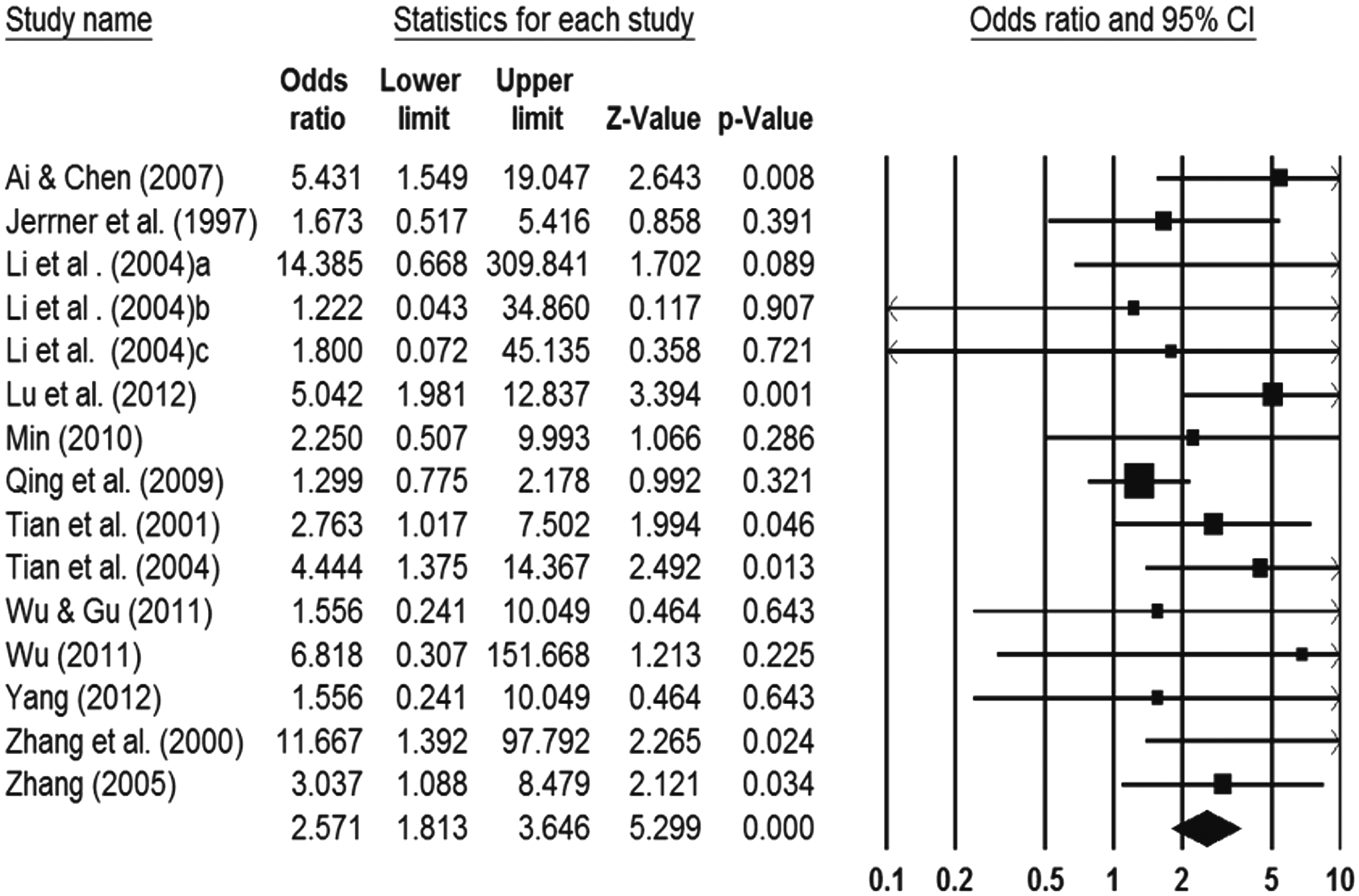
Effect sizes for 13 studies on the effective rate.

Effect sizes of time points for 13 studies on effective rate. The studies were grouped by Jadad score. The diamond shapes represent pooled effect size for “a” as score 1, for “b” as score 2, and for “c” as score 3–4.
Among the included studies, five reported adverse events, one reported no adverse events, 28 and only one reported the number of adverse events. 41 Calculating the number of participants was not feasible; hence, the number of occurrences was calculated. As shown in Table 3, 77 participants presented with 106 adverse events (13.2% occurring in the acupoint stimulation groups and 86.8% in the control groups). The overall incidence of adverse events was 5.4% (15/278) and 28.6% (63/220) in the acupoint stimulation and control groups, respectively. The most frequent adverse event was fever (n = 8) in the acupoint stimulation group and dry skin with itching (n = 42) in the control group.
To obtain additional insight into the summary effect, a subgroup analysis was used to determine the effects of intervention duration (1, 2, and 3 months) on outcomes and the differences in the time point effects. The duration of intervention was grouped into three subgroups. Figure 5 presents the results of the heterogeneity and effective rate for the groups 2–4 weeks (a; Q = 1.50, p = 0.68, I 2 = 0%; publication bias p = 0.05; OR = 4.08, 95% CI 0.82–20.37), 6–8 weeks (b; Q = 9.11, p = 0.03, I 2 = 67.08%, publication bias p = 0.33; OR = 2.16, 95% CI 1.26–3.69), and 12–18 weeks (c; Q = 2.87, p = 0.83, I 2 = 0%; publication bias p = 0.51; OR = 2.90, 95% CI 1.77–4.75).
Effect sizes of time points for 13 studies on effective rate. The studies were grouped by intervention duration. The diamond shapes represent pooled effect size for “a” as 2–4 weeks, for “b” as 6–8 weeks, and for “c” as 12–18 weeks.
In addition, acupuncture-related techniques were grouped as multiple and single techniques. Figure 6 shows the results of the heterogeneity and cure rate for the multiple techniques group (Q = 12.87, p = 0.12, I 2 = 37.83%; publication bias p = 0.08; OR = 2.62, 95% CI 1.57–4.39, p < 0.001) and the single technique group (Q = 1.57, p = 0.90, I 2 = 0%; publication bias p = 0.60; OR = 3.29, 95% CI 1.71–6.34, p = 0.001).
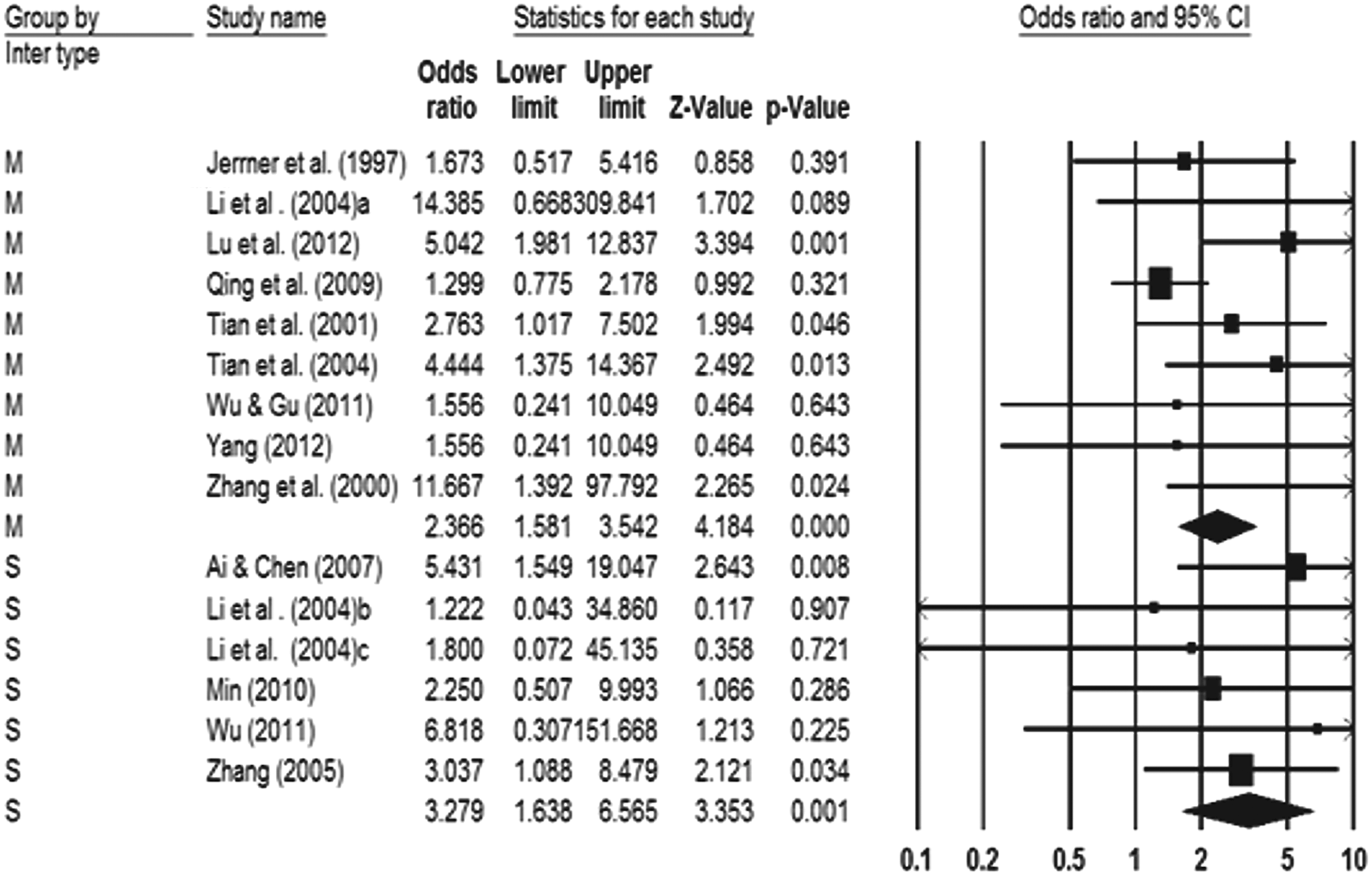
Effect sizes of types of acupuncture-related techniques for 13 studies on effective rate. The studies were grouped by interventions. The diamond shapes represent pooled effect size for “M” as a multiple technique and for “S” as a single technique.
Network meta-analyses
To analyze network meta-analysis of acupuncture-related techniques, a hypothesized model, including acupuncture, acupressure, acupoint bloodletting, and acupoint catgut embedding, Chinese herbal medicine, and narrow-band ultraviolet B, alone or combined (Fig. 7, 10 RCTs, 869 participants), was developed. For analyses of the included 10 RCTs, a contrast-based parameterization was used. Consistency between indirect and direct evidences was tested by comparing the results of pairwise comparisons with those of the network meta-analysis. No significant inconsistency (p > 0.05) was observed, indicating good coherence between direct and indirect comparisons in the side splitting analysis. Table 4 shows the consistency model with pooled OR for the treatment effect. Compared with medication, acupressure (OR = 1.62, 95% Cr 0.30–2.94) and acupoint catgut embedding (OR = 1.17, 95% credible interval [cr.] 0.35–1.99) significantly improved psoriasis. The estimated ranking probabilities, based on the effective rate, indicated that acupressure was most effective in treating psoriasis.
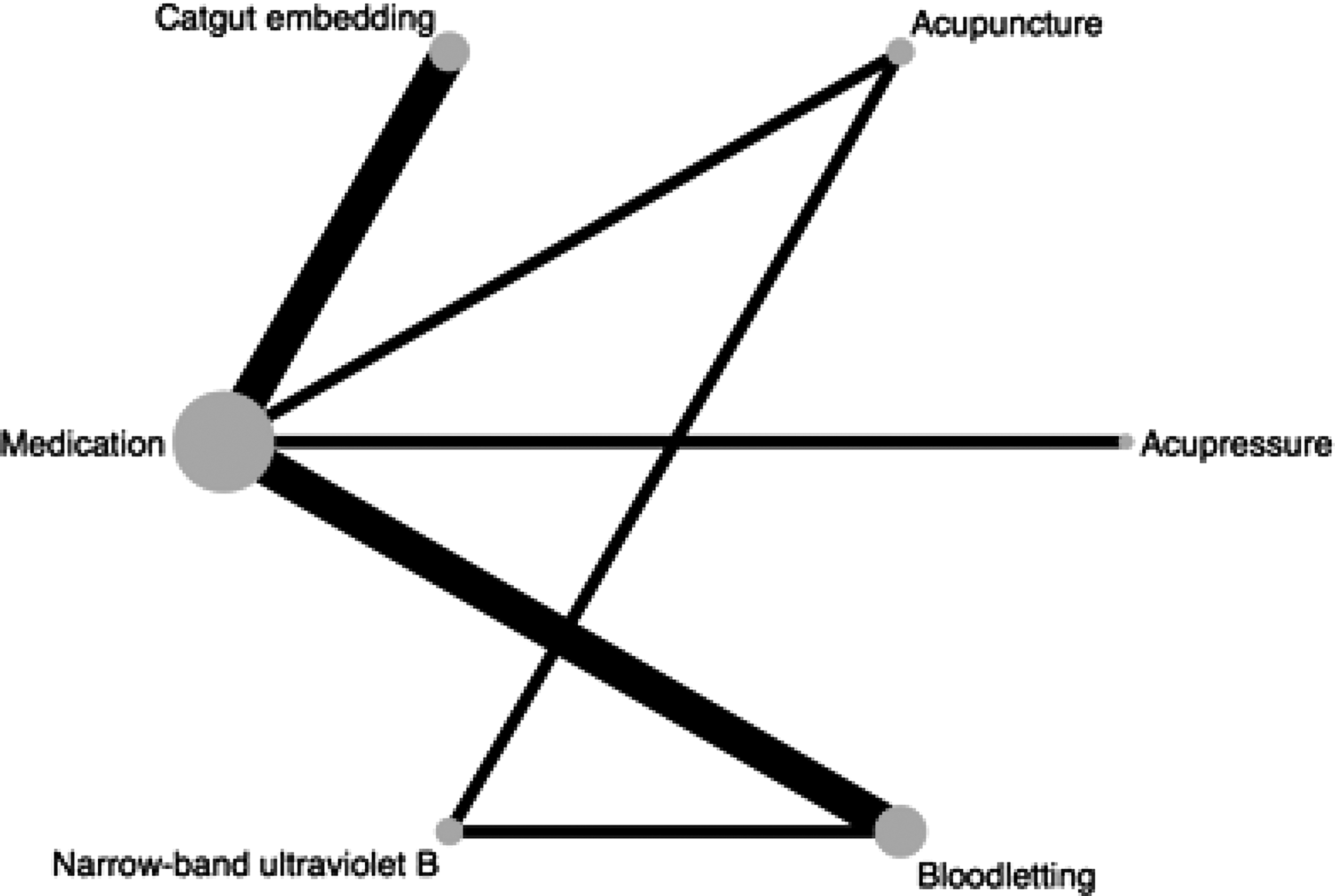
Model of network formed by acupuncture-related techniques and their direct comparisons. The lines between nodes indicate the direct comparison made within RCTs. The width of the lines is proportional to the number of trials comparing each pair of treatments. RCT, randomized controlled trial.
Numbers in parentheses indicate the 95% credible interval.
Discussion
Various acupuncture-related techniques are used in TCM, alone or in combination, to treat psoriasis. Acupuncture has the advantages of safety, reliability, efficacy, and ease of operation. Although acupoint stimulation using different acupuncture-related techniques has been used to treat psoriasis, its therapeutic effects remain unclear. The findings of this systematic review and traditional pairwise meta-analysis study of RCT support the notion that therapeutic effect of acupoint stimulation (including acupuncture, acupressure, catgut embedding, bloodletting, injection, electrostimulation, and moxibustion) is superior to that of nonacupoint stimulation in treating psoriasis. However, the included RCTs differed in their session duration, the acupoints, and the number of acupoints, complicating the comparison of acupuncture-related techniques in patients with psoriasis. Our subgroup analyses confirmed the effects in groups with various Jadad scores, treatment durations, and different acupuncture-related techniques.
Results of this study evidenced that the treatment effect of short-term treatment for psoriasis is superior to that of long-term treatment. Acupuncture-related techniques rely on the concept and practice of TCM stimulating particular acupoints. Thus, the clinical effect of acupuncture accumulated over multiple treatments and gradually extended beyond the length of each treatment session. 42,43 During short-term treatment, acupuncture may have modulated similar networks as placebo, but it exerted prolonged effects on specific brain areas after multiple treatments. 44 However, psoriasis is a chronic, relapsing skin disease with no proven cure. Psoriasis-affected skin commonly becomes resistant to continuous drug treatments over time. Treatment may be switched periodically, say every 12 to 24 months, if it is ineffective or causes adverse reactions. These meta-analyses indicated that acupoint stimulation quickly and effectively improved psoriasis. Only four included studies involved follow-up after their interventions, 41,45 –47 and the follow-up periods ranged from 6 months to 2 years. Additional studies on the sustaining treatment effect of acupoint stimulation are warranted.
This study confirmed that both single and multiple acupuncture-related techniques are effective for treating psoriasis. Furthermore, acupuncture-related techniques were categorized into acupuncture combined with narrow-band ultraviolet B phototherapy 31 or moxibustion, 48 acupressure, 28 acupoint bloodletting combined, 29,46,49,50 and acupoint catgut embedding. 41,45,47 In terms of both the direct and indirect effects of the network meta-analysis in this study, acupressure and acupoint catgut embedding were significantly more effective in the treatment of psoriasis than was medication. This study identified that acupressure is the most effective treatment for psoriasis.
The finding that acupressure is the most effective treatment for psoriasis is based on one included study 28 and the result of the network meta-analysis in this study. Acupressure refers to the application of needleless pressure on acupoints 27 and can be used alone or in combination with other acupuncture-related techniques for treating psoriasis. 17 Each acupressure treatment period for an episode of psoriasis lasts ∼2–8 weeks, wherein a certain acupoint is repeatedly pressed in each session. 28 Compared with other acupuncture-related techniques, acupressure is safer and has fewer side effects, such as local trauma; in addition, it is simple and has higher patient acceptance and compliance. 51,52
Acupoint catgut embedding presented its treatment effect after pooling three studies with increasing the sample sizes. The acupoint catgut embedding therapy used catgut, a type of cord made from the natural fiber in the walls of sheep or goat intestines. It is embedded on the acupoint and provides stimulation for 7–14 days. 29 The catgut is gradually completely absorbed by the body and hence, it is less painful, easy to absorb, and safe. This technique aids scientific decision making of clinical treatment, particularly in dermatology, and has an effective rate of more than 90%; psoriasis of the dermatological clinic is considered as the dominant disease of acupoint catgut embedding therapy. 53
In this study, six included RCTs reported adverse events 29,31,41,46,48 and one reported no adverse event of acupressure, 28 whereas the others did not address adverse events. 22,32,45,49,50,54 Among the adverse events, 14 out of 106 events were fever, pain, and dizziness caused by catgut embedding 47,53 and bloodletting 29,46 in experimental groups. Eight participants received acupoint catgut embedding and experienced mild fever for 2 to 3 days, but no further treatment was needed 47 ; 86.8% of the adverse events were found in the control groups. The common adverse events in the medication groups were dry skin, 29 desquamation and itching, 46,48 thirst, and dry mouth. 46,48 The findings of this study indicate that acupoint stimulation is safe and has few adverse events. Acupuncture-related techniques usually do not cause serious side effects, unlike those from adverse drug reactions. 30
The included RCTs in this study appeared to have methodological weakness because the Jadad score was low and because the risk of bias was unclear or high particularly to blinding. Among methodological difficulties, achieving therapist and participant blinding from acupuncture is difficult; only two included RCTs achieved adequate blinding. 22,28 These two studies had low-risk bias and reported the positive results for the effectiveness of acupuncture. The results of this study confirm that both auricular acupuncture and auricular acupressure are effective for treating psoriasis. One study randomized participants to receive acupuncture or minimal acupuncture as comparator and reported the efficacy after the 10-week psoriasis treatment. 22 However, this efficacy of psoriasis treatment was not sustained for more than 3 months. 22 Another study randomly assigned participants to receive acupuncture combined with medication or take medication alone and reported treatment efficacy after an 8-week therapy. 28
A preponderance of positive results was observed in this study. However, a placebo-controlled, double-blind trial of acupuncture is technically impossible. 55 Blinding patients and therapists is particularly difficult. One of the critical concerns to design acupuncture-related techniques research is that no standard placebo is currently available. This study recommends blinding the independent outcome assessor to the experimental intervention in the main study. 56
Limitations
This study has several limitations. First, the conclusion is limited to Chinese and English language articles. Other relevant trials may have been identified if this study had searched the literature in other languages. Second, considerable variation was observed across trials in the age of participants (18–77 years), treatment methods, clinical conditions, treatment periods ranging from 2 to 18 weeks, and follow-up durations ranging from 2 weeks to 2 years. Finally, the lack of allocation concealment and blinding was observed in the included studies.
Conclusions
Acupoint stimulation with acupuncture-related techniques was found to be more effective than nonacupoint stimulation in treating psoriasis. The use of acupuncture-related techniques for acupoint stimulation can be considered an alternative or adjuvant therapy for psoriasis with a short-term treatment effect, particularly acupressure. The acupuncture-related techniques should be applied for at least 6 weeks to achieve therapeutic effect. Catgut embedding on acupoint has a long-term treatment effect in addition to its short-term effect. Additional studies are warranted to confirm the long-term effect of acupressure. In addition, because the methodological quality of included studies was not rigorous, a cause–effect inference may be limited by no or unclear reporting of allocation concealment, blinding, and attrition. We suggest that future trials follow the guidelines of Consolidated Standards of Reporting Trials, which allow a comprehensive assessment of the methodological quality. To provide more valid treatment effect of acupoint stimulation, further designing head-to-head trials for comparing specific acupuncture-related techniques to current standards of care for psoriasis are also necessary to address issues related to a consensus protocol of acupuncture-related techniques for treatment periods of psoriasis, and outcome measures with multiple endpoints and follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.