
Abstract
Objectives:
This study was implemented to evaluate the effect of individualized acupuncture treatment (AT) on functional dyspepsia (FD).
Methods:
A randomized, waitlist-controlled, two-center trial was performed. Seventy-six patients with FD were enrolled in the trial with partially individualized AT in a more realistic clinical setting performed twice a week for 15 minutes a session over 4 weeks. The participants were randomly allocated to a group receiving 8 sessions of AT for 4 weeks or a waitlist control group. After 4 consecutive weeks, the AT group was followed up without AT and the control group received the identical AT. The proportion of responders with adequate symptom relief, Nepean Dyspepsia Index (NDI), FD-related quality of life, Beck Depression Inventory, State-Trait Anxiety Inventory, Acupuncture Belief Scale, and acupuncture credibility test were assessed.
Results:
After the first 4 weeks, the proportion of responders significantly improved (59% in AT group [n = 37] versus 3% in control group [n = 39]; p < 0.001). The difference was no longer significant at 8 weeks, at which point the waitlist control group showed similar improvement after receiving AT (68% in the AT group versus 79% in the control group). Total NDI scores were significantly reduced in the AT group compared with the waitlist group (p = 0.03). Among NDI items, discomfort (p = 0.01), burning (p = 0.02), fullness after eating (p = 0.02), and burping (p = 0.02) were significantly improved in the AT group compared with the control group. No significant differences were observed between groups in other secondary variables.
Conclusion:
Individualized AT adequately relieves symptoms in patients with FD, and this effect may persist up to 8 weeks.
Introduction
F
Many patients with FD seek complementary and alternative treatments despite the availability of several conventional therapies 4 –7 because of the lack of satisfactory relief. 8 Among the many modalities of complementary and alternative medicine, acupuncture treatment (AT) has become globally considered a treatment option for FD treatment. 9,10
AT for FD has been practiced in Asia for thousands of years. 9,11 However, evidence for the therapeutic effects of AT is still limited by the lack of high-quality clinical trials. 10,12 Furthermore, few clinical trials reflecting the real practice of AT have been conducted to date. Previous studies examining the effect of AT on FD were not practical because they used unrealistically frequent AT sessions (e.g., five times per week) for outpatients and standard, nonindividualized acupoint settings using a fixed set of acupoints. This is in contrast to traditional individualized acupuncture treatments that allow the practitioners to decide the treatment plan based on the patient's symptoms at each session, including the selection of different acupoints. 13 –15 Therefore, a well-designed clinical trial is needed to study the effects of individualized AT on FD, which accurately reflects real clinical practice.
The aims of the present study were to determine whether individualized AT can improve FD when administered at a frequency similar to that seen in real practice.
Materials and Methods
Study design
The present study used a randomized, waitlist-controlled, clinical trial with 76 participants. Participants were allocated to one of two groups: the AT group or a waitlist control group. The AT group received acupuncture treatment for 4 consecutive weeks, followed by 4 weeks with no treatment. The control group received no treatment for the first 4 weeks and then was administered identical AT over the subsequent 4 weeks (Fig. 1). The entire study protocol was reviewed by the institutional review board of the Kyung Hee University Hospital at Gangdong, Seoul, Korea (KHNMC-OH-IRB 2013-006), and Kyung Hee University Medical Center, Seoul, Korea (KOMCGIRB-2013-05). The study protocol was registered in the web database on

Study design. AT, acupuncture treatment.
Participants
This study was conducted in two Korean hospitals: Kyung Hee University Medical Center and Kyung Hee University Hospital at Gangdong. Consent was obtained by the investigators, ensuring all participants volunteered freely, were fully informed on the specifics of the study, and were deemed capable of rational decision making.
Included participants were age 18–75 years, met the Rome III criteria, and had a score of 40 or more mm on the visual analogue scale for overall dyspeptic symptoms (0 mm indicates no dyspeptic symptoms and 100 mm indicates extreme dyspepsia). Participants were excluded in the case of structural gastrointestinal diseases, such as gastric cancer. Participants with other diseases that could interfere with acupuncture treatment (e.g., clotting disorders) were also excluded. Inclusion and exclusion criteria were detailed in the previous protocol study. 11
Randomization
A random allocation table sequence was created by an independent statistician using block randomization. Random numbers were generated by using the PROC PLAN of SAS 9.2 (SAS Institute, Inc., Cary, NC). Each number was hidden in a sequentially numbered opaque envelope until participant group allocation. A total of 76 eligible participants were randomly allocated to the AT or control group.
Intervention
Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture recommendations were used to summarize information detailing AT protocols (Table 1). 16
In the present study, partially individualized manual AT was used on the basis of traditional meridian theory, experts’ consensus, and previously reported evidence. 13 –15,17 AT was administered twice weekly for 4 weeks, and the number of acupoints per participant per session ranged from 9 to 19. The treatment acupoints consisted of 9 basic acupoints and 10 additional acupoints; the 9 basic acupoints were LI 4, ST 36, LR 3, SP 4 (bilaterally), and CV 12 (unilaterally) (Fig. 2A). The 10 additional acupoints included GB 21, SI 14, PC 6, EX-HN 5, and ST 34 (Fig. 2B). The additional acupoints were used only when participants had specific symptoms corresponding to specific acupoints, such as headache (EX-HN 5), shoulder or back pain (GB 21 and SI 14), nausea and/or vomiting (PC 6), and heartburn or epigastric pain (ST 34). The same number of ah-shi points in both medial scapular regions replaced acupoints GB 21 and SI 14 if there was obvious pressure pain at these sites.

Locations of basic and additional acupoints.
The symptoms requiring the selection of additional acupoints were examined by the clinical research coordinator to minimize the bias induced by contact between Korean medicine doctors (K.S.K. and J.S.W.) and participants. The only exception to this protocol was that back pressure pain was diagnosed by the acupuncture-administering doctors so that the selection of additional acupoints (GB 21 and SI 14) or ah-shi points could be determined.
AT was performed by the same doctors (K.S.K. and J.S.W.) at each hospital. Both doctors had undergone more than 10 hours of training and simulation to ensure that they were capable of providing identical AT in accordance with a predefined protocol.
Outcome measures
The proportion of responders (PR), the primary outcome, is defined as the proportion of participants who answered “yes” to half or more questions about adequate relief (AR) when assessed at 4 or 8 weeks. 18,19 Participants were asked to answer the following AR question at each visit (twice weekly for 8 weeks): “After the last visit, have you had adequate relief of your stomach pain or discomfort?” AR was determined before AT administration at every visit.
The Nepean Dyspepsia Index (NDI) consists of a symptom scale and a QOL scale and is a reliable, validated questionnaire used to quantify symptoms and QOL in patients with FD. 20,21 In this study, only the symptom scale was used in order to avoid duplication of QOL questionnaires. The Functional Dyspepsia-Related Quality of Life (FD-QOL) scale was developed to measure QOL of patients with FD. The Beck Depression Inventory (BDI), created by Aaron T. Beck, is one of the most widely used tools for measuring severity of depression in both research and clinical practice. 22 The State-Trait Anxiety Inventory (STAI) is a psychological assessment based on a 4-point Likert scale, consisting of 40 self-reported items aimed to evaluate degree of anxiety. 23 NDI, FD-QOL, BDI, and STAI were evaluated at baseline, 4 weeks, and 8 weeks. The Acupuncture Belief Scale is a 36-item, self-reported evaluation that assesses belief in the effectiveness of AT. 24 The Acupuncture Credibility Test, originally proposed by Vincent et al., consists of the following 4 queries: (1) expected improvement of FD; (2) willingness to recommend AT to others with FD; (3) AT reasonability; and (4) effectiveness of AT for other diseases. Acupuncture Belief Scale and Acupuncture Credibility Test were assessed once at baseline. 25 All outcome measures were detailed in the previous protocol study. 11
Sample size calculation
In the present study, a 60% PR from the AT group and up to a 25% PR from the control group were expected. These anticipated percentages were derived from previous studies
14,26
and a consensus of experts in clinical gastroenterology. In previous clinical research with similar experimental design, the waitlist control group achieved approximately 28% PR.
26
Significance was determined as α = 0.05, and a power of 1–β = 0.80 was used. Accordingly, the required sample size in this trial was estimated according to the following formula where (pt
+ pc
)/2:
Assuming pt = 0.6 (pt : the effect on the AT group) and pc = 0.25 (pc : the effect on the waitlist control group), a sample size of n = 30.1 is calculated to achieve 5% significance level and 80% power. Assuming a dropout rate of 20%, a total of 76 participants were needed with a 1:1 allocation to each group (38 participants per group).
Statistical analysis
All data are presented as means and standard deviations or percentages (%), and all analyses were based on an intention-to-treat principle. The “last observation carried forward” rule was applied. For the patients’ characteristics and outcomes, continuous variables were compared by using a two-sample t-test, Mann–Whitney U test, or analysis of covariance, and categorical variables were compared by using a chi-square test or Fisher exact test. In the case of intragroup analysis, the Wilcoxon signed-rank test was used. In a post hoc subgroup analysis compared subtypes of FD: postprandial distress syndrome (PDS) and epigastric pain syndrome (EPS). A p-value less than 0.05 was considered to indicate a statistically significant difference. A statistical analysis was performed by using PASW statistics, version 18.0 (IBM, Chicago, IL).
Results
Demographic characteristics
Between September 2013 and December 2013, 84 patients were screened, 8 of whom did not meet the inclusion criteria (Fig. 3). Seventy-six participants divided into 3 subtypes of FD (48 PDS, 0 EPS, and 28 mixed subtype) were enrolled and randomly assigned to the waitlist control group or the AT group. Seventy-two participants (95%) completed the study and 4 dropped out (5%) (Fig. 3). The initial levels of experimental parameters, including NDI and FDQOL, were similar between the groups at the beginning of the study (Table 2).
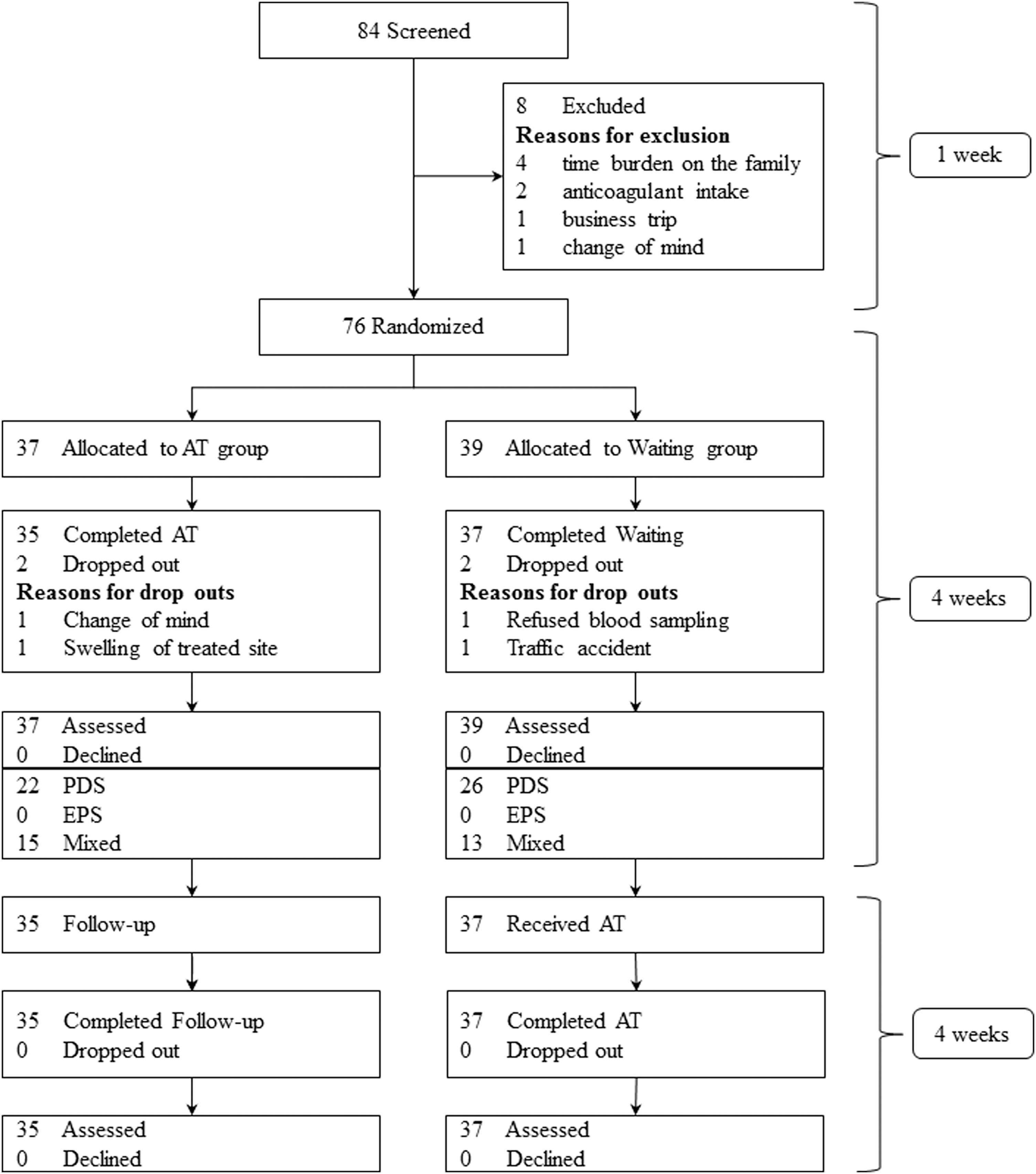
Trial flowchart. EPS, epigastric pain syndrome; PDS, postprandial distress syndrome.
Values are expressed as number (percentage) of patients or as mean ± standard deviation.
Mann–Whitney U test.
Chi-square test.
Fisher exact test.
Two-sample t-test.
Control, waitlist control group; AT, acupuncture treatment group; BMI, body mass index; VAS, visual analogue scale for dyspeptic symptom; NDI, Nepean Dyspeptic Index-Korean version; FD-QOL, Functional Dyspepsia–Quality of Life; STAI, State-Trait Anxiety Inventory; BDI, Beck Depression Inventory; ABS, Acupuncture Belief Scale; ACT, Acupuncture Credibility Test.
Proportion of responders
Twenty-two participants from the AT group (59.5%) responded positively to AT, whereas only one participant from the control group (2.6%) did so. At 4 weeks, the AT group showed a significantly higher PR than did the control group (p<0.001) (Fig. 4A and 4B). Additionally, the subgroups with AT displayed a significantly higher PR than did the control group at 4 weeks (p < 0.001 for PDS subtype and p = 0.007 for mixed type) (Fig. 4C). At 8 weeks, the AT group PR persisted at consistent levels, while the control group PR was markedly elevated (Fig. 4A and 4B).
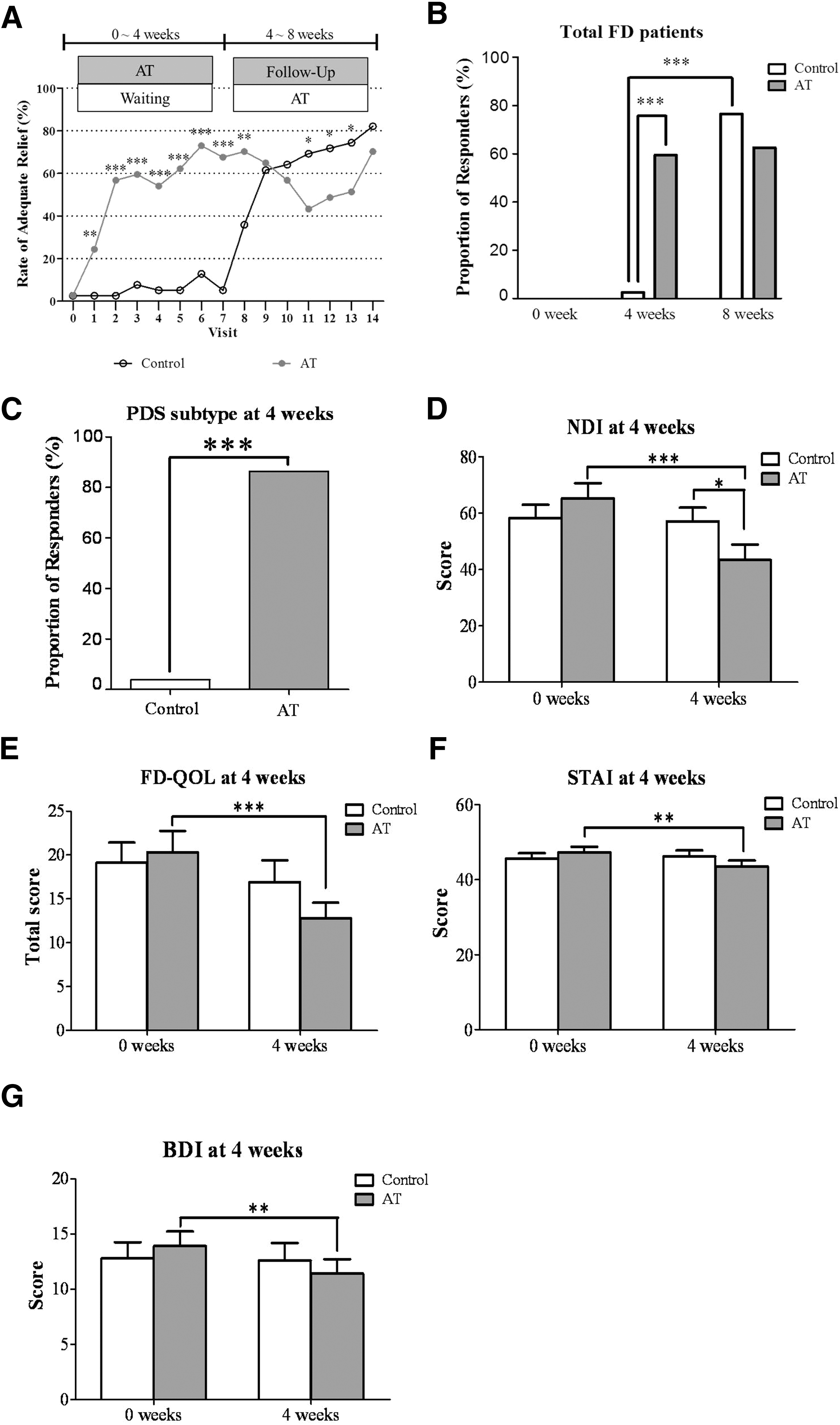
Main results of the present study.
NDI
The AT group presented a significantly lower total NDI score than the control group did after 4 weeks (Fig. 4D; Table 3). In subtype analyses, at 4 weeks, participants with PDS in the AT group reported significantly lower total NDI scores than did those with PDS in the control group (Table 4).
Values are expressed as mean ± standard deviation.
p < 0.05 versus control group analyzed by Mann–Whitney U test.
p < 0.05 versus baseline data of NDI items in AT group.
p < 0.05 versus 4 weeks’ data of NDI items in control group.
Values are expressed as mean ± standard deviation.
p < 0.05 versus control group, analyzed by Mann–Whitney U test.
Among the symptoms listed in the NDI, discomfort, burning in the upper abdomen, fullness after eating, and burping were significantly improved in the AT group at 4 weeks (Table 3). Similarly, discomfort in the upper abdomen, fullness after eating, pressure in the upper abdomen, and burping were among the NDI items that were significantly improved in patients with the PDS subtype in the AT group at 4 weeks (Table 4). Total score and severity of NDI symptoms did not differ between the two groups at 8 weeks (Table 3).
FD-QOL
The difference of total score for FD-QOL was not significant between the AT group and control group at 4 weeks (Fig. 4E). In subtype analyses, the QOL score was significantly improved in the PDS subtype of the AT group (p = 0.014). At 8 weeks, there was no significant difference in FD-QOL between the two groups.
BDI
The BDI score did not significantly differ between the AT group and the control group or between any subtypes of either group at 4 weeks (Fig. 4F).
STAI
There was no significant difference in STAI score between the AT group and the control group or between any subtypes of the 2 groups at 4 weeks or 8 weeks (Fig. 4G).
Belief in and credibility of acupuncture treatment
General beliefs in/expectations regarding the benefits of AT for general health were similar between the two groups (p = 0.112) and between the responders and nonresponders for each group (p = 0.258 and p = 0.493 in the AT and control groups, respectively). Regarding the credibility of AT for FD, there was no difference between the two groups (p = 0.207) or between the responders and nonresponders from each group (p = 0.248).
Adverse events
Reported adverse events did not significantly differ between the two groups (36 cases in AT group versus 42 in control group). Nausea, vomiting, and diarrhea occurred in the AT group (5 cases total), and abdominal pain and other gastrointestinal symptoms occurred in the control group (9 cases total) between 0 week and 4 weeks. However, there were no serious adverse events in this trial.
Discussion
These results demonstrated that twice-weekly individualized acupuncture for a month significantly improved clinical outcomes (PR and overall symptoms of FD) and that the beneficial effects persisted for 4 more weeks after treatment. Similar improvements were also observed in the control group when the identical AT was administered after a 4-week waiting period.
Although recent clinical trials studying headache, allergic rhinitis, and osteoarthritis have adopted individualized AT regimens, 27 –29 a partially individualized AT was applied to patients with FD for the first time in this study; in contrast, previous protocols used only fixed acupoints in AT trials for FD. 13 –15 In this study, the basic nine fixed acupoints were selected on the basis of traditional meridian theories, results of previous studies (e.g., ST 36 and CV 12), 13 –15,17 and the consensus of acupuncture experts in Korea. Additionally, a maximum of 10 other matching acupoints could be used for treatment, depending on the existence of additional individual symptoms that frequently accompany FD. These AT conditions were considered reflective of real practice AT for FD.
The current study did, however, try to maintain consistent AT for FD through the selection of basic common acupoints irrespective of differences in FD symptoms and through use of individualized AT by matching additional nondyspeptic symptoms with previously determined corresponding acupoints. In this study, nondyspeptic symptoms, such as headache (13.5%–5.4%), nausea and/or vomiting (13.5%–8.1%), heartburn (24.3%–16.2%), and shoulder and/or back pain (78.4%–73%) were also improved because of the partially individualized AT. Unlike in recent AT studies on FD, 13 –15 the frequency of AT in this trial was twice weekly because this is considered the most realistic frequency for an outpatient's adherence to therapy in actual practice. Thus, this study demonstrates that real-practice AT could be effective on both dyspeptic and nondyspeptic symptoms of FD.
At the design stage of this study, it was expected that approximately 60% of the participants in the AT group would respond to acupuncture compared with up to 25% in the waitlist group. 14,26 However, only 3% of the participants in the control group achieved adequate relief at 4 weeks. Such a discrepancy requires careful interpretation: A large response discrepancy in waitlist group between our study and Kaptchuk and colleagues’ trial 26 (3% versus 28%) might be due to different conditions investigated (FD versus IBS), natural course of disease and symptom fluctuations, different treatment periods (4 versus 3 weeks), and varying expectations and cultural backgrounds. Therefore, the current study tried to minimize the possible effects except for AT (e.g., establishment of minimal contact between doctor/practitioner and participants, measurement of expectation and credibility of AT, and check-out of dropout rate). As a result, credibility of or expectations of AT and dropout rate between the two groups were similar. However, a future study with a sham acupuncture control will clarify whether the present finding is specific to AT or mainly due to nonspecific (i.e., placebo) effects.
The selected acupoints used in this trial (e.g., ST 36, PC 6, and CV 12) have already been shown to have a positive effect on gastric slow wave and gastric emptying. 17,30 ST 36 is known to improve impaired gastric slow wave, delayed gastric emptying, impaired gastric accommodation, and gastric motor migrating complex, 31 –34 and PC 6 can also improve postoperative nausea/vomiting and delayed gastric emptying. 33,35 Therefore, although it is difficult to generalize the current results because of small sample size and short periods of treatment and follow-up, these results showed that AT could be an ideal therapeutic option for FD, especially PDS subtype.
This study did verify site specificity on acupoints, although many acupuncture researchers have noted the specificity of ST 36 and PC 6 for improvement of gastric function 30 –35 and stress reduction. 36 To maximize the effect of AT on FD, acupoints were selected on the basis of sites reported to be linked to gastric function (ST 36, PC 6, and CV 12), 17,30 frequently used empirical acupoints for relieving dyspeptic symptoms in real clinical practice (SI 14, GB 21, and EX-HN 5), and acupoints selected according to traditional acupuncture theory (LI 4, ST 34, LR 3, and SP 4). The approach used here highlights that a substantial gap remains between AT research focused on specific mechanisms and AT in real clinical practice. It can be argued that this gap has caused the discrepancy in the effectiveness and benefits of AT for treatment of FD observed by scientific researchers and clinical practitioners. To elucidate the causes of this observed incongruity, a carefully designed study incorporating a placebo control should be conducted to identify the discrepancies between the two AT approaches.
Despite encouraging findings in this trial, some limitations should be noted. First, no placebo control was used. There are about five methods for placebo in acupuncture studies: four skin-puncturing methods and one nonpenetrating method. 37 However, simple insertion of a needle into skin induces a physiologic response that may result in a variety of nonspecific effects. 38 Therefore, futures studies using stringent research design, including various types of placebo (skin-puncturing and non–skin-puncturing methods) are needed. Additional limitations to the current study include a relatively short study period and a localized ethnic group. Future studies with a larger, multinational sample group and a long-term clinical trial investigating a specific mechanism are necessary.
In conclusion, individualized acupuncture improved overall FD symptoms, and its effect persisted for 4 more weeks. AT was effective in improving individual FD symptoms, such as discomfort in upper abdomen, fullness after eating, burping, and burning. Future studies examining the effect of AT on FD that apply the same interventions and settings but with a longer study period, and with a valid placebo control, will determine the specific effect of AT on FD.
Footnotes
Acknowledgment
This work was supported by the National Research Foundation of Korea grant funded by the Korean government (Ministry of Science, ICT & Future Planning) (no. 2005–0049404).
Author Disclosure Statement
No competing financial interests exist.