
Abstract
Background:
Burning mouth syndrome (BMS) is a chronic pain disorder that is difficult to diagnose and refractory to treatment; it is more prevalent in pre- and postmenopausal women. Acupuncture and auriculotherapy have been suggested as options for the treatment of pain because they promote analgesia and allow for the reduction of symptoms with lower doses of drugs; this leads to greater patient compliance with treatment and has a positive effect on quality of life. Clinical trials investigating the effectiveness of acupuncture in the treatment of BMS are scarce in the literature.
Objective:
To investigate the effect of combined acupuncture and auriculotherapy on pain management and quality of life in patients with BMS.
Methods:
Sixty patients with BMS were subjected to a thorough differential diagnosis. Of these, 12 met the inclusion criteria and agreed to participate. Eight patients completed treatment with acupuncture and auriculotherapy using a previously established protocol. The outcome variables were analyzed before and after treatment: pain/burning (visual analog scale; VAS), salivary flow (unstimulated sialometry), and quality of life (Short-Form Oral Health Impact Profile [OHIP-14]). Two-year follow-up was carried out by assessing VAS and OHIP-14.
Results:
The intensity of pain/burning decreased significantly after the first treatment sessions, as shown by low values on the VAS (0–2) and a subjective indicator of quality of life (mean = 5.37 ± 3.50). There was no relationship between salivary flow and the intensity of pain/burning. At 2-year follow-up, no statistically significant difference was observed for VAS, but improvement on OHIP-14 was seen.
Conclusions:
Combined acupuncture/auriculotherapy was effective in reducing the intensity of burning and improving quality of life. There was no relationship between salivary flow and the intensity of burning mouth. Patients' status improved after acupuncture and auriculotherapy at 2-year follow-up.
Introduction
B
The use of acupuncture for pain relief has been studied in many clinical trials and is commonly used as a supplement to conventional treatment. Its recognition has been enhanced by improved knowledge about the mechanism of pain relief involving endogenous opioids. 7 In addition, acupuncture leads to reduced pain and considerable improvement in quality of life. Among the main benefits of this treatment, increased salivary flow and a partial or total reduction in the burning mouth sensation have been noted. 8 A systematic review with a meta-analysis showed that acupuncture is effective for chronic pain beyond placebo. 9
Auriculotherapy is an alternative medicine modality based on the idea that the ear is a microsystem that reflects the whole body. 10 The evidence that it may decrease chronic pain intensity is still limited because of the significant clinical heterogeneity and methodologic flaws identified in the analyzed trials. 11,12
The World Health Organization (WHO) highlights the need for scientific studies that evaluate the effectiveness of acupuncture under controlled clinical conditions but, at the same time, recognizes the difficulties of establishing a well-designed and controlled study because of the difficulties with ruling out the placebo effect and performing retrospective surveys given the lack of well-designed studies. Thus, the WHO recommends that if rapid improvement can be achieved in the treatment of a long-standing, chronic disease or if there is definite improvement in a disease that is generally recognized as intractable to conventional treatment, the effect of acupuncture should be viewed in a more favorable light, even when a well-designed, controlled study has not been carried out. 13
The aim of this study was to investigate the association between the intensity of burning/pain, changes in salivary flow, and quality of life with the outcome of acupuncture treatment combined with auriculotherapy in a small group of patients with BMS. This preliminary single-arm study was performed to test the logistics and to gather information before a larger randomized controlled trial regarding sample size, inclusion/exclusion criteria, health records instruments, the treatment protocol, the acceptability of treatment, and training of staff in the administration and assessment of the intervention. 14 A literature review yielded only five publications exploring acupuncture for the treatment of BMS. These studies included the first systematic review on assessing the efficacy of acupuncture in BMS treatment, which reported a lack of evidence. None of these studies combined acupuncture with auriculotherapy.
Materials and Methods
This single-arm clinical trial with observation before and after the intervention was submitted to and approved by the Ethical Committee at the Federal University of Goiás, Brazil under protocol number 619111.
The eligible population for the study consisted of 60 patients with burning mouth symptoms, associated or not associated with other oral symptoms, who were referred to the Oral Medicine Center of Goiás State, School of Dentistry, Federal University of Goiás, Brazil, from 2009 to 2014. After a detailed diagnostic process by exclusion (Fig. 1), the BMS group consisted of 53 patients who fulfilled the inclusion criteria, presenting dysesthesia or burning mouth for at least 4 months, associated or not associated with dysgeusia and xerostomia, with a normal aspect of the oral mucosa, normal hematologic evaluation (complete blood count, fasting blood glucose, iron, ferritin, vitamin B12, folate, zinc, triiodothyronine, thyroxine, and thyroid-stimulating hormone), no uncontrolled diabetes, and no use of angiotensin-converting-enzyme inhibitors at the time of the study. The BMS group was part of another clinical study and was submitted to conventional pharmacotherapy.

Sampling. ACE, angiotensin converting enzyme; BMS, burning mouth syndrome; T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone.
One year later, the BMS group was recalled for clinical reevaluation. At this point the acupuncture and auriculotherapy research objectives, the benefits and risks of treatment, and the duration and number of sessions were explained.
Nineteen patients were without pain or burning symptoms at the time of recall, and 22 did not participate in the study for the following reasons: changing city (n = 1), limited mobility (n = 1), need for a caregiver (n = 2), no availability for two weekly therapy sessions during 6 consecutive weeks (n = 14), treatment dropout in the early stage of the research (n = 3), and skepticism regarding acupuncture treatment (n = 1). Those who agreed to participate in the study signed a consent form and were the final sample, composed of 12 patients. Of these, 4 dropped out in the early stages of data collection and 8 finished the treatment (Fig. 1). All patients included in this study underwent treatment with acupuncture and auriculotherapy by a single dentist with formal postgraduate training in Traditional Chinese Medicine and 17 years of experience in acupuncture.
Table 1 was based on the STRICTA guidelines (Standards for Reporting Interventions in Clinical Trials of Acupuncture) 5 and lists characteristics of the acupuncture and auriculotherapy treatment performed.
Acupuncture protocol
Needle insertion followed two protocols in all patients and all sessions: specific points for BMS and facial points. 16 Other points were chosen and used according to individual needs and on the basis of clinical reevaluation at the beginning of each therapy session.
The rationale for the acupuncture points used was established according to Traditional Chinese Medicine (TCM) principles. BMS points were chosen to tone the kidneys, eliminate heat from the blood and the liver fire, regulate qi and blood, eliminate fire, and regulate the spleen and stomach, thereby relieving pain. 16 All facial acupuncture points were those important for reducing pain and muscle tension caused by a burning sensation.
Points selected according to individual needs were based on the main individual general health problems reported by the patients, which were related to anxiety, sleep problems, headaches, throat discomfort, stomach problems, and rigidities in neck region. For very anxious patients and those with sleep problems, the following points were used: HT 3, HT 4, HT 7, and PC 6. For those with headaches, GB 1, GB 20, GB 34, GB 40, GB 43, and LV 2 were used. For patients who had throat discomfort, SJ 9 was used. Some of these patients had serious stomach problems, and in these cases the following points were selected: ST 41, ST 44, and ST 45. For significant rigidities in the neck region, LI 14 and LI 1 were used. 16
Auriculotherapy protocol
For auriculotherapy, crystal spheres were used to stimulate the elected auricular points by ear acupressure method. After proper cleaning of the entire auricle with alcohol 70%, these 1.5-mm-diameter spheres were placed unilaterally on the points by using delicate hemostatic forceps. These polished crystal spheres are considered neutral; they are trapped in adhesive plaster to be applied on the ear surface and to produce a mechanical action on the desired acupoint. They were changed once a week by alternating right and left ears, beginning in the right ear. 17
The auricular points were also chosen according to Traditional Chinese Medicine. The Shen Men and heart points have calming properties, the kidney point has an energy function, and the stomach and spleen points are crucial to maintaining the physiologic nutrition process, as well as emotional and intellectual equilibrium. The central nervous system point regulates the functions of sympathetic and the parasympathetic systems, providing general balance to the body. The mouth point is used for all symptoms related to the mouth. 18
Outcome variables: burning/pain intensity, salivary flow, and quality of life
Burning/pain intensity was subjectively assessed by using a visual analogue scale (VAS) before and after each acupuncture/auriculotherapy session. This is a numeric scale ranging from 0 to 10, which corresponds to the following scores: 6 0, no pain;1–3, moderate or mild pain; 4–6, regular or uncomfortable pain; 7–8, severe or distressful pain; 9–10, horrible or insupportable pain.
All selected patients underwent unstimulated salivary flow rate assessment; 18 –20 rates were analyzed according to the following references: normal, 0.25–0.35 mL/min; low, 0.1–0.25 mL/min; hypoflow, less than 0.1 mL/min; hyperflow, more than 0.35 mL/min. 16,21
The Short-Form Oral Health Impact Profile (OHIP-14) was used to assess quality of life. It consists of 14 questions about the dysfunction, discomfort, and inability related to oral health. 19,22 For its calculation, the following scores were attributed to each answer: 0, never; 1, rarely; 2, sometimes; 3, frequently; 4, always. These scores were multiplied by weights assigned to each question according to Allen and Locker. 23 The OHIP-14 was used at two distinct time points: at baseline and after the last (11th) acupuncture session. Patients were appropriately instructed about the questionnaire, which was administered as an interview.
Two-year follow-up was carried out by assessing the intensity of pain/burning and quality of life through the VAS and OHIP-14, respectively.
Data analysis
The statistical data were analyzed by using the Statistical Package for Social Sciences (SPSS for Windows, version 17.0, SPSS Inc., Chicago, IL). Analyses compared the variables before and after acupuncture/auriculotherapy treatment. For nonparametric data, the Wilcoxon test was used for comparison between the two groups. When the data were parametric, the paired-samples t-test was applied. The adopted significance level was 5% (p < 0.05).
Results
Sample features
All eight patients who completed the treatment were women. Their ages ranged from 45 to 74 years (μ = 65 ± 9.12 years).
Effect of acupuncture and auriculotherapy on burning/pain intensity, salivary flow, and quality of life
Acupuncture treatment and auriculotherapy led to significant improvement in the intensity of burning/pain, as measured by VAS, starting with the first session (p = 0.005), with a gradual reduction. Seven of the 11 sessions showed a difference in the averages before and after treatment very close to 0, generating no statistical significance (Table 2). At the end of the fifth session, seven patients reached a VAS score of 0 or very close to it, remaining without symptoms until the end of treatment (11th session). In the last session, only two patients had a VAS score of 2, but they reached a score of 0 at the end of the session.
Paired t-test.
p < 0.05.
VAS, visual analog scale; SD, standard deviation.
The average salivary flow did not significantly change after acupuncture and auriculotherapy (p < 0.623), and considerable heterogeneity in sialometric values was observed before and after treatment (Table 3, Fig. 2).
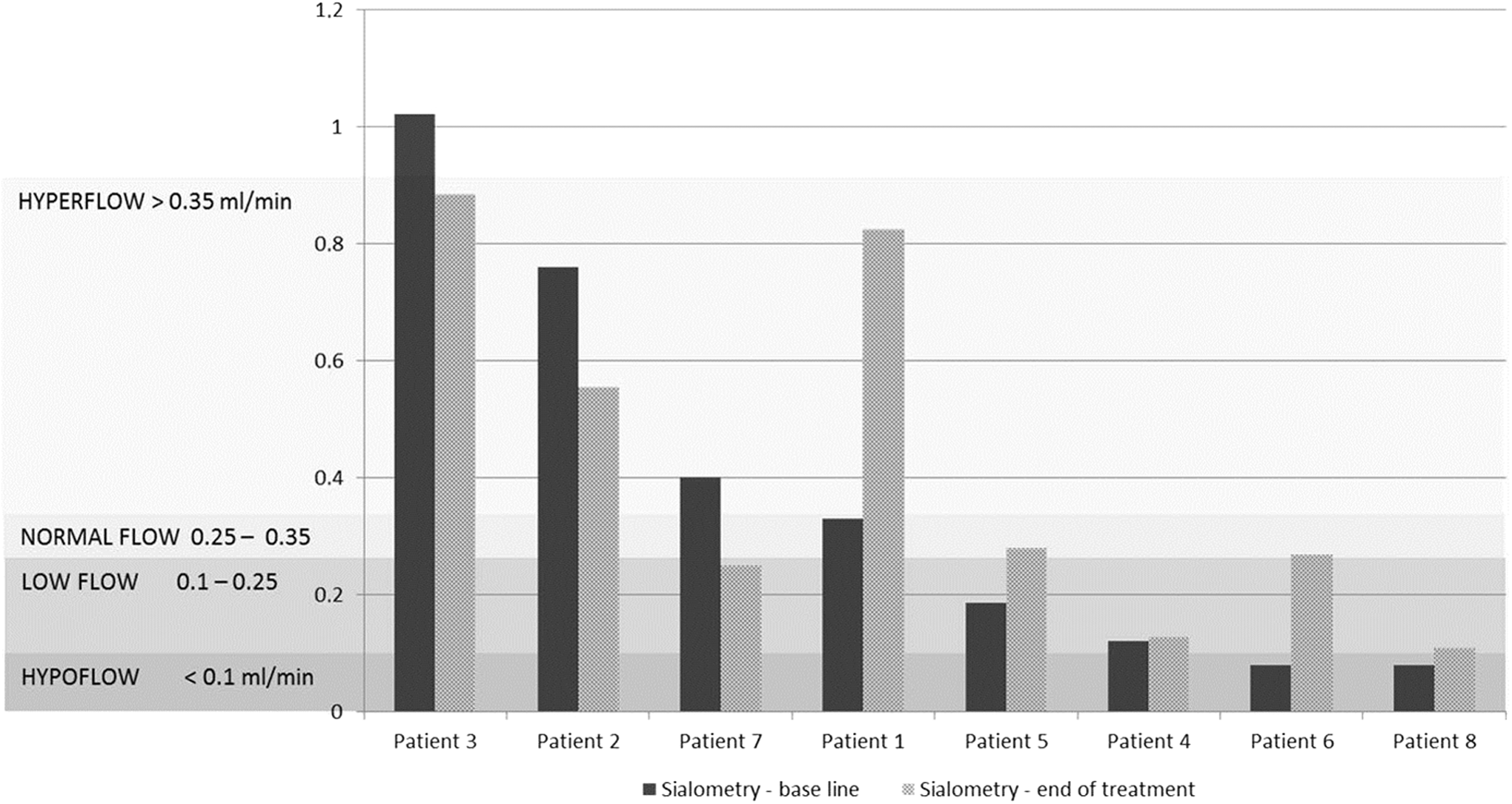
Sialometric values of each patient's salivary flow at baseline and after acupuncture and auriculotherapy.
Paired t-test.
Most patients (n = 6) reported dry mouth before treatment, independently of having normal or altered salivary flow or low or high VAS values (scores of 2 or 8, respectively). After treatment, dry mouth symptoms remained sporadic in only one patient, who sought treatment for low salivary flow and a VAS score of 8 (patient 5); this patient had improvement in symptoms to a normal flow and a VAS score of 0 (Table 3, Fig. 2).
Four patients still had low salivary flow after treatment (patients 4, 6, 7, and 8), but this did not interfere with the total remission of burning (VAS score, 0) that occurred at the fourth acupuncture and auriculotherapy session for three of them (Table 3).
Of the two patients with hypoflow before acupuncture and auriculotherapy, one (patient 6) improved to normal flow, with total remission of burning, after the fifth session to the end of treatment and with no dry mouth symptoms. The other, patient 8, finished treatment with low flow (VAS score, 2), but without the dry mouth symptoms she had before treatment (Table 3, Fig. 2).
Of the three patients with hyperflow before treatment, only one (patient 7) did not report dry mouth (Table 3).
All patients answered the OHIP-14 questions at baseline and after treatment. Scores significantly decreased after acupuncture and auriculotherapy (p = 0.005), suggesting an improvement in quality of life (Table 4).
Paired t-test.
OHIP, Short-Form Oral Health Impact Profile.
At 2-year follow-up, there was no statistically significant difference when average VAS score was compared to scores after treatment and baseline (Table 5), even most patients have had a return of pain/burning. A significant difference was observed (p = 0.005) when average OHIP-14 at 2-year follow-up was compared to that at baseline (Table 5).
Paired t-test.
Discussion
The main finding of this study was the significant reduction in burning/pain intensity after acupuncture and auriculotherapy treatment in patients with BMS, which was clearly evidenced by the VAS scores in the first few sessions.
Many studies have investigated acupuncture and auriculotherapy in pain treatment, but not many have combined therapies. 21,22,24,25 Auriculotherapy is usually combined with somatic acupuncture, and it is believed that there is a synergy between them, with a positive effect in terms of reducing pain. 21,22,24,25
Few clinical trials have evaluated the effectiveness of acupuncture in the treatment of BMS. The first systematic review performed to search for evidence on the efficacy of acupuncture and acupoint injection treatment in the management of BMS reported a lack of evidence. However, considering the positive outcomes/analgesia reported in some publications, further studies are recommended. 8
The analgesia produced by acupuncture has been explained by a neurophysiologic process that occurs when acupuncture needles are inserted. Neuroimaging studies have indicated that acupuncture modulates activity in multiple cortical and subcortical brain areas, which includes endogenous antinociceptive limbic networks. This modulation of subcortical structures may be an important mechanism through which acupuncture exerts its complex multisystem effects. The cerebral responses elicited by acupuncture stimulation are extensive and are still not fully understood. 23,24,26,27 Previous studies have reported an association with changes in blood flow and increasing microcirculation in the oral cavity with significant improvement of BMS after acupuncture. 25,26,28,29
Some studies have suggested that the mechanism of action of auriculotherapy modulates the reticular formation and the autonomic nervous system. 27,30 The auricle has innervations that, upon receiving a stimulus, sensitize brain regions such as the brainstem, cortex, and cerebellum. Each point on the auricle is directly connected to one part of the brain and so to the central nervous system. 10
Seeds, needles, semi-permanent needles, and laser are well known options with which to stimulate the ear points. The frequent exchange of stimulators trapped in tapes and moisture accumulation in the pinna can promote inflammation and injury during auriculotherapy, especially in a tropical country such as Brazil. The crystal spheres are safe because quartz crystal is not organic matter and is less likely to stick to the skin. These crystals are well tolerated by people with sensitive skin, such as the elderly and children. 17
Evidence for efficacy of auriculotherapy in the treatment of pain is similar to what has been found for acupuncture; this therapy has shown positive results in terms of pain management. 11,12,28,11,12,31 Auriculotherapy has been recommended as an adjunctive therapy in the treatment of pain and helps minimize the use, adverse effects, and tolerance of analgesics. 11,12,28,31
The decision to perform this single-arm trial was mainly due to the quality of the sample selected, although it was small. The rigor established in the BMS differential diagnosis process ensured a sample with truly essential BMS. All possible local and/or systemic causes of burning mouth symptoms were excluded. This made the trial worthwhile and justified the relevance of this preliminary study. The lack of well-established clinical criteria in sample selection and even the absence of their description in publications are some of the limitations of the already scarce clinical trials investigating the management of BMS in general. 29,30,32,33 A rigorous sample selection process associated with the age range of these patients, who had various limitations regarding study participation (mobility impairment, lack of availability for a weekly treatment without interruption for 6 weeks, caregiver needs) contributed to the small sample size, making the segmentation of a control group impossible. Various efforts were made to increase the study sample size. A larger sample and the presence of a control group, matched by age and sex, would provide more consistent scientific evidence.
Xerostomia is often associated with a burning mouth sensation, 31,32,34,35 which was not found in this study. Other authors have also reported no association between nonstimulated salivary flow rate and BMS. 33 –38 The unchanging status of salivary flow rate after acupuncture/auriculotherapy and no association with a reduction or remission of burning mouth and even dry mouth symptoms, which improved in almost all patients, reinforce the hypothesis of a neuropathic origin of BMS. Neurophysiologic, psychophysiologic, neuropathologic, and functional magnetic resonance imaging studies have shown that the essential mechanism of BMS is associated with sensory changes in the central, peripheral, or mixed level nervous systems. 36 –41 In other words, the neurochemical mechanism induced by acupuncture/auriculotherapy might act at the level of the supposed neuropathic disorder, improving burning/pain, without stimulating saliva production.
Changes in salivary composition and flow have been associated with mucosal atrophy and/or subclinical inflammation, 35,38 which may be accompanied by oral neuropathy, dry mouth, and taste alterations in patients with BMS. 34,35,37 –39,42 Other studies have shown no difference in salivary flow in patients with BMS and healthy patients. 34,37,40,43 Despite no significant changes in salivary flow, mechanical salivary stimulation in patients with BMS results in a significant decrease in total protein levels in saliva and an increase in tumor necrosis factor-α, 41,44 which may account for the clinical effectiveness of therapy. This effectiveness included a significant reduction in the burning sensation and number of burning sites, as well as an improvement in taste disturbances and xerostomia.
The results of this study revealed significant improvement in the perception of quality of life after acupuncture/auriculotherapy in patients with BMS, as measured by OHIP-14. The OHIP-14 instrument is considered a good tool to capture the perceptions and feelings of individuals regarding their own oral health and their expectations regarding treatment and dental services. 42,45 A previous study investigated the effect of BMS on quality of life by using the abbreviated instrument of the World Health Organization Quality of Life among 116 patients (58 with BMS and 58 controls). The results showed interference in the physical and psychological domains. The syndrome is closely related to emotional changes, such as anxiety, depression, and stress, which interfere with the psychological domain. The pain or persistent discomfort affects well-being and the physical domain. All these factors negatively influence patients' quality of life. 43,46
Lower quality-of-life scores in patients with BMS have also been demonstrated by cross-sectional studies 44,45,47,48 across all domains of the Medical Outcomes Short-Form health survey (SF-36). 44,47 On the other hand, a pilot study investigated the use of acupuncture in 10 patients diagnosed with BMS using the same questionnaire (SF36) and did not identify significant improvement in quality of life, even with a statistically significant reduction in the VAS, although with an average of only 0.99 points of pain scale. 49
The sample size and the large standard deviation of the average VAS score at 2-year follow-up (standard deviation, 2.34) could be responsible for the lack of statistically significant difference when averages VAS were compared. However, when the average quality-of-life measure (OHIP-14) at baseline and 2-year follow-up were compared, the post-treatment improvement remained.
The 2-year follow-up results showed improvement in the status of patients after acupuncture and auriculotherapy. They strengthen the importance of the association of subjective self-perception instruments to VAS for evaluating the effectiveness of pain treatment methods, as well as the need for larger samples and longer longitudinal follow-up to confirm the results obtained in this study.
Despite the limited design, these results should encourage further studies on acupuncture in the treatment of BMS, especially because it is an inexpensive therapeutic option that promotes the humanization of the professional–patient relationship and a more holistic view of health.
Conclusions
These results allow us to make the following inferences: (1) Acupuncture reduces the intensity of burning and improves quality of life, but sham-controlled studies with a larger sample and possibly blinding are needed; (2) there was no relationship between salivary flow, dry mouth, and the intensity of burning mouth, which may strengthen the theory of the neuropathic origin of BMS; (3) patients had improved quality of life (OHIP-14) after acupuncture and auriculotherapy at 2-year follow-up; (4) longer longitudinal follow-up of patients is necessary to evaluate the stability of the results and differences among patients.
Footnotes
Acknowledgments
The authors thank Professor Carolina Rodrigues Costa and undergraduate student Isabella Munich Corrêa Caputto from the Institute of Tropical Pathology and Public Health, Federal University of Goias, for contributing to the microbiological tests for the differential diagnosis of patients with BMS. This study was supported by a scholarship from CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).
Author Disclosure Statement
No competing financial interests exist.