
Abstract
Objectives:
This project was designed to assess the quality of care received by patients with depression and anxiety who were seen by naturopathic physicians in a community health center.
Methods:
The Natural Medicine Quality Improvement Project for the Treatment of Depression and Anxiety (NMQP-DA) was conducted over a 26-month period from December 2009 through February 2012 at HealthPoint, a non-profit, consumer-governed, community health center network located in suburban King County, Washington. A total of 112 patients enrolled in the NMQP-DA, and 60 were seen for two or more visits, thus meeting eligibility criteria for inclusion in the study. The mean number of visits was 3.3. The Patient Health Questionnaire (PHQ-9) depression screener and the Generalized Anxiety Disorder 7-item scale (GAD-7) anxiety screener were the outcome measures.
Results:
The overall improvement in symptoms of depression and anxiety was highly significant (p < 0.0001) when comparing the group's average initial screener scores to their average final screener scores for both depression (16.4 vs. 8.6) and anxiety (12.4 vs. 7.2). The response rate, as measured by a 50% decrease in scores, for those with initial scores ≥10 was 58.6% for depression (PHQ-9) and 50% for anxiety (GAD-7).
Conclusions:
This study adds new data to the limited literature on the nature and effectiveness of naturopathic medicine to treat anxiety and depression in the context of an integrative community health center.
Introduction
M
Studies on the prevalence of complementary and alternative medicine (CAM) use in the United States suggest that 4/10 adults use CAM as a part of their healthcare. Surveys of CAM use for mental-health conditions in the United States found that 15% of those surveyed use CAM to treat mental or emotional problems. 8,9 In a nationally representative survey of 2055 respondents, 56.7% of those with anxiety attacks and 53.6% of those with severe depression reported using CAM in the past 12 months. 10 When patients were asked their reasons for using CAM, commonly cited responses were belief in its efficacy and ability to resolve symptoms more quickly than conventional care, dissatisfaction with conventional care, desire to work cooperatively with their physician, decreased side effects from treatment, and a desire to improve overall health. 11,12 In a review of 2543 older adults who used naturopathic medicine services in the Seattle area, anxiety and depression were among the top five reasons for seeking care. Participants reported that the reason they sought naturopathic medicine services was because it offered a different system of care aligned with their values. 13 CAM use is one way that patients are attempting to expand their care for a mental-health disorder. There is an increasing body of evidence supporting the efficacy of some CAM treatments for both depression and anxiety, further validating this patient preference for CAM mental-health treatments. 14 –19 In a small observational pilot study from Australia, a potentially beneficial effect was found for naturopathic medicine for reducing depressed mood, anxiety, and stress. 20 CAM treatments are generally low risk, low cost, and well received by patients. 21
The American Association of Naturopathic Physicians defines naturopathic medicine as a distinct system of primary healthcare—an art, science, philosophy, and practice of the diagnosis, treatment, and prevention of illness. Naturopathic medicine is distinguished by the principles upon which its practice is based. These principles are continually reexamined in the light of scientific advances. The techniques of naturopathic medicine include modern and traditional, and scientific and empirical methods. The following principles are the foundation of naturopathic medical practice: the healing power of nature (vis medicatrix naturae), identify and treat the causes (tolle causam), first do no harm (primum non nocere), doctor as teacher (docere), treat the whole person, and prevention. 22
As of 2010, 17 U.S. states, the District of Columbia, and two U.S. territories license naturopathic physicians. 23 Naturopathic physicians (NDs) take a holistic approach to the care of their patients and integrate both natural and conventional medicine treatment options. The scope of practice of naturopathic physicians encompasses multiple modalities, including diet and nutraceuticals (vitamins, minerals, and nutritional supplements), herbal medicine, homeopathy, hydrotherapy, mind–body medicine, physical medicine, and pharmaceuticals. Currently, there are a limited number of integrative clinics and hospitals nationwide that employ naturopathic physicians. 24 To date, there is a paucity of research examining the nature and efficacy of mental healthcare provided by naturopathic physicians in such settings. 25
Washington State licenses a large number of practicing naturopathic physicians in the United States and is home to a unique integrative community health center network, HealthPoint, which employs naturopathic physicians as PCPs. 23 This community health center system served as an ideal venue to conduct a small study evaluating the efficacy of naturopathic treatment for anxiety and depression. This descriptive report evaluates patient outcomes of naturopathic physicians and explores physician-directed natural medicine utilization by patients with anxiety and or depression.
Materials and Methods
The Natural Medicine Quality Improvement Project for the treatment of depression and anxiety (NMQP-DA) was conducted over a 26 month period from December 2009 through February 2012 at HealthPoint, a non-profit, consumer governed, community health center network located in suburban King County, Washington. At the time of the study, HealthPoint had 12 centers delivering medical, dental, and complementary healthcare services to >60,000 patients annually. Health services are delivered in the preferred language of the patient through the use of interpreters to any individual or family in need, regardless of their ability to pay. Target populations are low-income, uninsured, minority, refugee, and homeless individuals and families in King County, outside the city limits of Seattle. In a report by the Kaiser Commission on Medicaid and the Uninsured, community health center patient populations were analyzed and compared to the low-income population overall. Community health centers are described as a key source of comprehensive primary care in medically underserved communities across the country. Compared to the low-income population overall, health center patients are more disadvantaged. They are poorer, more racially and ethnically diverse, and more likely to be unemployed and uninsured than the broader low-income population is. 26
Starting in December 2009, patients at HealthPoint undergoing usual naturopathic care who had symptoms of anxiety or depression assessed through history taking during their patient visit were asked to fill out a packet of validated screeners, including the Patient Health Questionnaire (PHQ-9) depression screener, the Generalized Anxiety Disorder 7-item scale (GAD-7) anxiety screener, the Mood Disorder Questionnaire (MDQ) bipolar screener, and the GAIN-SS substance use screener.
27
–30
See the appendixes for copies of the PHQ-9 (Appendix 1 is available online at
Demographic detail, care team composition, medication prescriptions (including both natural and pharmaceutical medications), and treatment modality utilization were extracted from the electronic medical record. A chart review was also conducted to identify the provider type at initial clinical contact and to attempt to identify possible reasons for lack of follow-up visits. A comparison of the initial screener scores of the eligible participants and the group with only one visit was conducted using an unpaired t-test. Analysis of the difference between initial and final screener scores using a paired t-test was calculated for the eligible participants—those patients meeting eligibility criteria with two or more visits with a naturopathic physician. The response rate, as measured by a 50% decrease in PHQ-9 or GAD-7 scores, was calculated for those with initial scores ≥10.
Results
Demographics
A total of 112 patients were enrolled in the NMQP-DA over a 24-month period, starting in December 2009 and ending in December 2011. Of these, 54% were seen for two or more visits, with a mean of 3.3 visits. Eligible participants, those seen for two or more visits by a naturopathic physician, were predominantly female, single or divorced, with an average age of 44 years. English was the most common language spoken, though 1/5 participants spoke Spanish. Approximately one-third of the participants identified as ethnically Hispanic. The racial distribution was predominantly white, and 47% had incomes at or below the federal poverty level, which at the time of the study was $22,050 for a family of four. The majority of the group (55%) had no insurance, 13.3% had public insurance, and 30.0% had commercial insurance. Some differences were noted when comparing the eligible group to the group with only one visit with a naturopathic physician. The group with only one visit had fewer women (75% vs. 82%), and participants were 20% more likely to be single. The group with only one visit also had a higher percentage of individuals at or below the poverty level, and participants were 50% less likely to have private insurance. An unpaired t-test comparing initial screener scores (GAD-7 and PHQ-9) of the group with only one visit to the eligible participants found there was no difference in the severity of anxiety or depression between the two groups. Demographic details of eligible participants compared to those of all HealthPoint patients from 2010 are listed in Table 1. The comparison showed an equal percentage of Hispanic participants and patients, and a larger number of uninsured participants in the study.
SD, standard deviation.
Integrative provider teams
Because patient care at HealthPoint is collaborative and varied in nature, an analysis of the care team composition was done. Patients at HealthPoint can be seen by any of the available healthcare service providers. This includes conventional providers (MD, DO, ARNP, and PA), behavioral health consultants (BH), naturopathic physicians (ND), acupuncture providers (LAc), and nutrition providers (RD). During the study period, all 60 participants saw a naturopathic physician, and 55% also saw a conventional provider. The same percentage (55%) also saw a behavioral health consultant. Twelve percent of the group utilized nutrition services, and 5% utilized acupuncture. Sixty-five percent of the group had their first clinical contact at HealthPoint with a naturopathic physician, and 25% of the group saw only the naturopathic physicians. See Figure 1 for a more detailed representation of care team composition.
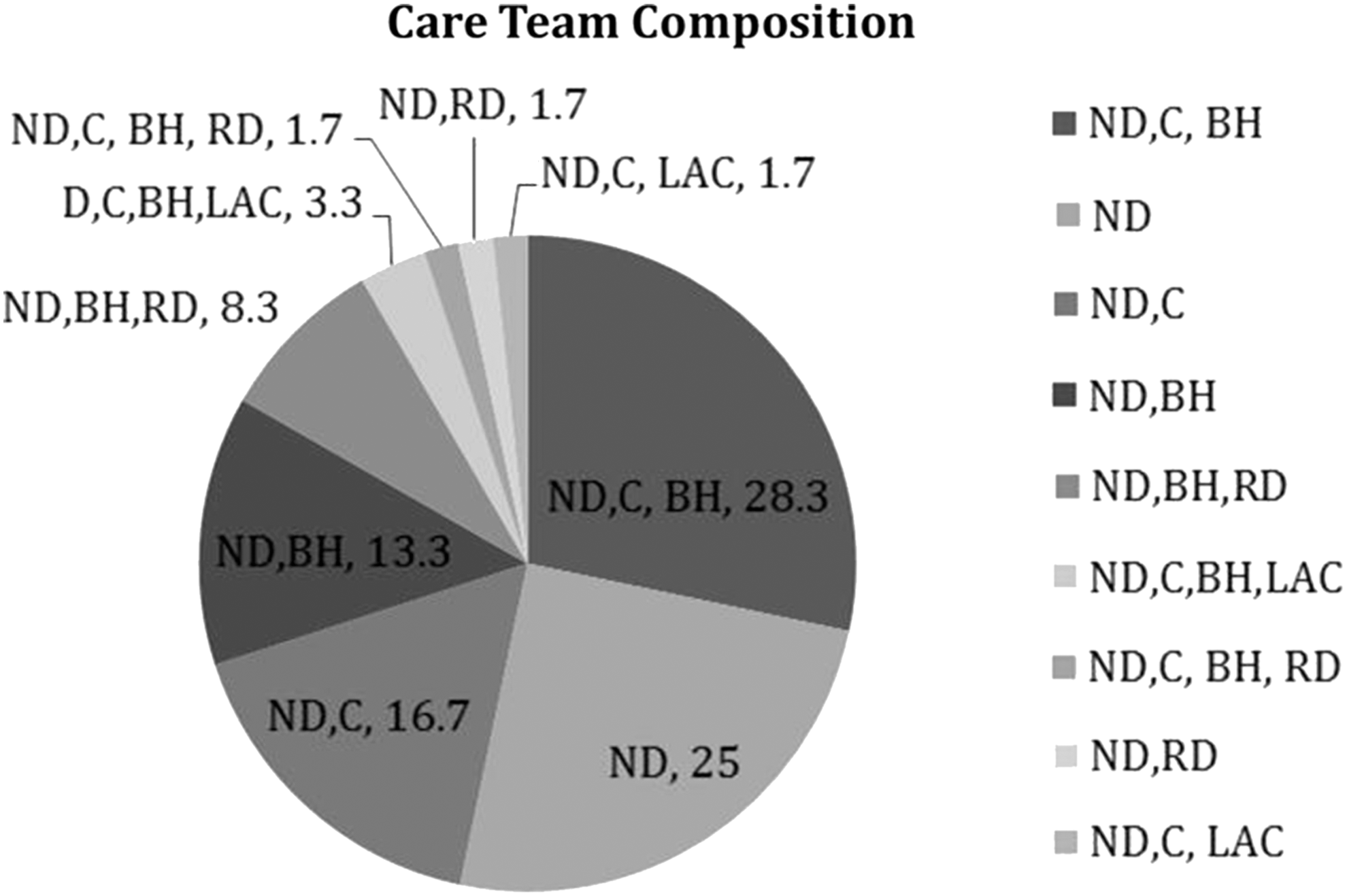
Provider type combinations that provided care to the participants during the study period. ND, naturopathic physicians, C, conventional providers (MD, DO, ARNP, and PA); BH, behavioral health consultants; LAc, acupuncture providers; RD, nutrition providers.
Modality utilization
Recommended treatment modalities were extracted from patients' medical records. The modalities used include nutraceuticals (vitamins, minerals, and nutritional supplements), pharmaceuticals, homeopathic medicine, herbal medicine, acupuncture, craniosacral therapy, and HeartMath biofeedback. As shown in Figure 2, the most common treatment modalities used were nutraceuticals (75%), followed by pharmaceuticals (32%), homeopathy (30%), herbals (25%), and acupuncture (20%). There was limited use of craniosacral and HeartMath biofeedback. See Table 2 for a detailed list of both the nutraceuticals and pharmaceuticals prescribed for anxiety and depression during the study period.

Percent of participants utilizing treatment modalities alone or in combination.
Clinical outcomes
The initial mean PHQ-9 score was 16.4, characteristic of patients experiencing moderate to severe levels of depression. The initial mean GAD-7 score was 12.4, characteristic of patients experiencing moderate levels of anxiety. The overall improvement in symptoms of depression and anxiety was highly significant (p < 0.0001) when comparing the group's average initial screener scores to their average final screener scores for both depression (16.4 vs. 8.6) and anxiety (12.4 vs. 7.2; see Table 3). The final PHQ-9 and GAD-7 scores in the outcomes group are clinically consistent with mild symptoms of depression and anxiety, and represent average drops in scores of 48% for depression and 42% for anxiety. The response rate as measured by a 50% decrease in scores for those with initial scores ≥10 were 58.6% for depression (PHQ-9) and 50% for anxiety (GAD-7), as can also be seen in Table 3.
PHQ-9, Patient Health Questionnaire; GAD-7, Generalized Anxiety Disorder 7-item scale.
Discussion
This study found that patients in a community health center setting who received care for depression and anxiety from a naturopathic physician (or a healthcare team including naturopathic physicians) demonstrated improved clinical outcomes based on decreased screener scores for depression (PHQ-9) and anxiety (GAD-7). A main goal of this study was to collect data on the usual care provided by HealthPoint naturopathic physicians while minimizing process change and, as much as possible, limiting the impact on health center flow—providing a strong proof of concept for future practice-based studies. Additionally, the study adds new data to the limited literature on the nature and effectiveness of naturopathic medicine to treat anxiety and depression in the context of an integrative community health center.
There was strong, statistically significant (p < 0.0001) improvement in both depression (PHQ-9) and anxiety (GAD-7) scores in patients receiving naturopathic care in this study. They had on average a 48% decrease from the initial to final screener score for depression and a 42% decrease from the initial to final screener score for anxiety. The percentage of participants who experienced a 50% decrease in screener scores was 58.6% for PHQ-9 and 50% for GAD-7. The response rates for depression seen in this study compare favorably to other published studies as can be seen in Table 4. In a psychiatric clinical practice, a 41–45% response rate to depression treatment (defined as a PHQ-9 score <10 or a 50% improvement in the PHQ-9 score) was documented. 31 In a community health center, a 35.1% response rate (defined as a 50% decrease in PHQ-9 score) to depression treatment was reported. 32 In a review of collaborative care management for depression in Minnesota, a 52.3% clinical response to depression treatment (defined as PHQ-9 score ≤50% of baseline) was reported. 33
Response rate to depression treatment defined as 50% improvement or PHQ-9 < 10.
NMQP-DA, Natural Medicine Quality Improvement Project for the Treatment of Depression and Anxiety.
Socioeconomic barriers faced by the low-income, uninsured, minority, and homeless people served by HealthPoint presented challenges to participation. It has been shown that homelessness, language barriers, poverty, and lack of social support adversely impact healthcare access and behaviors, and make it more challenging to identify, assess, and treat a health problem. People who are on a low income are more likely to suffer from social behavioral and environmental impediments to good health and well-being, and are thus more likely to suffer ill health and poor outcomes. 34 Almost half of the participants were at or below the poverty line. Furthermore, the group differences between those who became eligible participants and those who had only one visit are of interest. The eligible participants more often had their initial clinical contact with a naturopathic physician and were then more likely to follow up with them. In addition, the participants were more likely to be married, to be insured, and to have a higher socioeconomic status, and they were less racially diverse than the group with only one visit were. There was, however, no difference in initial screener scores between the eligible participants and those with only one visit for anxiety or depression.
One possible explanation for the significant improvement seen in screener scores is the time and attention to patients that naturopathic physicians provide at HealthPoint. Naturopathic visits at HealthPoint typically last 30 min, whereas other HealthPoint medical providers (M.D., D.O., A.R.N.P., or P.A.) typically have patient visits lasting 20 min. Good communication skills by physicians can affect patient outcomes, and time with patients may improve the chances for improved communication. 35 The extended length of naturopathic visits at HealthPoint may explain, in part, the improvements in depression and anxiety seen with naturopathic care. The treatment approach of naturopathic care is also likely at work here. Naturopathic philosophy views illness as a process beginning with a disturbance in health that may be caused by a number of factors (e.g., poor nutrition or stress). Naturopathic therapies are thus aimed at identifying and minimizing such disturbances with the least invasive and intensive therapies possible, ultimately restoring the overall health of mind and body. 20
The variety of treatment modalities used by naturopathic physicians at HealthPoint is common in naturopathic medical practice and includes the use of pharmaceuticals prescribed as part of the broad scope of naturopathic medical practice in Washington State. The choice of modality is a shared decision-making effort between provider and patient that may be influenced by evidence for safety and efficacy, patient preference, and cost to the patient, including what may be covered by insurance.
Limitations of this study include the lack of a control group for comparison and a relatively small sample size (and the resultant effects on statistical power). Furthermore, 46% of patients did not return to see a naturopathic physician after their initial visit and thus were not eligible for outcome analysis. Additionally, conducting the study in a community health center setting did not allow for randomization in the selection process and leaves open the possibility of selection bias. There also remains the chance that the results are in some part due to a regression to the mean.
Conclusion
This project was designed to assess the quality of care received by patients with depression and anxiety who were seen by naturopathic physicians in the community health center, HealthPoint, and found significantly improved screener scores over the study period. More research is needed to determine if these results can be duplicated. Naturopathic physicians are an integrated part of the healthcare team at HealthPoint. However, this innovative model is not currently widely utilized. Further exploration of the possible benefits of this model in community health center settings is warranted.
With the healthcare workforce shortage and the increased demand for care in the community health center setting, the need for innovative solutions to build adequate and effective healthcare teams is urgent. This project provides data that may inform policy makers and others to consider expanding healthcare teams to include naturopathic physicians. Further study is needed to evaluate the potential benefits and challenges of including naturopathic physicians in community health center settings. It is the authors' hope that this work will catalyze broad conversations about healthcare delivery, healthcare teams, and the opportunities available to improve care for patients.
Footnotes
Acknowledgments
We acknowledge the contributions and support of JoAnn Dechant, ND, and Christopher Krumm, ND, for data collection and clinical care of patients; Judy Featherstone, MD, CMO, and Thomas Trompeter, CEO, of HealthPoint for their general support for the project; and the participating health centers of HealthPoint.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.