
Abstract
Objective:
Religion, spirituality, and health are inseparable in human history. Yet, the effects of religion and spirituality on health are controversial. The objective of this study was to investigate the effects of praise dance on the quality of life (QoL) of women with or without medically diagnosed diseases.
Method:
This was a pretest–posttest study with one convenience sample that took place at Praise Dance Association Hong Kong (PDA) centers. Two hundred and fifty-six Chinese adult females participated. They were aged ≥45 years and had joined the PDA centers within 4 weeks of the commencement of this study. The intervention lasted for 12 weeks, and the subjects practiced praise dance three times a week in a group with a coach in the first four weeks and subsequently on their own or with the same group at least once a week. Each dancing session lasted for 30 min. The subjects completed the World Health Organization Quality of Life (WHOQOL)-BREF (HK) questionnaire before and after the intervention of the praise dance.
Results:
The findings showed significant improvement in the psychological well-being of the participants, regardless of their religious background. The improvement in their physical domain was statistically marginal.
Conclusion:
This is the first empirical study to test the benefit of praise dance on QoL. Promoting praise dance could be beneficial to the psychological well-being of women, regardless of their religious backgrounds. The effect of religion or spirituality on QoL warrants further investigation.
Introduction
D
With the development of empirical science in the West in the Middle Ages, religion, spirituality, and health have split. Health has been taken care of by medicine, which uses empirical evidence, while religion and spirituality have remained part of people's belief in God and supernatural power, which are related to hope, faith, and connectedness. 3 With the advancement in medical science and globalization, concepts of and attitude toward religion and spirituality are frequently challenged by non-believers and atheists. However, this phenomenon has not occurred in Eastern culture. This is probably because spirituality in the East is more influenced by the tenets of Confucianism, Daoism, and Buddhism. 4 In addition to faith, hope, and connectedness, the fulfillment of personal responsibilities (being a good person) and acceptance of death as a life process (letting go and living in harmony with nature and self, and having a sense of peace) are related to spirituality, especially for Chinese people. 5 Moreover, the theory of yin and yang from Daoism in China has strongly influenced the view of health and illness in Chinese culture, and forms the foundation for Chinese medicine. 6 Spiritual well-being has been reported to have positive influence on health-related quality of life (QoL). 7 –9 In Hong Kong, around 14% of people follow Buddhism and >14% follow Daoism. About 12% of the population are Christians, comprising mainly of Protestants and Catholics. 10 Does religion or spirituality have an impact on health in such a way as to affect the management of health conditions? The effects of religion and spirituality on health are nevertheless controversial.
Theories about the dancing body are often developed in a metaphysical way. 11,12 Dance may improve the well-being and healing process of people through physiological processes, as well as increasing individuals' sense of control through possession of spirit in dance, mastery of movement, relief from stress or pain, and facing stressors and handling their effects. 13 Evidence supports that dance could improve physical fitness and strength, reduce pain, develop social skills, and enhance mental health (e.g., increase self-esteem and promote positive mood) and QoL. 14 –16 Posture has been found to be a powerful tool in expressing and recognizing emotions and giving insights into their unconsciousness. 17,18 Therefore, dance has become a therapeutic tool in recent decades, and is defined as “the psychotherapeutic use of movement to further the emotional, cognitive, physical, and social integration of the individual” according to the American Dance Therapy Association. 19 Recent meta-analysis and systematic reviews concluded that dance therapy could improve QoL, mood, affect, subjective well-being, and body image, and decrease depression and anxiety. 20,21 In a nutshell, dance could be an important strategy to promote psychological QoL. Praise dance is a form of dance that praises and gives thanks to God. 22 Despite being co-extensive with much of the 20th century's Western dance literature, the study of praise dance, however, has remained somewhat limited and basic in its theoretical enquiry and analysis. 23
Nonetheless, based on the limited literatures, praise dance is linked to spiritual benefits for the dancers. 21 Through rhythmical movements, the dancers release energy and lift up their spirit while experiencing a kinesthetic awareness of their body. Praise dance allows people to feel the power source within their own soul through an awareness of their body, to have a personal relationship with God, to let go of their inner feelings in this form of worship and praise, and to become more aware of their spirituality. 21 What makes praise dance potentially more beneficial is that it may work for people both with or without a Christian background. 22 Praise dance educators argue that no matter what faith tradition people follow, the dance creates a community where people come and practice together in a common space and at a common time. Such a community brings energy and spirit when people come together to move and dance, sing and praise, and pray and thank God. 22
Dance educators have also discussed the health benefits of praise dance. The dance is thought to elicit wonder, compassion, wisdom, and wholeness on both esthetic and spiritual levels. 24,25 Through the search for wholeness, wisdom, and the sacred, the dance as a form of meditation unites the body, mind, and spirit. 24 The somatic movements that signify a physical meditative practice offer a way to heal the deepest and most meaningful part of people. 25 As the dance honors inner sensation and knowing, the dancers are asked to go inside and make decisions on what is healthy and what will lead them to wholeness and happiness through the dancing approach. Such a process often leads to unintentional therapeutic effects for the dancers. 26
However, until now no studies have put the health effects of praise dance to the test. The present study intended to examine the health benefits that praise dance could bring to Christian believers as well as to non-Christians in a community sample. Specifically, the potential health benefits were examined in terms of QoL after practicing praise dance for 12 weeks. The therapeutic effects of praise dance were also compared for people with different health conditions (i.e., as measured by the number of medically diagnosed diseases) and religions (i.e., Christian vs. non-Christian). Additionally, all these factors were taken into consideration, and the study tested whether there were any interaction effects between the factors.
Materials and Methods
Procedure
The Praise Dance Association Hong Kong (PDA) has around 300 centers/platforms across all 18 districts in Hong Kong to organize community-based praise dance sessions. The study was a pretest–posttest design with one convenience sample. The praise dance program was promoted by putting up recruitment posters in the PDA centers. Adults who were interested in joining the program could enroll. The researchers invited eligible adults who had registered on the program to participate in the study, and obtained their signed consent for doing so. A self-administered World Health Organization Quality of Life (WHOQOL)-BREF (HK) 27 with demographic, health history, and life-style information was completed as the baseline measure of their QoL before starting the praise dance program. All subjects practiced praise dance for 12 weeks. At the end of the 12th week, after the subjects had participated in the present study, they completed the WHOQOL-BREF (HK) again as the post-test measure of their QoL. Ethical approval was sought and obtained from Tung Wah College, Hong Kong.
Participants
The target population for the study was PDA members. Most of them were full-time housewives at their late middle age with grown-up children and were free from child-rearing chores during the day (M. Chung, pers. commun., June 4, 2015). Therefore, the inclusion criteria for the convenience sample were (1) female, (2) aged ≥45 years, (3) able to understand Chinese, (4) physically fit for aerobic exercise, and (5) joined the PDA within 4 weeks of the commencement of this study. Adults who were pregnant, and who had a physical disability, any contraindication to exercise, a terminal illness, and/or dementia were excluded. Two hundred and fifty-six Chinese women were included in this study.
Intervention
The praise dance program comprised 36 sessions, three times a week (12 weeks in total). Each dancing session lasted for 30 min. The subjects learned seven praise dance songs in groups with a coach in the first four sessions. In the ensuing eight sessions, the subjects practiced all seven praise dance songs in groups with a coach in the PDA centers. For the remaining weeks of the program, they could choose to practice the seven songs on their own or in groups (Table 1). The songs were about the power of God and Christ. All subjects followed the standard praise dance training plan designed by PDA experts to ensure consistency of movements, duration, intensity, and frequency of the dance among all subjects. The standard training plan was provided to the subjects at the beginning of the program.
PDA, Praise Dance Association Hong Kong.
Measures
The WHOQOL-BREF (HK) was used to assess subjects' QoL. This questionnaire is composed of four subscales: physical, psychological, social, and environmental. 27 This questionnaire was modified to suit the Cantonese-speaking population. 28 As a result, two cultural-specific questions were added to the questionnaire: “To what extent do you feel other people accept you?” and “How easy is it for you to eat the food you desire?” The WHOQOL-BREF (HK) has satisfactory psychometric properties, with Cronbach's alphas of 0.77 (physical), 0.78 (psychological), 0.59 (social), and 0.76 (environmental), and excellent test–retest reliability (range 0.80–0.91). 27
The questionnaire also collected demographic information (age, marital status, education, monthly income, etc.), religion, and medical history (12 medically diagnosed diseases such as diabetes, asthma, cardiovascular disease, heart failure, chronic respiratory disease, thyroid, liver and kidney diseases, rheumatism, arthritis, osteoporosis, and cancer). Three-quarters of the participants were Christians, while 2.7% and 0.8% were Buddhists and Catholics, respectively; the remaining participants had no religion. The participants were then grouped into Christians and non-Christians. The number of medically diagnosed diseases was defined as none, one, and two or more.
Data analysis
Two hundred and fifty-six eligible participants were included in the analysis. To examine the change in the four domains of QoL after the intervention of praise dance, a paired t-test was performed. A repeated-measures analysis of variance was performed using general linear models in order to investigate the effects of praise dance on the four domains of QoL, and this was varied by religion (Christian belief in this case) and the number of diseases. All analyses were conducted using IBM SPSS Statistics for Windows v22 (IBM Corp., Armonk, NY).
Results
The mean age of the 256 Chinese females was 57.6 years (SD = 7.6 years; range 45–74 years; Table 2). The majority of the women (74.2%) were married. Three-quarters of the participants completed either secondary education (57%) or undergraduate degrees or higher (17%). As regards monthly income, 38%, 18%, and 5% of the participants earned $10,000–29,999, $30,000–59,999, and ≥$60,000, respectively. The majority (74.2%) were Christians. About half (57%) of the women had no medically diagnosed disease, while the others had one (34%) or more than one (9%) forms of chronic diseases.
HKD, Hong Kong dollar; M, the mean.
After participating in praise dance, all domain scores increased (Table 3). However, only the improvement in the psychological domain was significant (p < 0.001). It is worth noting that the improvement in the physical domain of QoL was marginally significant (p = 0.06).
WHOQOL-BREF, World Health Organization Quality of Life.
To investigate whether the benefit of praise dance would vary by (1) religion and (2) health status, general linear models were used. There were no significant interactions of (1) religion (Christians vs. non-Christians) or (2) health status (number of medically diagnosed diseases) with the benefit of praise dance (Table 4).
The three-way interaction of religion, health status, and the effects of praise dance were also examined. There were no significant interactions for all of the four domains (p > 0.05). However, the scores of the four domains decreased over time among the non-Christian women who had two or more diseases diagnosed, whereas the scores increased or remained unchanged in the other groups (Figs. 1 –4).
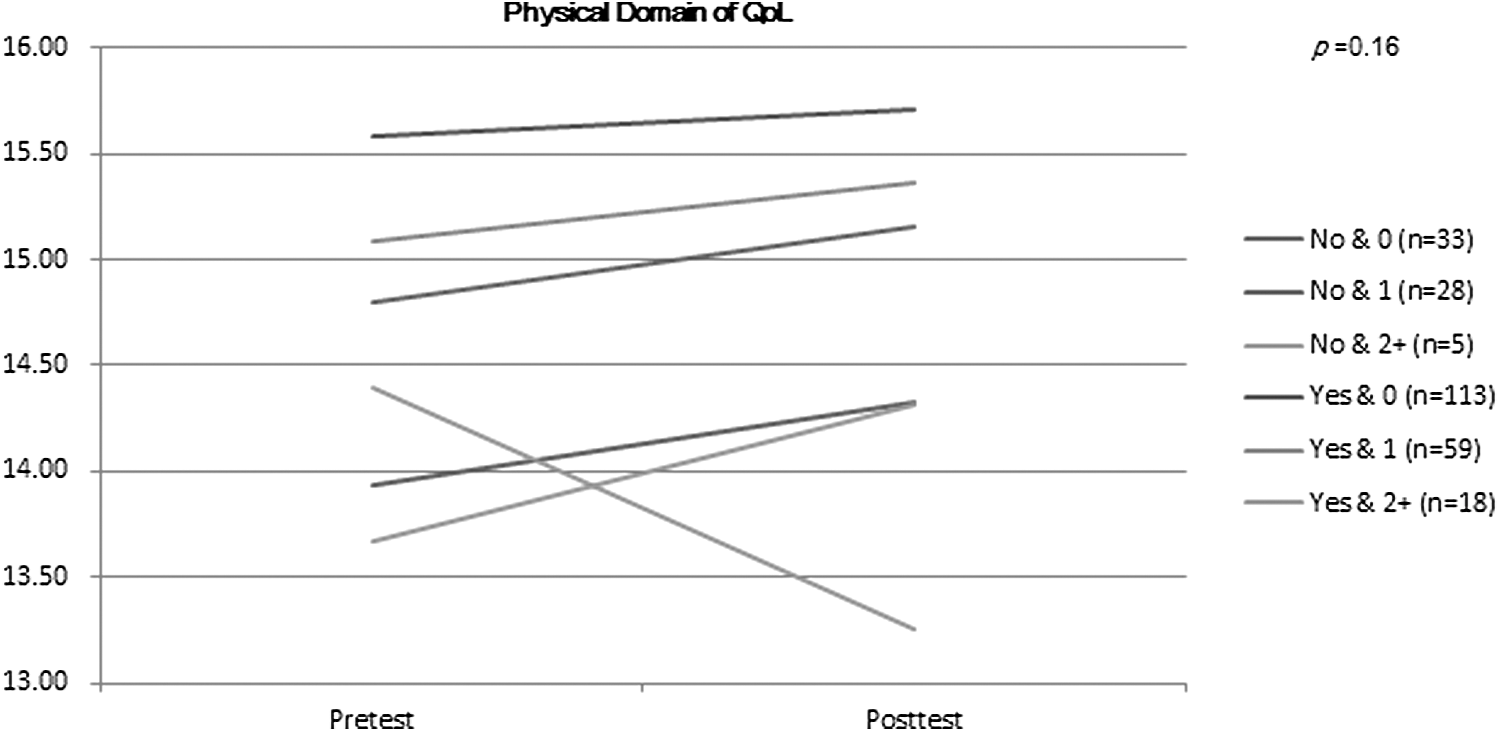
Mean plots of the interaction effects between health status and religion on physical quality of life (QoL) improvement. Yes, Christian; No, non-Christian; 0, no disease; 1, one disease; 2, two or more diseases.
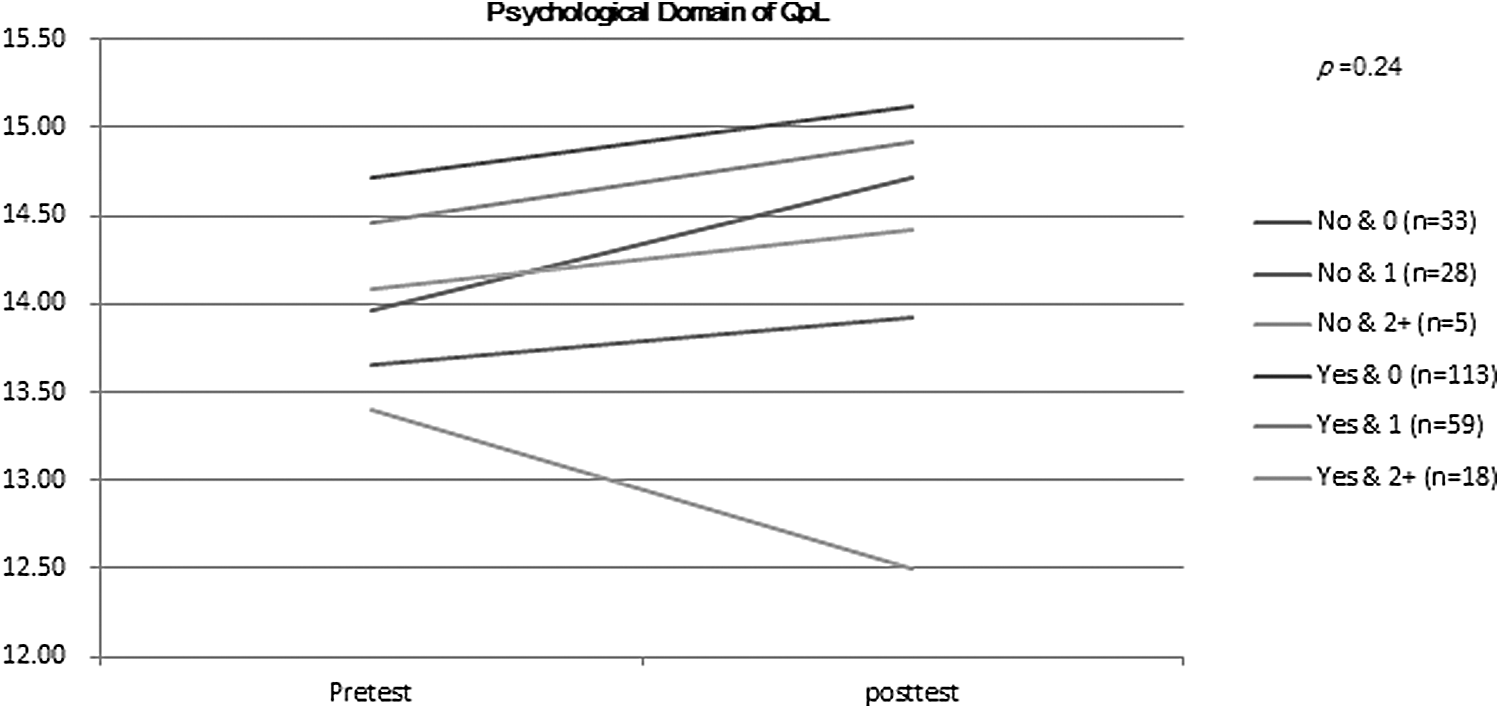
Mean plots of the interaction effects between health status and religion on psychological QoL improvement. Yes, Christian; No, non-Christian; 0, no disease; 1, one disease; 2, two or more diseases.
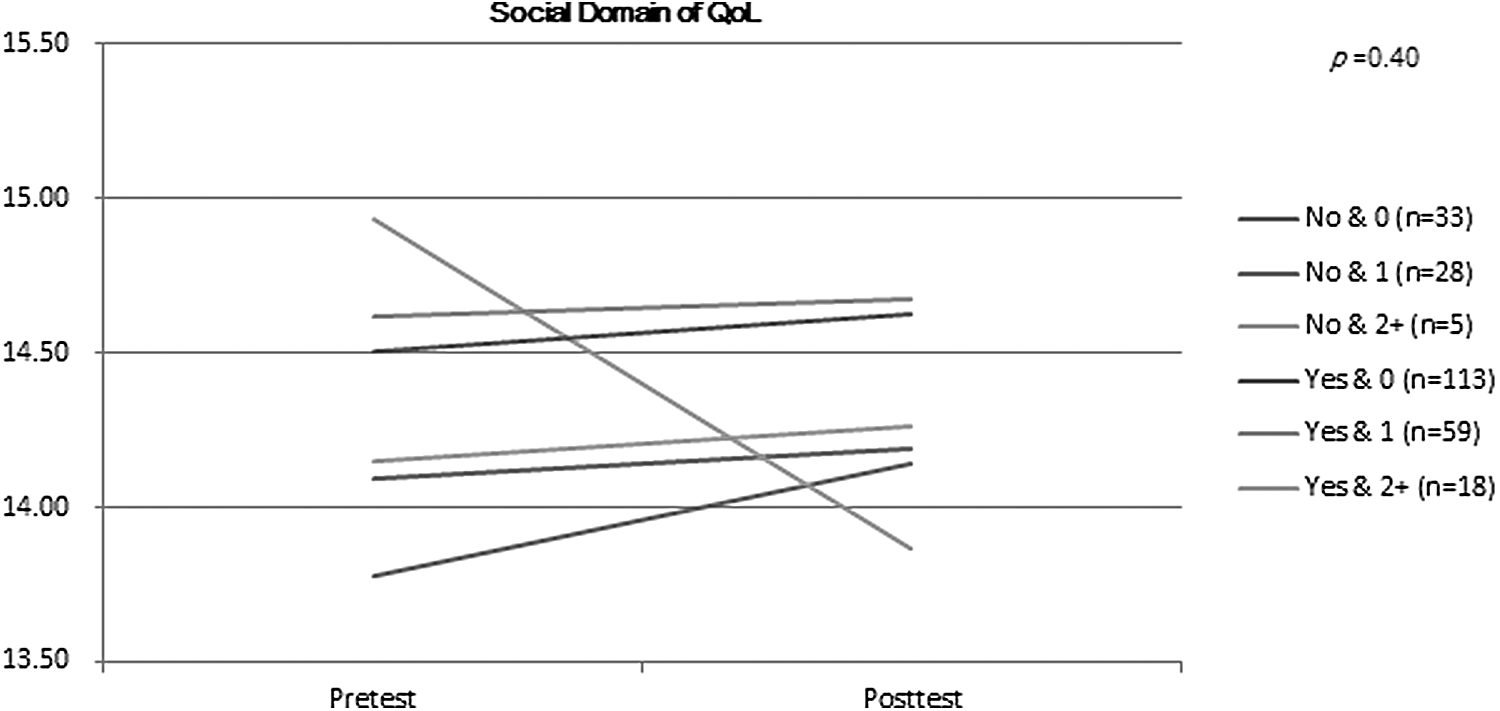
Mean plots of the interaction effects between health status and religion on social QoL improvement. Yes, Christian; No, non-Christian; 0, no disease; 1, one disease; 2, two or more diseases.
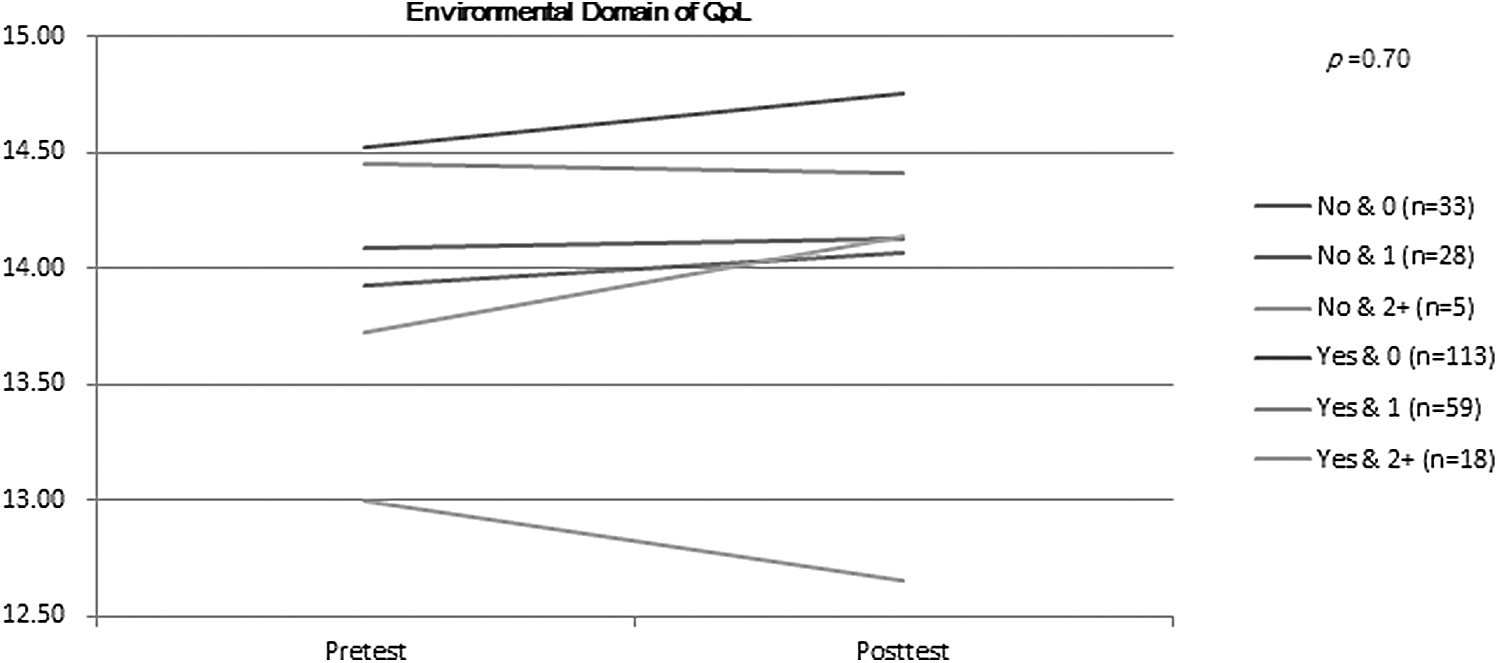
Mean plots of the interaction effects between health status and religion on environmental QoL improvement. Yes, Christian; No, non-Christian; 0, no disease; 1, one disease; 2, two or more diseases.
Discussion
The literature has suggested that praise dance can bring both mental and physical health benefits to participants, regardless of their religious background. 24 –26 However, empirical studies have seldom put these assertions to the test. This study was the first known attempt to test the health benefits of praise dance. Although there is substantial evidence to support the physical, psychological, and social benefits of dance (e.g., Western dance, aerobic dance, and dance therapy), 14 –16,19 –21 the results of this study demonstrated that after practicing praise dance, the participants showed a significant improvement in the psychological domain of their QoL, whereas the improvement in the physical domain was marginally significant.
Apart from the beneficial effects of the dance, which is a physical activity in itself, on health-related QoL, 29 –32 praise dance might have enhanced spirituality, which, in turn, improved the participants' psychological and physical well-being, 33,34 regardless of the participants' religious backgrounds. Spirituality and religion are correlated but yet discrete constructs. 2 Spirituality focuses more on the meaning and purpose of life, transcendence, harmony with the universe, and values, whereas religion focuses more on the system of attitudes and beliefs. 35 However, only one item measured religion but not spirituality. Participants could not be classified as (1) no religion but high spirituality, (2) no religion and low spirituality, (3) Christian but low spirituality, or (4) Christian and high spirituality, and hence, the difference in the change in spirituality during the intervention and its effects on quality of health among such groups could not be ascertained. Hence, no analysis could be performed to confirm whether the change in spirituality explains the change in QoL.
Further analysis was performed to examine whether the effects of praise dance would vary in accordance with the participants' religion and health status. The findings suggested that praise dance's effects may differ among Christian and non-Christian women and with the different number of diseases. In general, the scores of all four QoL domains decreased over time among the non-Christian women with two diseases or more, whereas the four scores increased or remained unchanged for the rest of the women, including Christian women with two diseases or more. This interaction effect was insignificant, probably due to the small subgroup size of the non-Christians with two diseases or more (n = 5) in the group. Greater beneficial effects might be found in Christians than in non-Christians with more diseases possibly because the Christian might anchor greater hope on something that they believed in (e.g., God) and accept death as a life process. Further studies are needed to confirm whether the beneficial effects of praise dance vary according to religion and health status.
The limitations of the present study include that there was no control group, and that there were no attendance records to examine the potential explanation on the low beneficial effects of praise dance in the non-Christians with two diseases or more. Therefore, an analysis of the dose–response relationship between praise dance and psychological QoL was not possible. Moreover, a convenience sample was recruited from the PDA but not from the general population. This special target population might benefit more from the praise dance intervention than the general population would. Since no measurement could be made of spirituality, the change in the effect of praise dance on spirituality and hence on QoL among religious and spiritual groups (e.g., no religion but high spirituality vs. no religion and low spirituality vs. Christian but low spirituality vs. Christian and high spirituality) could not be assessed. No analysis could be performed to confirm whether the change in spirituality explains the change in the QoL. Nonetheless, the present study is the first empirical study to investigate the effects of praise dance on health-related QoL. Future studies should confirm the findings with a more rigorous study design and sample (e.g., randomized control trial) and more detailed instruments (e.g., including assessment on the level of adherence to the program, spirituality, and religion). Given that spirituality and religion are correlated but discrete constructs, it is worthwhile assessing whether the effects of praise dance on QoL vary (e.g., no religion but high spirituality vs. no religion and low spirituality vs. Christian but low spirituality vs. Christian and high spirituality). Future studies should consider assessing whether the effect of praise dance on QoL is explained by spirituality.
In conclusion, praise dance could be beneficial to the psychological well-being of women, regardless of their religious backgrounds. Promoting praise dance could be a useful strategy to improve the psychological well-being of women.
Footnotes
Acknowledgments
We would like to thank the staff of the Praise Dance Association Hong Kong for their generous support of this research project. We also thank the Praise Dance Association Hong Kong for its kind permission to allow us to conduct this research project, and its cooperation to enable the research to be carried out smoothly. Finally, we thank all of the participants for taking the time to complete our survey.
Author Disclosure Statement
The authors have no commercial interest in the non-profit-making PDA, and they have no conflicts of interest to declare.