
Abstract
Background and Objective:
Spastic hypertonia usually occurs in patients with chronic disorders of consciousness (DOC) following severe traumatic brain injury (TBI). Spinal motor neuron excitability has been reported to increase in patients with brain damage. The aim of this study was to evaluate the immediate effects of acupuncture on spinal motor neuron excitability in patients with DOC following TBI by using evoked electromyography.
Setting and Participants:
Eleven male patients (mean age, 33 ± 14 years) with refractory muscle spasticity of the upper extremity accompanying chronic DOC following TBI and admitted to Chubu Medical Center for Prolonged Traumatic Brain Dysfunction were included.
Design:
A crossover study design was used. Changes in variables in the acupuncture session were compared with those in the control session in the same patients.
Intervention:
Acupuncture treatment was performed at GV 26, Ex-HN 3, bilateral LI 4, and ST 36 for 10 minutes.
Outcome measures:
F-wave was recorded from the abductor pollicis brevis muscle. The main outcome measure was F/M amplitude ratio (F-wave amplitude/M-wave amplitude), calculated as an index for spinal motor neuron excitability. F-waves were recorded before treatment (baseline), 10 minutes after needle insertion (phase 1), and 10 minutes after needle removal (phase 2). The same procedure was followed in the control session without acupuncture on a separate day.
Results:
F/M ratio was significantly reduced from baseline to phase 1 (p < 0.001) and phase 2 (p < 0.001) in the acupuncture session, whereas no significant changes were observed in the control session. Changes in F/M ratio from baseline to phase 1 and phase 2 were greater in the acupuncture session than the control session (p = 0.001 and <0.001, respectively).
Conclusion:
The excitability of the spinal motor neurons in patients with DOC following TBI was reduced after acupuncture treatment, suggesting that it is beneficial for reducing spastic muscle hypertonia in these patients.
Introduction
S
Motor deficits caused by severe spasticity in patients with severe brain injury increase the possibility of misdiagnosing the degree of DOC because the clinical signs of consciousness, such as voluntary movements, are no longer visually detectable at the bedside. 14 Therefore, preventing and reducing spastic muscle hypertonia is one of the most important strategies for the treatment of DOC.
F-wave measurement, a useful noninvasive index representing the excitability of spinal motor neurons, has been used to evaluate the effects of various treatments for spasticity. 15 –19 The measurement is obtained by using evoked electromyography, and F-wave is induced by the antidromic activation of the motor neurons. 20 In the chronic stage of upper motor neuron lesions, the spinal cord excitability increases, and F-wave parameters such as F/M amplitude ratio and F-wave persistence in patients at this stage have been reported to be higher than those in healthy persons. 15,18,21 –23 F-wave also changes with muscle tone after cerebral insult 19 and has been reported to be a more sensitive method than H-reflex and T-reflex. 15
Acupuncture is a part of traditional medicine originating in ancient China; it was further developed in East Asian countries, including Japan. Some studies have reported that acupuncture and electrostimulation of acupuncture points are effective in reducing muscle spasticity following cerebral stroke and TBI. 24 –29 Using neurophysiologic measurements, the technique has also reduced spinal motor neuron excitability in stroke patients. 25,27 However, there appear to be no studies that have used F-wave measurements to investigate the effects of acupuncture on spasticity in patients with DOC following severe TBI. The study hypothesis was that acupuncture treatment will reduce the excitability of spinal motor neurons in these patients, leading to a reduction in muscle hypertonia.
The aim of this study was to use F-wave measurements to evaluate the immediate effects of acupuncture on the excitability of spinal motor neurons in patients with chronic DOC accompanied by spastic muscle overactivity following severe TBI.
Materials and Methods
Design and ethical approval
A crossover study design was used. The changes in variables during the acupuncture session were compared with those during the control session (resting state without acupuncture) conducted on another day. The sessions were performed in a computer-generated random order, and each session was separated by an interval of at least 1 week.
This study was approved by the ethics committee of Kizawa Memorial Hospital and was conducted in accordance with the Helsinki declaration. Written informed consent was obtained from the legal guardians of the participants because the participants could not give consent because of DOC; they were free to withdraw from the study at any point.
Setting and participants
The study was carried out in the examination room of the Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, Gifu, Japan. The inclusion criteria were as follows: (1) muscle spasticity score of greater than 2 on the modified Ashworth scale (MAS) in the upper limbs (MAS score of 2 indicates marked increase in muscle tone through most of the ranges of motion [ROM]), 30 (2) flexional abnormal posture in the elbow joint due to spastic muscle overactivity, (3) DOC following traffic TBI, (4) at least 3 months since injury, (5) at least 3 months since admission to the study hospital and start of standard pharmacologic treatment and rehabilitation, including stretching therapy and ROM exercise of limbs for spastic muscle overactivity, and (6) at least 1 month since last change of medication.
Eleven male patients (mean age ± standard deviation [SD], 33 ± 14 years) with tetraplegia and muscle spasticity of the upper extremity accompanying DOC following severe TBI were included in the study. The participants' characteristics and TBI diagnosis are shown in Table 1. TBI diagnosis was based on computed tomography and magnetic resonance imaging. The mean time ± SD from injury to inclusion in this study was 19 ± 8 months, and the mean ± SD time from admission to the study hospital to inclusion was 10 ± 6 months. This study included four patients in a vegetative state (more recently referred to as unresponsive wakefulness syndrome) 1,31,32 and seven patients in a minimally conscious state. 33 All patients had tetra-paresis and exhibited flexional abnormal posturing and a reduction of passive ROM in the upper limbs due to muscle overactivity and contracture. They were incapable of movement on their own and received central and/or peripheral muscle relaxants, including oral baclofen and/or dantrolene sodium hydrate.
DOC, disorders of consciousness; EMG, electromyography; M, male; DAI, diffused axon injury; VS, vegetative stage; UWS, unresponsive wakefulness syndrome; R, right; SAH, subarachnoid hemorrhage; L, left; ICH, intracerebral hemorrhage; MCS, minimally conscious state.
Intervention
The time course of this study is shown in Figure 1. Patients first maintained rest in the supine position for 10 minutes and then received acupuncture treatment at GV 26, Ex-HN 3, bilateral LI 4, and ST 36. GV 26 is located on the face at the midpoint of the philtrum midline, Ex-HN 3 is located in the middle of the forehead at the midpoint of the line midway between the medial ends of the eyebrows, LI 4 is located on the dorsum of the hand radial to the midpoint of the second metacarpal bone, and ST 36 is located on the anterior aspect of the leg and the tibialis anterior muscle under the knee (Fig. 2). Details of the locations of these points are given in the World Health Organization guideline on standard acupuncture points. 34 On the basis of Traditional Chinese Medicine, previous reports, and the authors' clinical experiences, these points were chosen to achieve antispastic, relaxation, and brain activation effects in patients with DOC. 26,35,36 Previous studies have reported that GV 26 can be used for treatment of patients with DOC following brain injury, 26,37 LI 4 and LI 36 can be used for treatment of spasticity after stroke and brain injury, 28,38 and Ex-HN3 can be used for relaxation and sedation. 39,40

Schedule of F-wave measurement. Rest refers to resting state with supine position.
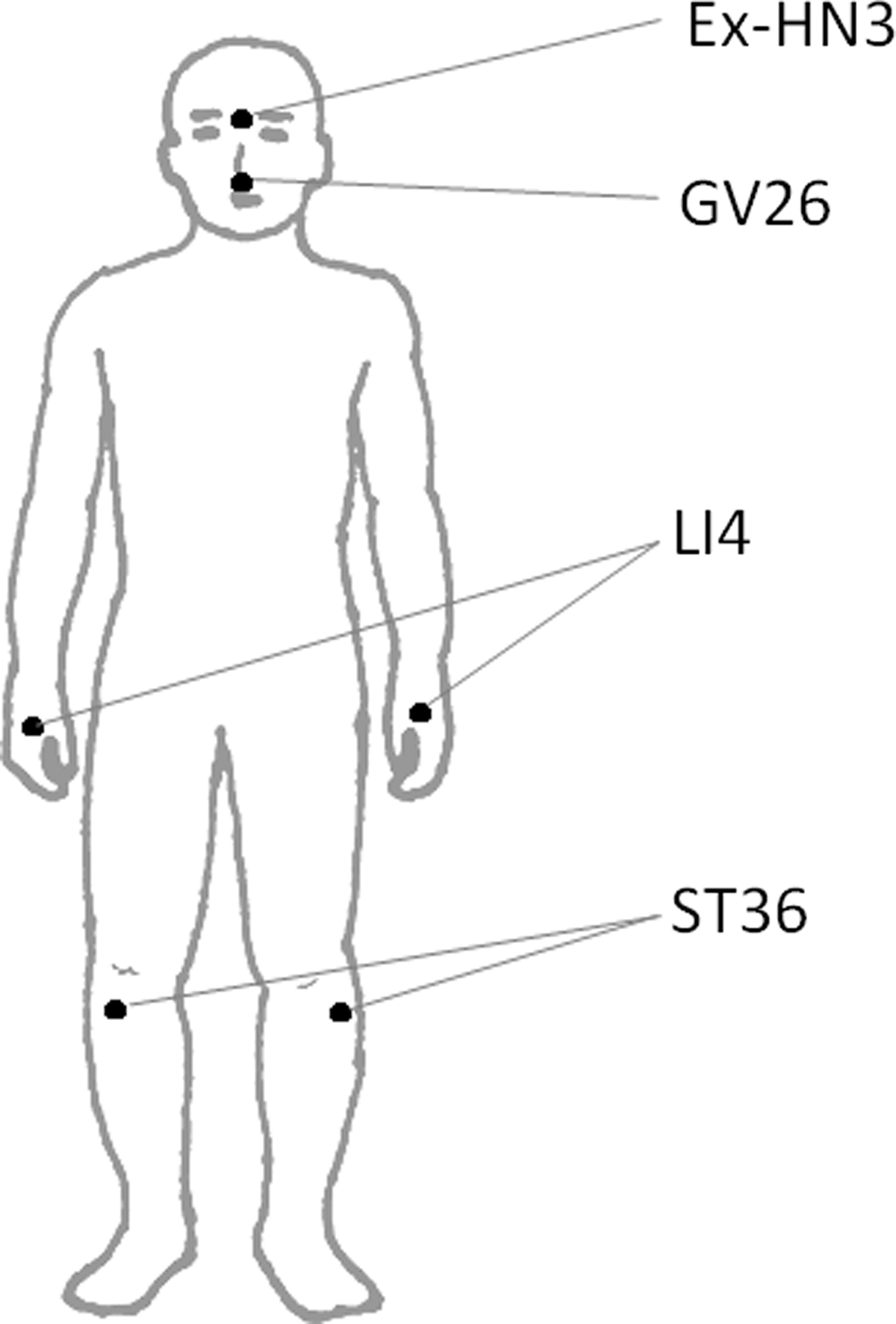
Acupuncture points used.
The Japanese style of acupuncture was used in this study, wherein stainless steel, disposable acupuncture needles (0.16 mm in diameter and 40 mm in length) (Seirin, Shizuoka, Japan) were inserted gently into the acupuncture points up to a depth of 3–15 mm. The needles were left in the points without manipulation for 10 minutes and then removed. All procedures were carried out by an acupuncturist with a national license, a Master's degree in acupuncture, and 9 years of practical experience.
In the control session conducted on a separate day, the patients maintained a resting supine position and did not receive any acupuncture treatment.
Outcome measures
F-waves were recorded and analyzed by using a Neuropack MEB 2200 recorder (Nihon Koden, Tokyo, Japan) with a band-pass filter of 50 Hz to 3 kHz, and the sensitivity was set at 2 mV and 200 μV per division to record the direct M-wave and F-wave. Sixteen F-waves, elicited by electric stimulation of the median nerve, were recorded from the abductor pollicis brevis muscle (Fig. 3) on the more affected side (right side, n = 9; left side, n = 2) of each patient in resting supine position. At the beginning of the session, the maximal amplitude of the M-wave was recorded. The stimulus intensity used to elicit F-wave was more than the 120% that is required to elicit a maximal M-wave response. Sample images of the F-wave and M-wave are shown in Figure 4. The electrical stimulus rate and duration were 1 Hz and 0.2 milliseconds, respectively. Electromyographic electrodes were attached firmly over the abductor pollicis brevis muscle, and the median nerve was stimulated with a rigid bar electrode strapped securely to the wrist, with the cathode positioned proximally (Fig. 3). The ground electrode was placed between the stimulating and recording electrodes.

Measurement of F-wave. G, ground electrode; R, recording F-wave from abductor pollicis brevis muscle; S, electrical stimulation of the median nerve.
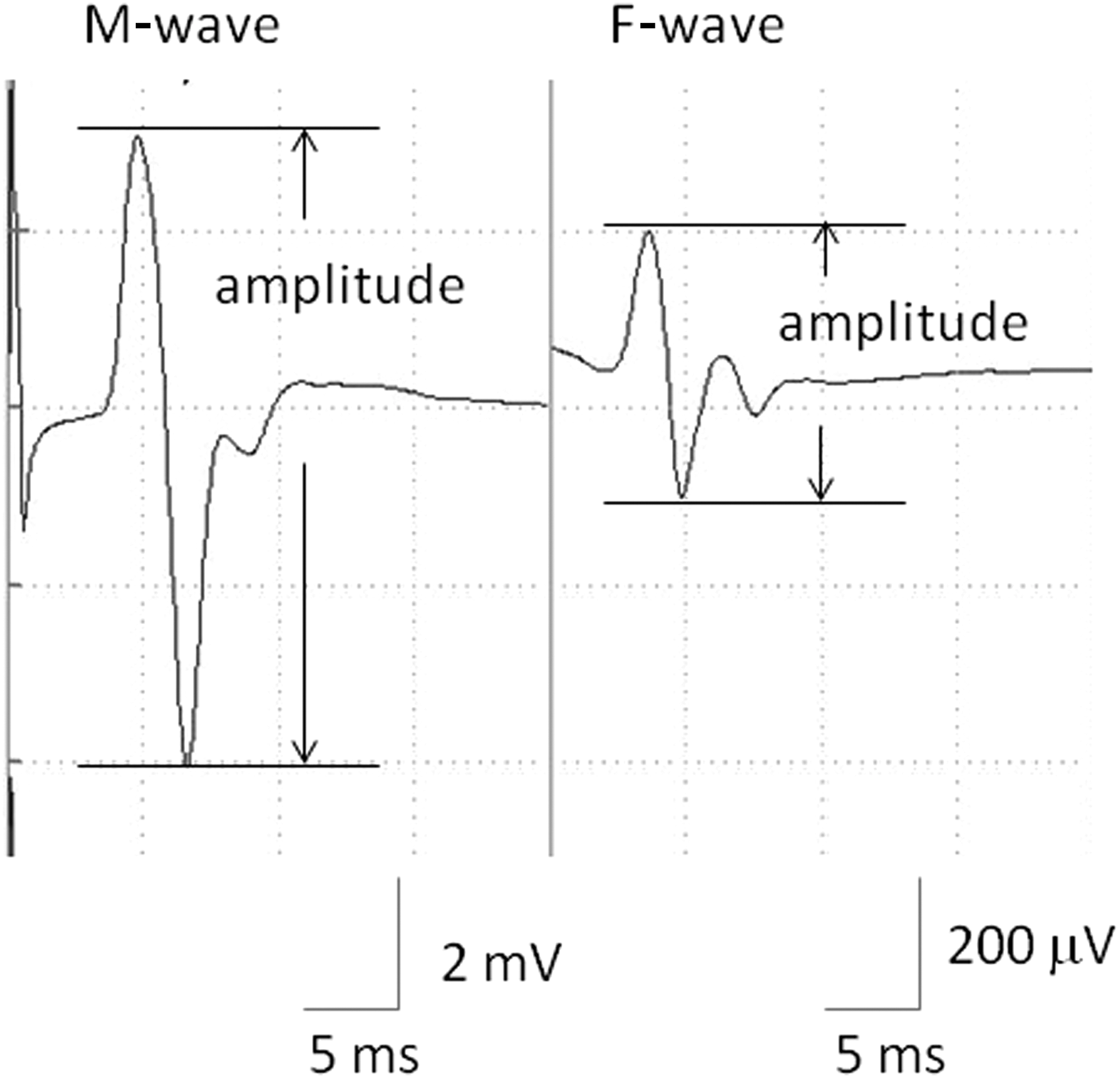
Sample of F-wave image.
F-wave is defined as a response with peak-to-peak amplitude greater than 50 μV. The mean F/M ratio (mean F-wave amplitude/M-wave amplitude) was calculated to evaluate spinal motor neuron excitability. F-wave occurrence (persistence) and mean F-wave amplitude were also calculated.
F-wave recordings were performed in three phases: baseline, 10 minutes after insertion of acupuncture needle (phase 1), and 10 minutes after removal of acupuncture needle (phase 2). The stimulus intensity in phases 1 and 2 was the same as that at baseline. In the control session, the F-wave was recorded three times with 10-minute intervals, similar to the acupuncture session.
The changes in F/M amplitude ratio from baseline to phases 1 and 2 were compared between the acupuncture and control session. The secondary outcome measures were other parameters of F-wave, including mean F-wave amplitude and F-wave occurrence.
Statistical analysis
The Shapiro-Wilk test was used to assess distribution. Normally distributed variables were expressed as the mean ± SD, while those without normal distribution were expressed as median and quartiles (first and third). When the values at each phase (baseline, phase 1, and phase 2) were normally distributed in the two groups (acupuncture and control sessions), a two-way repeated-measures analysis of variance with post hoc Bonferroni test was used for statistical comparison between the session and phase and between each phase (baseline and phase 1, baseline and phase 2, and phases 1 and 2). When the data were not normally distributed, a Bonferroni collected Wilcoxon singed-rank test with a Friedman test was used for comparison of each phase (baseline versus phase 1, baseline versus phase 2, and phase 1 versus phase 2). The changes from baseline to phase 1 and phase 2 were compared between acupuncture and control sessions by using paired t-tests for parametric variables or Wilcoxon singed-rank tests for nonparametric variables. To test for period and carryover effects, an independent sample t-test was used on the difference and the sums of the summary scores of the changes from baseline to phase 2 in F/M ratio for the first and second sessions.
p-Values less than 0.05 were considered to indicate statistically significant differences, except for the Bonferroni correction (number of comparisons = 3), for which a p-value less than 0.05/3 was considered to indicate a significant difference.
All statistical analyses were performed with SPSS software, version 22 (IBM, Armonk, NY) for Windows.
Results
F/M ratio
The changes in F-wave parameters are shown in Figure 5 and Table 2. No significant differences in the baseline value of the F/M ratio (p = 0.934), mean F-wave amplitude (p = 0.193), F-wave occurrence (p = 0.719), and M-wave amplitude (p = 0.173) were observed between the control and acupuncture sessions.
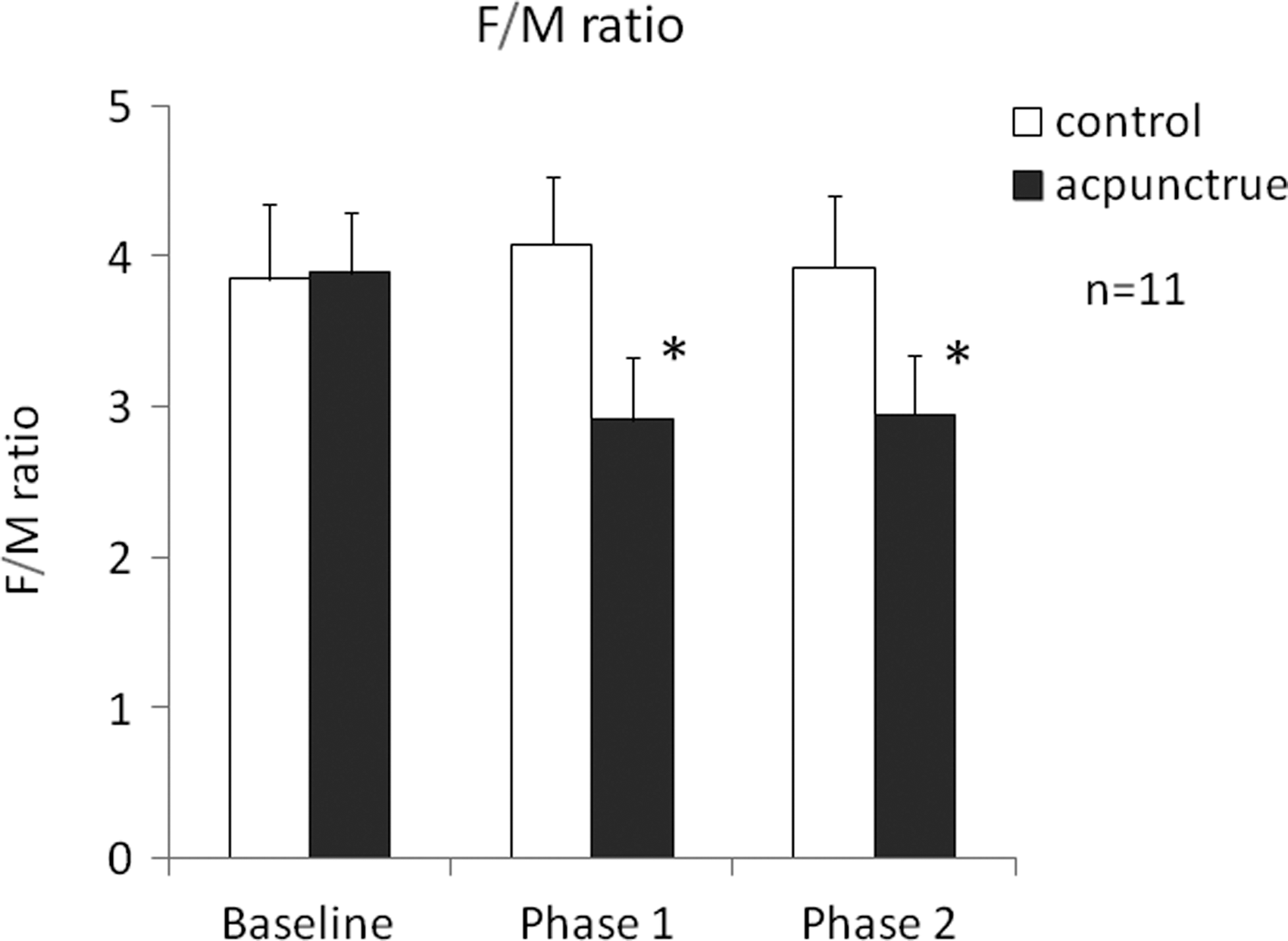
Changes of F-wave amplitude/M-wave amplitude (F/M ratio) in both sessions. Error bars indicate standard error. *p < 0.001 versus baseline.
Data are shown as median (25th percentile, 75th percentile) or mean ± standard deviation.
p = 0.004 vs. baseline.
p = 0.003 vs. baseline.
p = 0.003 vs. control.
p = 0.002 vs. control.
ΔPhase 1, change from baseline to phase 1; ΔPhase 2: change from baseline to phase 2.
The mean F/M ratios were 3.89 ± 1.34, 2.91 ± 1.29, and 2.95 ± 1.30 at baseline, phase 1, and phase 2, respectively, in the acupuncture session. The corresponding values in the control session were 3.85 ± 1.66, 4.08 ± 1.44, and 3.92 ± 1.58 (Fig. 5). There was significant interaction in F/M ratio (p < 0.001) between the sessions and phases. Significant reductions were observed from baseline to phase 1 (mean difference [95% confidence interval (CI)], 0.98 [0.54–1.43]; p < 0.001) and from baseline to phase 2 (0.95 [95% CI, 0.49–1.40]; p < 0.001) in the acupuncture session. Changes in F/M ratio from baseline to phase 1 (1.20 [95% CI, 0.63–1.79]; p = 0.001) and phase 2 (0.91 [95% CI, 0.47–1.35]; p < 0.001) were larger in the acupuncture session than the control session (Fig. 6). Six patients attended the control session and then the acupuncture session, and five patients attended the acupuncture session and then the control session. The changes in F/M ratio from baseline to phase 2 in the control-first group and treatment-first group are shown in Table 3. There were no significant period effects (p = 0.824) or carryover effects (p = 0.543).
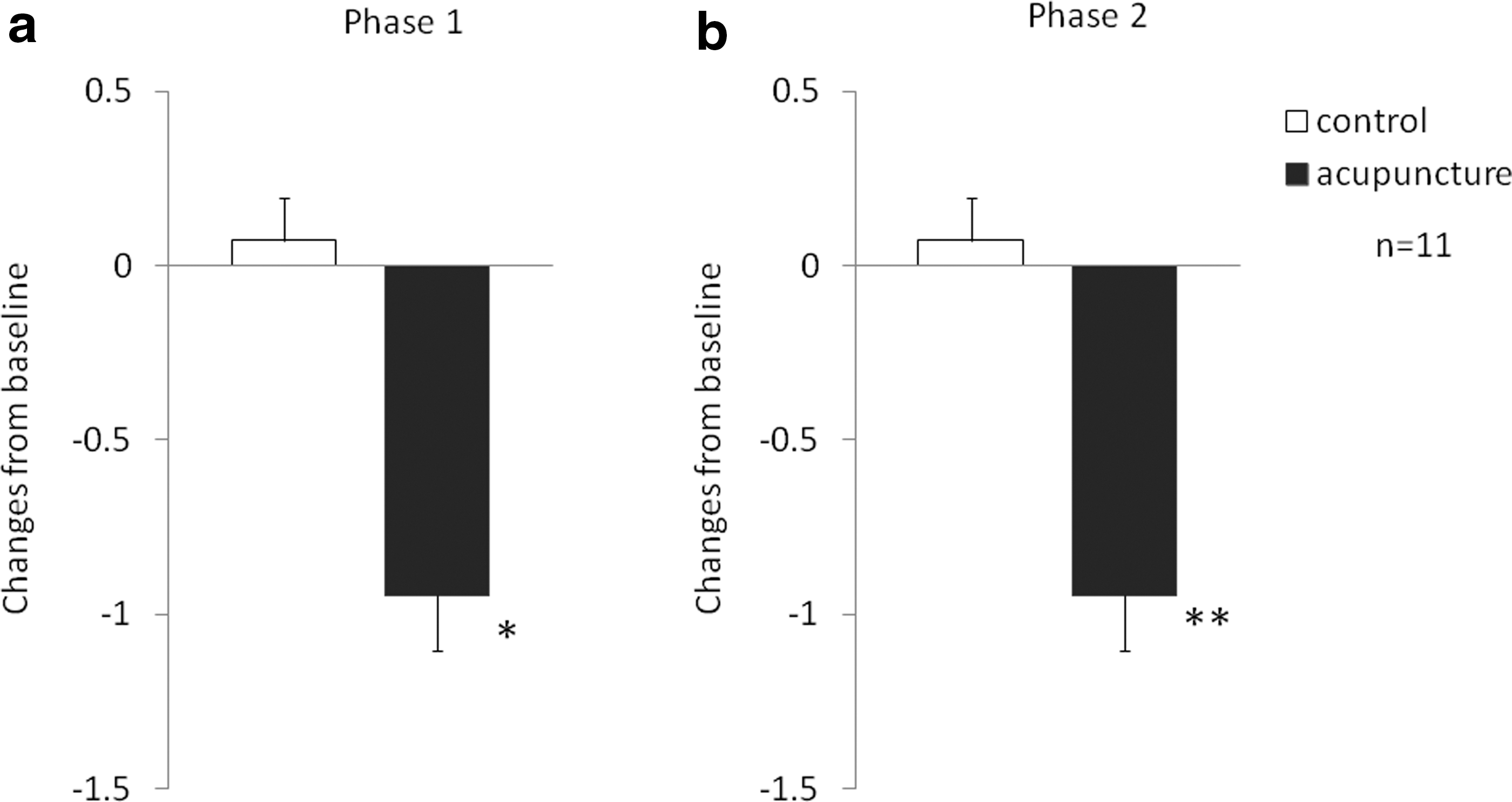
Changes in F/M ratio from baseline at phase 1
Data are shown as mean ± standard deviation.
Mean F-wave amplitude
The mean F-wave amplitude was reduced significantly at phase 1 (p = 0.004) and phase 2 (p = 0.003) in the acupuncture session, while no significant changes (p = 0.100) were observed in the control session (Table 2). The mean value of changes in F mean amplitude from baseline to phase 1 and phase 2 were larger in the acupuncture session than the control session (mean difference,115.8 [95% CI, 51.2–180.4; p = 0.003] and 103.3 [95% CI, 47.3–159.3; p = 0.002], respectively) (Table 2).
F-wave occurrence
There were no significant differences in F wave occurrence between the control (p = 0.532) and the acupuncture (p = 0.490) sessions (Table 2). There were also no significant differences in the change in F-wave occurrence from baseline to phases 1 (p = 0.656) and 2 (p = 0.488) between the two sessions (Table 2).
M-wave amplitude
There were no significant changes in M-wave amplitude in the acupuncture and control sessions (Table 2), and there were no significant interactions (p = 0.409). There were also no significant differences in the change in M-wave amplitude from baseline to phases 1 (p = 0.683) and 2 (p = 0.898) between the acupuncture and control sessions (Table 2).
Adverse events
No adverse events requiring medical attention were observed.
Discussion
To the best of the authors' knowledge, this is the first study to use F-wave measurement to examine the effects of acupuncture on the excitability of spinal motor neurons in patients with DOC accompanied by spastic muscle hypertonia.
Spastic hypertonia is a result of the exaggerated activation of stretch muscles and reduction of spinal inhibition caused by the upper motor lesions 41 because injury to cortical motor neurons and the corticospinal tract decreases the inhibitory effects of the motor cortex on the spinal anterior horn. The current findings indicated excessive excitability of spinal motor neurons caused by the upper motor neuron lesion, as the F/M ratio at baseline in the current study was higher than normal values described in previous reports (approximately 1–2). 42,43
The significant reduction in F/M ratio and mean F-wave amplitude during and after acupuncture treatment suggests that this treatment may reduce the excessive excitability of spinal motor neurons. The treatment may also help to treat muscle overactivity in patients with DOC following TBI by modulating motor neuron excitability.
Hand measurements of the F-wave parameter were used here because several studies have reported their usefulness in evaluating antispastic effects of various treatments, such as physiotherapy, medications, repetitive transcranial magnetic stimulation, and vibration therapy in stroke patients. 15,16,19,42 However, it is still controversial whether F-wave parameters recorded only from the abductor pollicis brevis muscle of the hand can indicate spastic muscle overactivity of the whole upper limb. The MAS, 30 which is used most commonly to evaluate spasticity in clinical situations, 44 was not used here because the score depends on the examiner's impression of passive movement and the reliability and validity of the scale have been previously questioned. 44 –46 In addition, the reduced ROM seen in patients enrolled in the present study can effectively prevent MAS measurement because the scores assume that measurement was performed through a full ROM (except in grade 4), and the reliability of this measurement may be influenced by the reduced ROM. 47 Although the current study did not include clinical assessments using neurologic scales for spasticity, the physicians and nurses observed a tendency for the passive ROM to increase in the upper limbs as a result of reduced muscle overactivity. Future studies with long-term observation and reliable clinical assessments are necessary to establish the clinical significance of acupuncture in spastic muscle overactivity through inhibition of the excitability of spinal motor neurons.
The mechanism by which acupuncture reduces spinal motor neuron activity is still unclear. The increase in F/M ratio observed in stroke patients has been reported to be suppressed by motor cortex stimulation, 42 while acupuncture and stimulation points have been reported to change motor cortex excitability. 48,49 Therefore, the alteration of motor cortex excitability could potentially be associated with a reduction in spinal motor neuron activity by acupuncture treatment in this study. However, this is merely a speculation because the current study did not measure cortex excitability. Further studies are required to investigate the mechanism of reduction of spinal motor neuron excitability.
All patients included in this study were already receiving central and/or peripheral muscle relaxants, including baclofen, a derivative of γ-aminobutyric acid, at spinal and supraspinal sites, and/or dantrolene sodium hydrate, which acts by abolishing excitation-contraction coupling in muscle cells. The patients also received rehabilitation, including muscle stretching therapy and ROM exercise for muscle overactivity. Therefore, the results of this study indicate that acupuncture may be useful as additional therapy that complements usual treatment and rehabilitation for spastic hypertonia in patients with chronic DOC following TBI.
Moreover, acupuncture for spastic muscle overactivity may not only be beneficial for patients with spasticity but also for medical staff and caregivers as severe spasticity can reduce the patient's ability to perform daily activities, thus increasing the burden on the caregiver. 5,12,13
These results should be interpreted with caution because this study has several limitations, including a small number of participants with heterogeneous TBI lesions and short period of observation using evoked electromyography. As stated earlier, the clinical effects on muscle overactivity were also unclear. Further research with long-term observation, more participants with homogeneous TBI lesions, and a blinded controlled design is required to elucidate the clinical efficacy of acupuncture in patients with DOC following severe TBI.
Conclusions
The overexcitability of the spinal motor neurons following severe TBI was reduced during and immediately after acupuncture treatment. This treatment may complement conventional therapy for refractory spastic muscle hypertonia occurring in patients with DOC due to severe TBI.
Footnotes
Acknowledgments
The authors thank Mr. Norio Nishiyama for technical assistance. They also thank all staff at the Chubu Medical Center and all participants in this study.
A part of this study was funded by ZENKYOREN (National Mutual Insurance Federation of Agricultural Cooperatives).
Author Disclosure Statement
No competing financial interests exist.