
Abstract
Background/Objective:
Sasang constitutional medicine is a component of traditional Korean medicine that classifies individuals into four Sasang constitutional types (SCTs) by their physical and psychological traits. Each SCT is known to show different susceptibilities to disorders. This systematic review investigated the effect of SCT as a risk factor for various disorders.
Methods:
A systematic literature survey was conducted by searching seven databases for all articles on the prevalence rates of disorders according to SCT and sex.
Results:
From 14,272 relevant articles, 15 studies (13 disorders) were ultimately identified to verify different prevalence rates by SCT. Of the 13 disorders, 6 (prehypertension, general obesity, abdominal obesity, metabolic syndrome, diabetes mellitus, and irritable bowel syndrome [IBS]) had a significantly different prevalence by SCT. Metabolic syndrome and its associated disorders showed the highest prevalence in Taeumin-type individuals, whereas IBS was most prevalent in Soeumin-type individuals. In general, these findings were consistent with the results obtained in an analysis of male and female participants.
Conclusions:
This study revealed that susceptibility to disorders was affected by SCT to some extent. Further studies are needed to determine the concrete features of SCT-related susceptibility, which may be helpful in preventive medicine with Sasang constitutional practice.
Introduction
G
SCM, a branch of traditional Korean medicine, categorizes individuals into four constitutional types: Taeumin (TE), Soeumin (SE), Soyangin (SY), and Tayangin (TY). Sasang constitutional types (SCTs) are determined according to an individual's innate temperament and body shape, and they exert a profound effect on each person's risk for contracting disease and response to drugs. 5 This Korean-originated concept of SCT classification is now being interpreted with modern genetic science. For example, variants of fat mass and obesity-associated genes are assumed to influence constitutional discrepancy for body mass accumulation, resulting in different physiques among SCTs. 6
Since the introduction of SCM by Jema Lee (AD 1837–1900), a series of studies have investigated vulnerability to disorders according to SCT. In these studies, TE, SE, and SY showed significant differences in the prevalence rates of various chronic diseases (e.g., diabetes, hypertension, obesity). 7,8 Regarding incidence, SCT also displayed different patterns. For example, 24.3% of TE individuals were newly diagnosed with type 2 diabetes mellitus during a 10-year survey, followed by SY (14.3%) and SE (12.1%) individuals. 9
Taken together, these findings raise the possibility that SCT may be a potent factor in determining disease susceptibility in each person. One study showed the pattern of prevalence for 27 types of disorders according to SCTs using 1453 participants; 10 however, this study did not compare data between men and women. Therefore, there is a need to characterize the prevalence rates of diseases according to SCT and sex.
To investigate the contribution of SCT to susceptibility to disorders, the authors surveyed articles reporting the prevalence of disorders according to SCT, which is expected to be a foundation of further scientific investigation into SCM.
Materials and Methods
Data sources and keywords
A systematic literature survey was conducted using publicly available electronic databases. Searches were performed for all studies published before August 2015 in PubMed (
Eligibility criteria
Articles were screened by using the following inclusion criteria: (1) reported prevalence rates of disorders according to SCT in Korea, (2) included more than 400 participants from the general population, (3) showed information regarding prevalence rates for both male and female patients except for sex-dependent disorders (e.g., alopecia, irregular menstruation, ovarian neoplasm, and uterine fibroid), and (4) provided clear diagnostic criteria for disorders. Articles filtered by these criteria were read in full by the authors, who together then determined the suitability of each article. Articles that did not meet all of the necessary inclusion criteria were excluded from this study (Fig. 1).
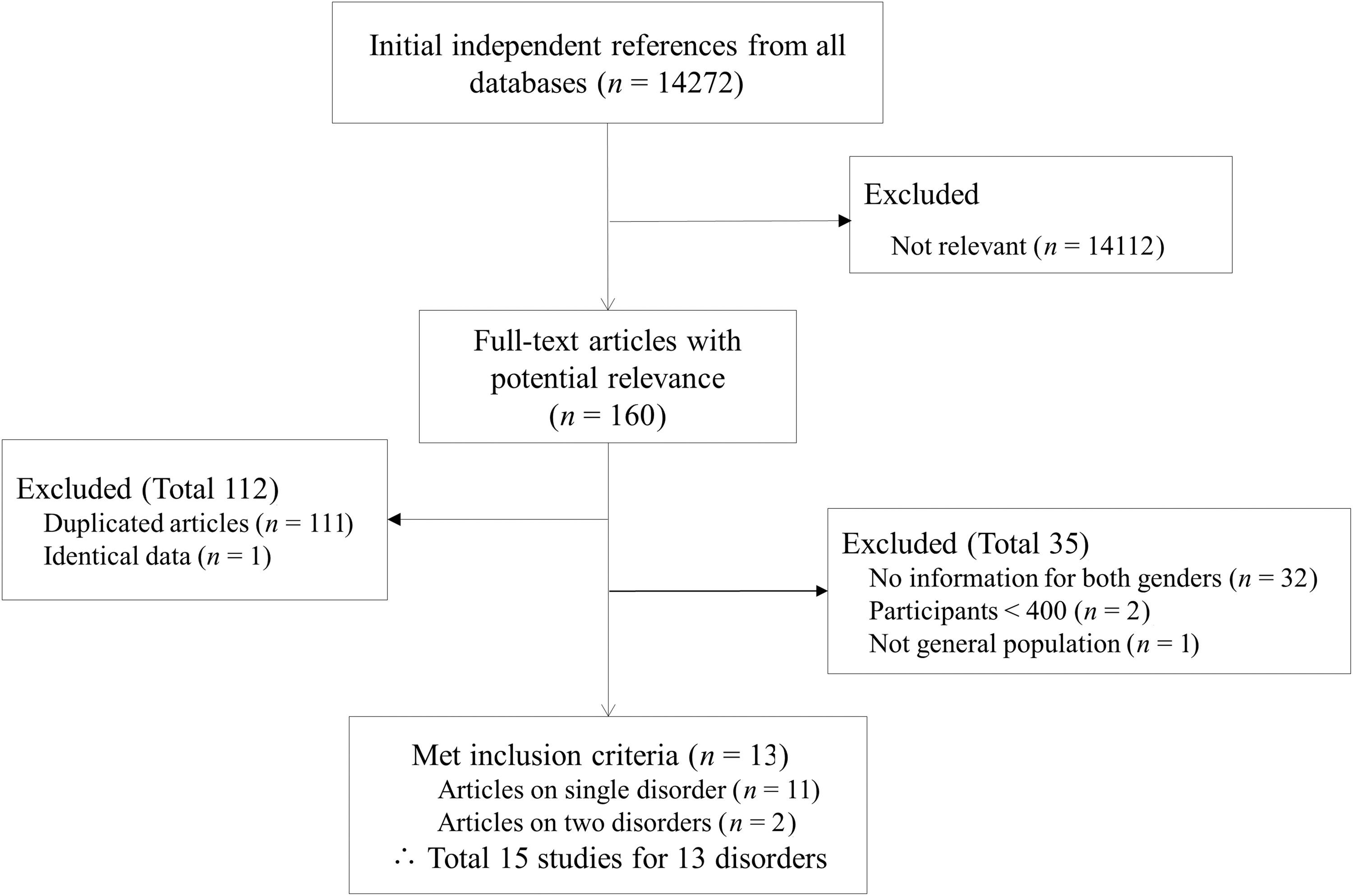
Flowchart of the studies included in this analysis.
Review process
The articles that passed the filtering criteria were collected, and data, including population, sex, age, disorder, and SCT (TE, SE, or SY type), were extracted. The TY type was excluded from this study because of the low frequency of TY-type individuals in the general Korean population (0.03%–0.1%). 5 If any article simultaneously concerned multiple diseases, then it was divided into separate studies of each disease.
Classification of Sasang constitution and diagnostic criteria of each disorder
The diagnostic tools for SCT classification in the collected studies are as follows: Sasang constitutional analytical tool (SCAT), Questionnaire for the Sasang Constitution Classification II (QSCC II), the revised QSCC II (QSCC II+), or SCM specialists. SCAT is a web-based SCT diagnostic tool developed by the Korea Institute of Oriental Medicine that combines four individual quantitative data: facial structure, body shape, voice analysis, and questionnaire responses. 11 QSCC II is a self-SCT diagnostic questionnaire consisting of 121 inquiries and QSCC II+ is simplified into 54 questions. 12 SCM specialists refer to traditional Korean medicine doctors specializing in SCM. The diagnostic criteria for each disorder are summarized in Table 1.
SBP, systolic blood pressure; DBP, diastolic blood pressure; WC, waist circumference; FBG, fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; IBS, irritable bowel syndrome; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory value in 1 second; FVC, forced vital capacity; BMD, bone mineral density.
Extraction of patient characteristic
The extracted information about population, sex, age, disorder, and the SCT of the patients from each study is shown in Tables 2 and 3 to characterize the pattern of disease susceptibility according to SCT and sex. The population is presented as the number of total participants and is broken down into male and female. The distribution of SCTs is given as a percentage. Age is provided as the mean (± standard deviation) or median.
Values expressed with a plus/minus sign are the mean ± standard deviation.
SCT, Sasang constitutional type; TE, Taeumin; SE, Soeumin; SY, Soyangin; SCM, Sasang constitutional medicine; SCAT, Sasang constitutional analytical tool; QSCCII, Questionnaire for the Sasang Constitution Classification II; QSCCII+, revised Questionnaire for the Sasang Constitution Classification II.
Values expressed with a plus/minus sign are the mean ± standard deviation.
p-Value obtained by chi-square test for each disease's prevalence rates among SCTs in male participants, female participants, and total.
p < 0.01; obtained by chi-square test for each disease's prevalence rates between male participants and female participants.
p < 0.05; obtained by chi-square test for each disease's prevalence rates between male participants and female participants.
T, total; M, male; F, female.
Statistical analysis
A chi-square test was applied to investigate the statistical significance of the differences in the prevalence rates of disorders according to SCT and sex. A p-value ≤0.05 was considered to indicate a statistically significant difference. All statistical analyses were performed by using SPSS software, version 18.0 KO for Windows (IBM Inc., Chicago, IL).
Results
Data characteristics
From 14,272 relevant articles, 160 articles were identified in the initial screening, and 13 articles were ultimately selected for this study (Table 2). Of the 13 articles, 11 articles surveyed a single disorder, whereas 2 articles investigated 2 disorders simultaneously, resulting in 15 studies of disorders. In addition to abdominal obesity and metabolic syndrome, 11 types of disorders had a single study (Table 3).
Among the 13 disorders, 4 were sex-dependent disorders (alopecia, irregular menstruation, ovarian neoplasm, and uterine fibroid); 9 were general disorders for both sexes, including 5 metabolic syndrome–related disorders (prehypertension, general obesity, abdominal obesity, metabolic syndrome, and diabetes mellitus); 2 were gastrointestinal disorders (functional dyspepsia and irritable bowel syndrome [IBS]); and 2 were other types of disorders (chronic obstructive pulmonary disease [COPD] and osteoporosis).
Participant characteristics and SCT diagnosis
Fifteen studies involved a total of 19,307 participants (6945 male and 12,362 female participants). The average number of participants was 1485 ± 938 (male, 631 ± 298; female, 1030 ± 594), ranging from 409 to 3348 participants across 15 studies. Participant ages were diverse depending on the study, ranging from 10 to 77 years. SCT diagnosis was obtained by SCM specialists for 5 studies, SCAT for 5 studies, and QSCC II or QSCC II+ for 5 studies. The proportions of the TE, SE, and SY types were 45%, 26%, and 29%, respectively, and no significant difference was observed in sex distribution (48%, 24%, and 28% in male participants and 42%, 28%, and 30% in female participants, respectively) (Table 2).
Prevalence of each disease by SCT
The average prevalence rate across 15 studies for the TE, SE, and SY types were 35.0 ± 25.2, 20.1 ± 15.2, and 22.6 ± 16.4, respectively. Of the 15 studies, 8 studies showed a significantly different prevalence pattern according to SCT for 6 disorders (prehypertension, general obesity, abdominal obesity, metabolic syndrome, diabetes mellitus, and IBS). Among these disorders, IBS was SE-type predominant whereas the others were TE-type predominant. Functional dyspepsia and osteoporosis showed partial significance, whereas 4 sex-dependent disorders and COPD did not show significant differences in SCT-related prevalence (Table 3).
Prevalence of each disease by sex and SCT
The average prevalence across 15 studies was 27.2 ± 18.3; by sex, it was 29.3 ± 18.5 for male participants and 26.1 ± 19.1 for female participants (except for 4 sex-dependent disorders). COPD was mostly male-predominant (5.6-fold; p < 0.01), along with several other disorders (1.5-fold for general obesity and diabetes mellitus, 1.4-fold for prehypertension; p < 0.05 or p < 0.001). Functional dyspepsia (1.9-fold), as well as abdominal obesity and metabolic syndrome (1.5- and 1.4-fold, in only one study), was significantly female-predominant (p < 0.001).
When the analyses were conducted for each sex, SCT-dependent differences in prevalence were observed repeatedly in both male and female participants. In addition, no disorder showed a significantly different pattern of SCT-related prevalence between male and female participants (Table 3).
Discussion
This review revealed that SCT has an effect on the prevalence rates of various disorders, especially disorders of the circulatory and metabolic systems. SCM is a Korean-originated medical theory that formulates a customized system of diagnosis, treatment, and prevention based on 4 SCTs (TE, SE, SY, and TY). The diagnosis of SCT depends on facial structure, body shape, voice, and personality originating from a functional imbalance among the visceral organs in an individual.
35,36
This functional imbalance includes hyperactive liver function and hypoactive lung function (TE, greater yin) and vice versa (TY, greater yang), as well as hyperactive kidney function and hypoactive spleen function (SE, lesser yin) and vice versa (SY, lesser yang). As such, each pair of the four visceral organs forms a “see-saw” relationship, affecting individuals’ digestive and metabolic performance.
37,38
The spleen–kidney pair regulates nutrient metabolism, in which the hot energy of the spleen draws in food and water whereas the cold energy of the kidney sends them out. On the other hand, the liver–lung pair controls energy metabolism, in which the cooled energy of the liver converts diet into qi ( ) and body fluid while the warmed energy of the lung expels them.
39
Several studies revealed a different aspect of susceptibility to disorders according to SCT, such as a more than 2-fold higher prevalence of fatty liver in TE-type individuals than in individuals of other SCTs.
40
) and body fluid while the warmed energy of the lung expels them.
39
Several studies revealed a different aspect of susceptibility to disorders according to SCT, such as a more than 2-fold higher prevalence of fatty liver in TE-type individuals than in individuals of other SCTs.
40
To evaluate and characterize the influence of SCTs on the development of disorders, the authors systematically reviewed articles about disorder prevalence by SCT. To minimize bias due to small sample sizes, only studies with greater than 400 participants were included. This review showed that SCT significantly affected the prevalence rates of 6 disorders: prehypertension, general obesity, abdominal obesity, metabolic syndrome, diabetes mellitus, and IBS. Except for IBS, the other 5 disorders (prehypertension, general obesity, abdominal obesity, metabolic syndrome, and diabetes mellitus) have a TE-predominant pattern, the average prevalence rates of which were 2.7-fold and 1.9-fold higher in TE than in SE and SY, respectively. Similar TE-predominant prevalence rates in these disorders were also observed in each sex group (Table 3). The etiology and pathologic features were also closely associated with each other, which were associated with the metabolic syndrome. 41,42 These results indicated that TE would be highly susceptible to metabolic disturbances and cardiovascular disorders, a finding supported by several recent studies.
During a 10-year follow-up study involving 2839 patients, 56.4% of TE-type individuals were newly diagnosed with metabolic syndrome, followed by SY (32.3%) and SE (14.5%) individuals, respectively. 43 In addition, one study showed that the TE type was predominant among 493 inpatients with cerebral infarction (56.4% for TE, 9.1% for SE, and 34.1% for SY). 44 Consistent with the current results, another study showed that both hypertension and dyslipidemia were more prevalent in TE-type individuals. 8
Recently, genome-wide association studies were performed to identify susceptible loci for common and complex diseases. 45 For example, individuals with genetic variants at the 12p13.33 locus had a greater risk for lung squamous cell carcinoma. 46 The classification of SCT is now in the process of interpretation with modern genome-wide association analysis for scientific evidence. 47,48 One group reported that the TE type is subject to higher levels of serum triglyceride but lower levels of high-density lipoprotein cholesterol, due to the 1131T>C polymorphism of APOA5, a genetic determinant of serum lipids. 49 Another study also observed that overweight TE-type women are often associated with the 889C/T polymorphism of interleukin-1α, affecting multiple neuroendocrine and metabolic functions. 50 For abdominal obesity 14,15 and metabolic syndrome, 16,17 two different groups have studied these disorders, and their findings were grossly similar.
According to SCM, SE-type individuals are prone to digestive problems because of deficient spleen function. 5 In the current data, the SE type showed a high prevalence of IBS 20 (1.8- and 1.4-fold for the TE and SY types) (Table 3). Several clinical studies have reported that SE-type individuals tend to report gastrointestinal symptoms (e.g., loss of appetite, discomfort in defecation). 51,52 However, the data revealed a TE-predominant pattern for functional dyspepsia. 19 Thus, further scientific evidence is needed to determine the relationship between the SE type and the digestive system. There was no significant difference in the SCT-related prevalence of 4 sex-dependent disorders: alopecia, 23 irregular menstruation, 24 ovarian neoplasm, 10 and uterine fibroid. 10 Several studies have reported a potentially sex-dependent difference in SCT-associated susceptibility in specific diseases, including cancer. 53 We therefore analyzed the sex difference in SCT-related prevalence, and no significant difference was observed (Table 3).
However, the current study has some limitations, including a relatively small number of participants for studying the susceptibility to disease, a lack of enrolled studies, and a wide variance in SCT distribution, which may be due to different types of SCT diagnostic criteria. Nevertheless, this review study strongly assumed the presence of SCT-associated susceptibility to specific diseases, especially metabolic syndrome–related disorders. To explain the underlying mechanisms of the different susceptibilities to specific disorders by the SCT trait, many previous studies have been performed. SCM classification is assumed to be connected to macro-level genomic differences. 54,55 In addition, there was a notably distinct profile of gut microbiota, indicating different behaviors of food intake and excretion and different biological and psychological characteristics according to SCT. 56 –58 Our study provides important insight into SCT-associated susceptibility to disorders, which is expected to be a foundation of further scientific investigation in SCM.
Conclusion
Taken together, the findings reported here suggest that SCT strongly affects the development of diseases, especially metabolic syndrome–related disorders. Further studies are needed to elucidate the concrete features of SCT-related susceptibility in the future, which may be valuable in preventive medicine using Sasang constitutional practice.
Footnotes
Acknowledgments
This research was supported by the Bio & Medical Technology Development Program of the NRF funded by the Ministry of Science, ICT & Future Planning (NRF-2014M3A9D7034335), the research program of the Korea Institute of Oriental Medicine (K16091), and the Oriental Medicine Research and Development Project, Ministry of Health and Welfare (HI15C-0112-000015), South Korea.
Author Disclosure Statement
No competing financial interests exist.