
Abstract
Objective:
To evaluate the effect of micronutrients (minerals and vitamins) on adult psychosis when added to conventional medications by using a placebo-controlled randomized design with a 1-month open-label run-in.
Design:
Longitudinal comparison study following a randomized, controlled trial that had failed because participants declined to undergo randomization.
Setting/Locations:
Rural primary care and psychiatry clinic in northern New England (town of 16,000 people).
Participants:
People older than age 18 years diagnosed with a psychotic disorder who were receiving medications.
Intervention:
Fifty consecutive clients seen in 1 month's time were invited to participate; 19 completed a 1-month open-label phase of the addition of a micronutrient to their medication regimen; all 19 then withdrew rather than risk randomization to a placebo. This finding itself was important, so the study was restructured to compare the response of those 19 patients during 24 months of micronutrients + medication to the response of the 31 people who declined participation, enriched by an additional 28 consecutive patients recruited over the second month of the study. This yielded a total of 59 patients who received medication without micronutrients.
Outcome measures:
All clients were evaluated with the Positive and Negative Symptom Scale and the Clinical Global Impression scale at study baseline and after 3, 6, 9, 12, 15, 18, and 24 months. Psychosis was confirmed with clinical interview by using Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision, criteria. All participants had normal physical examinations and laboratory studies.
Results:
Outcomes were similar for both groups until 15 months, although the micronutrient group used significantly less antipsychotic medication throughout that time (p < 0.001). At 15 months, the micronutrients + medication group exhibited significantly fewer symptoms than the medication-only group, a difference that was even stronger at 24 months.
Conclusions:
Micronutrients may appear to be a beneficial long-term, adjunctive strategy for people with psychotic disorders, allowing for smaller doses of medication to achieve the same effectiveness with fewer side effects.
Introduction
T
A fourth and important reason is the solid biologic rationale for considering micronutrients for treating mental health problems. A review by Ames and colleagues showed that as many as one third of known genetic mutations resulted in the corresponding enzyme having an increased Michaelis-Menten coefficient, or Km, which results in decreased binding affinity for a coenzyme, and then a lower rate of reaction. 5 At least 50 human genetic diseases caused by defective enzymes can be remedied or ameliorated by the administration of high doses of the vitamin component of the corresponding cofactor, which at least partially restores enzymatic activity.
Other scientific findings form the context for treating with nutrient therapy. At the population level, diets higher in vegetables and fruits are associated with lower depression and anxiety, whereas diets low in vegetables and fruits and higher in processed foods are related to higher rates of depression and anxiety. 6 Longitudinal studies have shown that these dietary patterns have preceded the onset of psychiatric symptoms, 7 suggesting a causal relationship. One hundred years of scientific research provided promising (though modest) results of treating mood swings and irritability with single nutrients. 8 In contrast, research since 2000 on formulas with more than 25 minerals and vitamins (referred to as broad-spectrum) has shown much larger effects. 9 More than 20 randomized controlled trials (RCTs) show that micronutrients are beneficial in treating stress, anxiety, aggression, low mood, autism, and attention-deficit/hyperactivity disorder. 10 One RCT showed that a 25-ingredient micronutrient formula plus some omega-3 fatty acids (eicosapentaenoic acid and docosahexaenoic acid) resulted in roughly a one-third reduction of aggressive offenses in young adult prisoners. 11 In another setting, micronutrients had a statistically significant impact on emotions and stress related to the 6.3-magnitude earthquake on February 22, 2011, in Christchurch, New Zealand. 12 These postdisaster results were replicated in a general population following a destructive flood in southern Alberta, Canada. 13
One final example of an RCT with a broad-spectrum formula was reported in adults with attention-deficit/hyperactivity disorder. 14 Those consuming the active formula showed greater reductions in symptoms than those taking placebo, with medium-to-large effect sizes. In a subgroup that entered the trial with moderate to severe depression, twice as many people went into remission in the micronutrient group compared with the placebo group. Importantly, the benefits of micronutrients continued through the 1-year follow-up. 15
Finally, two case studies are relevant because both demonstrated complete remission of psychotic disorders, and both used the same broad-spectrum formula employed in the current study. In one case, a child was treated unsuccessfully with conventional medication from age 6 to 12 years; 16 subsequent treatment with micronutrients alone resulted in complete recovery of mental health. Similarly, a 10-year-old boy treated with conventional medications as an inpatient in a tertiary care pediatric hospital for 6 months showed no improvement in symptoms such as hallucinations, delusions, and obsessive-compulsive disorder. 17 When discharged to outpatient care and treated with micronutrients alone for the immediately subsequent 6 months, he became well; 7 years he later graduated from high school. In this case, a health economist determined that his 6 months of successful micronutrient treatment cost less than 2% of the prior 6 months of unsuccessful conventional medication treatment. Both of these cases have been followed for a minimum of 7 years, and both boys remain well as long as they take their micronutrients. No cases of adult psychosis have yet been published.
A pilot RCT was designed to determine feasibility of a larger RCT, the time course of action of micronutrients, and effect size to aid in designing future studies.
Materials and Methods
Design
A randomized, placebo-controlled trial was initiated, with a 1-month run-in period of open-label exposure to the active treatment. The trial was designed as a pilot study of 50 patients being treated with conventional psychiatric medications. The study was reviewed and approved by the authors' institutional review board. Each participant signed a consent form indicating willingness to participate in a study with a 1-month open-label exposure to a broad-spectrum micronutrient formula, followed by randomization to that formula or a placebo. All participants continued with their conventional psychiatric medications with a treatment philosophy of using the lowest dose compatible with acceptable symptom reduction.
In the initial month of the study, 19 of 50 patients accepted the micronutrient. At the 1-month mark, none would agree to randomization. These were two important findings. First, it might not be feasible to do a larger RCT in this population, as 31 of 50 people were reluctant to participate in a study that would require taking more pills in addition to their conventional psychiatric medication. Second, those who did take the micronutrient formula for 1 month found it sufficiently beneficial that none were willing to proceed to the randomization phase, where there was a 50% chance of being assigned to the placebo group.
As a result of this experience, the study was reconfigured as a longitudinal comparison study that would follow the 19 patients who were taking micronutrients and compare them to the 31 who had not for as long as follow-up was feasible. To the group receiving medication without micronutrients, 28 consecutive patients were added to reduce any inherent differences between people who will take micronutrients and people who will not. The ethics protocol was revised to be simply the comparative analysis of data between the two groups over time. The same psychiatrist (L.M.-M.) managed all patients with the same treatment philosophy. Individual and group psychotherapy was available for all patients. The research objective was modified to determine whether adding a micronutrient formula to standard treatment would improve response without producing side effects in comparison to a group receiving only conventional treatment. As with the initial plans for the RCT, the goals continued to be (1) to determine the feasibility of a larger trial, (3) to determine the time course of action of the micronutrient formula, and (3) to find the effect size that would inform a future sample size.
Participants
The practice setting was an integrated medical and mental health clinic in a small, rural, northern New England town (population 16,000). Federal and/or state government health insurance funded 86% of the patients. The remainder had private or no health insurance. Thirteen of the 31 who declined micronutrients did so because they didn't want to take so many pills. Nine patients declined because they “had a real problem” and felt trivialized by an offer to treat the seriousness of their disorder with micronutrients. Nine declined because they had previously tried some forms of vitamins that had not been beneficial. The demographics of patients are described in Table 1. No substantial differences emerged between the two groups.
p < 0.01.
p < 0.001.
SD, standard deviation.
Confirmation of diagnosis
All participants had a preexisting diagnosis of a psychotic disorder, which was confirmed by history and assessment. No patients in this sample were having their first psychotic episode. All participants met the criteria for a psychotic disorder described in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision. 18 For the 19 who volunteered for the RCT, the diagnoses consisted of schizophrenia (n = 4), schizoaffective disorder (n = 3), bipolar disorder with psychotic features (n = 10), and psychosis not otherwise specified (n = 2). For the 31 who were treated only with medication, the diagnoses consisted of schizophrenia (n = 5), schizoaffective disorder (n = 5), bipolar disorder with psychotic features (n = 18), and psychosis not otherwise specified (n = 3). There was no difference in the distribution of diagnoses. The authors screened out all patients who had not had at least three psychotic episodes, in keeping with a developing perspective of a transdiagnostic spectrum between schizophrenia and bipolar disorder, with overlapping affective and nonaffective psychotic symptoms. This is in keeping with recent data questioning the Kraepelinian dichotomy between schizophrenia and bipolar disorder. 19 For the 28 consecutive patients who were added to enrich the medication-only sample, the diagnoses were schizophrenia (n = 9), schizoaffective disorder (n = 9), bipolar disorder with psychotic features (n = 2), and psychosis not otherwise specified (n = 8). * There were insufficient numbers to make comparisons across diagnostic codes.
Physical and laboratory assessments
Baseline assessments consisted of history and neurologic and physical examinations. Screening procedures included a complete blood cell count; measurement of glucose, electrolytes, blood urea nitrogen, fasting glucose, and creatinine; liver function tests; homocysteine and methylmalonic acid levels; thyroid-stimulating hormone; and urinalysis. Each participant had previously undergone magnetic resonance imaging or computed tomography to confirm structural normality, or one of those examinations was ordered. All values were within normal limits and remained there regardless of the intervention administered.
Micronutrient management
The authors selected a broad-based micronutrient supplement (EMPowerPlus Advanced Formula) that encompassed all known dietary vitamins and a broad spectrum of minerals and trace elements (Fig. 1). The dosage was 4 capsules of the advanced formula twice daily. All patients were also offered a fish oil supplement provided by the same manufacturer. They were encouraged to consume enough capsules to provide them with 2000 mg eicosapentaenoic acid daily. All patients were receiving public assistance or no assistance and could not afford to buy any additional micronutrients than what was provided to them via the study. None were employed on a regular basis.
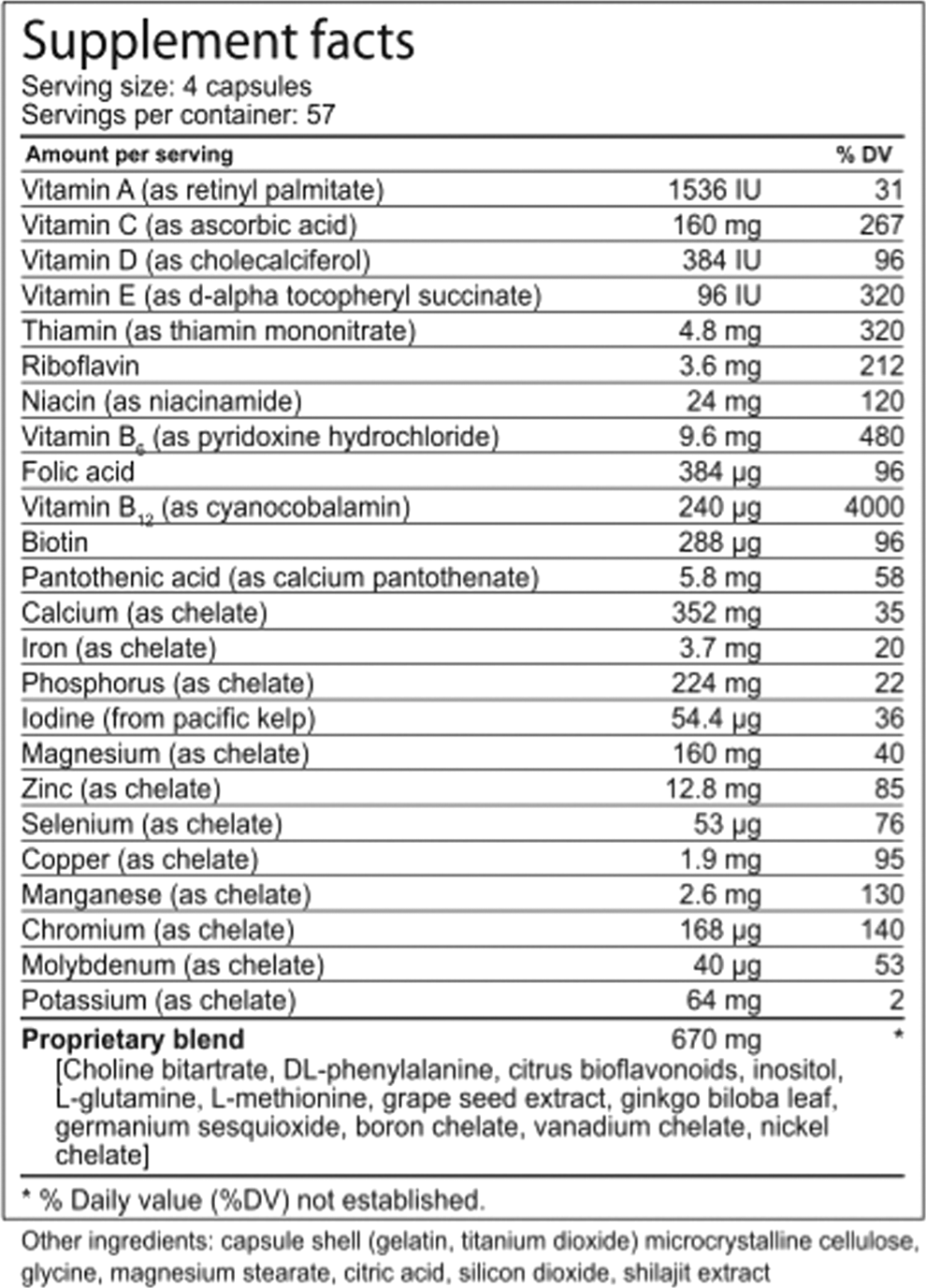
Contents of the micronutrient formula.
Medication comparisons
For calculation of dose across participants, all medications were converted to haloperidol equivalents using a standardized, validated method. 20
Measures
The primary outcome measures were scores on the Positive and Negative Syndrome Scale (PANSS) 21 and Clinical Global Impression scale (CGI), 22 which were collected at study baseline and after 3, 6, 9, 12, 15, 18, and 24 months of study participation. Secondary safety and tolerability outcomes included incidence of serious adverse events; incidence of treatment-emergent adverse events; and changes in weight, measures of neurologic side effects, and laboratory analyses.
Secondary measures included the Measure Yourself Medical Outcome Profile (MYMOP), version 2 (MYMOP2), a patient-centered, problem-specific outcome measure that provides a useful and sensitive measure of change in perceived symptoms and quality of life. 23 –25 In the current study, participants used the MYMOP2 to choose one or two symptoms of most concern, along with one activity of daily living that was restricted or prevented by these symptoms. The client scored these items according to their severity in the last week by using a 7-point Likert scale ranging from 0 (as good as it can be) to 6 (as bad as it can be). They also rated their general feeling of well-being. Measures were taken before the first treatment (baseline) and at each follow-up period.
The MYMOP2 has been used in clinical audits in the United Kingdom to improve patient care, 26 to show that acupuncture benefited people with chronic illness, 25 and to assess overall outcomes in a complementary care clinic. 27 In all these contexts, the MYMOP2 provided an opportunity to assess overall improvement in symptom severity, the degree to which symptoms restrict participation in desired activities, and overall quality of life in cases in which the symptoms themselves may be radically different. The use of symptom-specific scales in these cases would result in insufficient numbers of participants for comparison purposes and also prevent across-illness comparisons. The MYMOP2 is considered useful for “real-world” situations in which clinicians apply the same treatment methods (group therapy, talking circle, acupuncture) to a variety of different patients and conditions, all with the same goal of reducing their suffering and improving their quality of life. Sex, age, occupation and marital status were recorded.
Independent-samples t-tests were used to compare the differences in outcome measures at each evaluation point. The power to detect an effect at 15 months was 95%, with an effect size ranging from 1.2 to 1.35.
Common therapies available to all participants
All participants received dietary counseling to reduce their intake of simple carbohydrates and to increase their intake of lean protein and vegetables. Individual and group therapies were available to all participants. Group therapies included some instruction in meditation, chi gong, and yoga. There was no disproportionate enrollment of participants taking micronutrients in these services.
Results
The medication and the micronutrient groups did not differ on any demographic variable (Table 1). Statistically significant differences emerged in the reasons for discontinuations, with side effects being prominent among those taking only medications and markedly less among those also taking micronutrients. By 15 months' follow-up, patients also taking micronutrients were scoring significantly better on all measures (PANSS, MYMOP, and CGI) than patients taking only medications, which continued at 24 months (Tables 2 –4). Changes were noted earlier on the CGI, with significant differences emerging at 6 months (Table 3). Significant changes in medication dosage emerged at 6 months (effect size, 0.6 range) and continued to widen through the 15-month follow-up. The gap was narrower at 24 months because many patients in the medication-only group had stopped their treatment. During the first year of follow-up, there were three hospitalizations in the medication-only group and one hospitalization in the micronutrients + medication group. During the second year of the follow-up, there were four hospitalizations in the medication-only group and two in the micronutrients + medication group. The effectiveness of medication tended to diminish in the medication-only group and at around 12 months, a number began a second medication, which was increased while the first medication was decreased; this resulted in an increase in medication dose, which then dropped when the first medication was tapered fully (Table 5; Fig. 2).
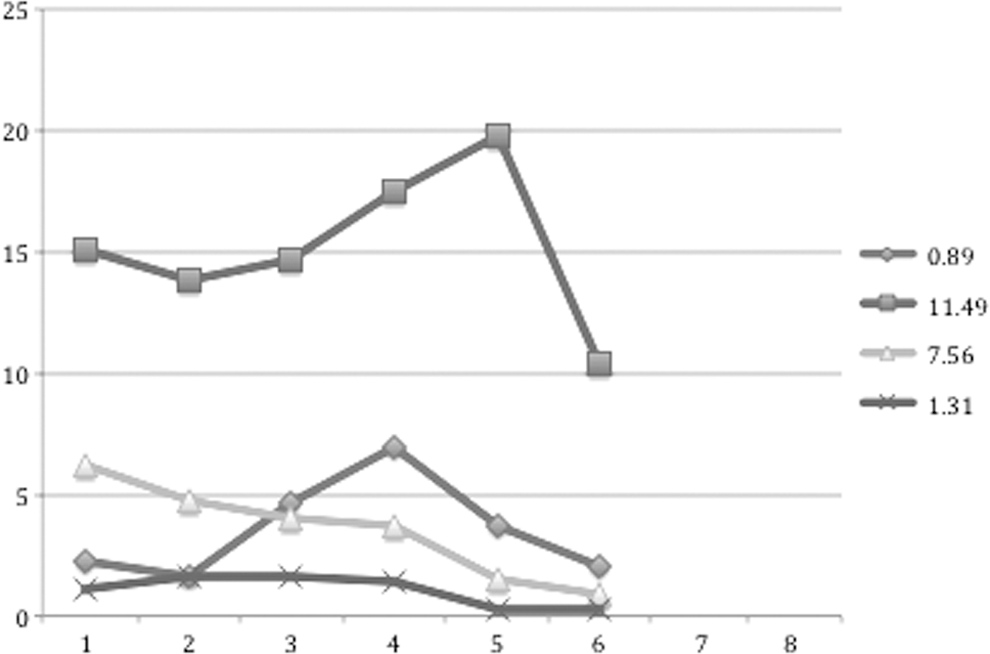
Comparisons of medication doses between medication group only and medication + micronutrients group. Lower lines represent the dose minus the standard deviation. Data were collected at baseline and 3, 6, 9, 12, 15, 18, and 24 months. Doses are in haloperidol equivalents.
p < 0.001.
SEM, standard error of the mean.
p < 0.01.
p < 0.001.
p < 0.001.
MYMOP, Measure Yourself Medical Outcome Profile.
p < 0.01.
p < 0.001.
Discontinuation of micronutrients
Six of 19 patients discontinued micronutrient treatment. One patient did so because her psychotherapist was critical of micronutrients and convinced her to rely only on medications. Her level of distress worsened when she stopped the micronutrients, and distressing, critical voices returned. Another patient stopped the micronutrients because she felt guilty about feeling better. Her grandparents had been in the Holocaust and her voices were telling her she needed to suffer because they had. The voices were upset that she was feeling better on the micronutrients and convinced her to stop them. Her symptoms worsened upon doing that. One patient was able to eliminate antipsychotic medication with the use of micronutrients over the course of a year. Then he became convinced that he had to also eliminate micronutrients and all other nutritional support. He did so and began to isolate himself. Six months later, he fell in love with someone who did not reciprocate. He began to follow her and was eventually involuntarily admitted to the hospital.
Another patient was able to reduce his antipsychotic dose to the level at which he was having erections again. He was doing very well until he moved into a house with a female roommate with whom he became sexual. This terrified him and he stopped all his medication and was readmitted to the hospital within 2 weeks. Another patient consistently refused antipsychotic medication. He did better on micronutrient therapy but did not believe he needed anything. He started and stopped micronutrients at intervals of every 2 months. He was intermittently hospitalized, averaging 1.5 times per year. A final patient stopped because he felt guilty about not paying for the micronutrients even though he was reassured that he was part of a study and did not need to pay. He did better with the micronutrients and was able to take a lower dose of antipsychotics.
Discussion
Adding micronutrients to conventional treatment resulted in significantly better symptom management than conventional treatment alone over time. The addition of micronutrients also permitted a lower dose of conventional medications that was apparent at 3 months and statistically significant at 6 months. The results suggest that micronutrients may have a greater potential in biological psychiatry than has previously been realized. Previous studies have focused on one nutrient at a time; patients who are deficient in one nutrient are likely deficient in others, so supplementing with one nutrient may be an inadequate strategy.
Our pilot study showed that a larger RCT might be feasible without an open-label run-in design. However, time matters. The typical pharmaceutical study lasts 6–12 weeks. Micronutrient effects may take longer to appear in this population. Another challenge is that not all patients will agree to take more than one pill per day. Also, not all patients can remember to take micronutrients every day. Some patients with psychotic disorders stopped treatment when they improved for a variety of reasons, so dropping out of treatment, for micronutrients, or for medications was not always an indication that the treatment had not worked or that unacceptable side effects had occurred. Importantly, almost no side effects were seen with micronutrients, and it was possible to decrease the dose of conventional medication needed to achieve a therapeutic benefit, which was associated with reduction in dose-related side effects.
With larger sample sizes, an effect might be detectable before 15 months. The level of medication use, however, did become significantly different at 6 months and continued to widen without any increase in hospitalization rates among those receiving lower doses of medication (Table 5).
One limitation of this study was that the same psychiatrist (L.M.-M.) prescribed for everyone. His enthusiasm about micronutrients could have made their effect stronger than might be seen if a skeptic were prescribing (a study that could be done). Although he believed that he strove for the best possible outcome for all patients and tried consciously to be equally positive to all, that potential source of bias cannot be ruled out. However, were enthusiasm to produce such large differences in medication response—that would also be worthy of study and comment.
Often, micronutrient therapies are dismissed because of the smaller number of studies and perhaps also related to an intrinsic bias in favor of pharmaceuticals. Increased pharmaceutical advertising among 11 major U.S. medical journals was associated with their publishing fewer articles about micronutrients and publishing more articles with conclusions that micronutrients were unsafe. 28 Certainly, industry research funding is biased away from micronutrients because no new patents are possible for these compounds. However, in the interests of improving patient care with little or no risk of adverse events, further studies on this topic are warranted.
Given the exploratory nature of this study, some variables were not assessed. The study did not assess the contribution of self-awareness, sense of rightness in the body, suggestibility level, or hopefulness in influencing outcome.
Conclusions
Micronutrients appear to be useful adjuncts to psychotropic medications in the long-term treatment of psychosis. Patients taking micronutrients dramatically reduced their dose and experienced fewer side effects than those taking only medications. Further research is indicated.
Footnotes
Acknowledgments
The authors acknowledge support from TrueHope Nutritional Support Ltd, Raymond, Alberta, in the form of free bottles of EMPowerPlus and omega-3 fatty acids for administration to participants. Coyote Institute provided general operating funds for the study.
Author Disclosure Statement
No competing financial interests exist.