
Abstract
Objectives:
Gastroesophageal reflux disease (GERD) is a prevalent gastrointestinal disease that causes troublesome symptoms and/or complications. The major therapeutic strategy for GERD focuses mainly on symptom alleviation using proton pump inhibitors (PPIs), which does not produce a perfect response in all patients. An approach with new therapeutic agents for GERD seems to be essential. The aim of this study was to review animal and human studies investigating the effect of medicinal plants in GERD as well as mechanisms underlying their therapeutic effects.
Methods:
Medline, Scopus, and Cochrane Central Register of Controlled Trials were searched for animal or human studies. The data collected covered January 1966–October 2015.
Results:
A total of 22 studies were included in this review, of which nine were animal studies and 13 were human studies. Ceratonia siliqua as a medicinal plant and rikkunshito as a multicomponent herbal preparation were the most frequently studied herbal medicines in GERD. Antioxidant and anti-inflammatory activities were the main mechanisms demonstrated in animal studies for ameliorating the effects of medicinal plants in GERD. Other mechanisms include downregulation of genes encoding inflammatory proteins, improvement of barrier function and gastric mucus, a decrease in gastric acid, and induction of tonic contractions of the lower esophageal sphincter. All herbal preparations used in human studies have led to the alleviation of symptoms related to GERD. Myrtus communis and Cydonia oblonga showed marked reduction in GERD symptoms comparable to omeprazole. The therapeutic effect of Cydonia oblonga persisted after discontinuation of the drug. Tongjlang and rikkunshito showed therapeutic effects for non-erosive reflux disease (NERD) where PPIs failed to show a promising effect. Studies on Ceratonia siliqua have been solely focused on regurgitation in infants, and a remarkable decrease in the number of regurgitations was demonstrated.
Conclusion:
The multiple mechanisms of action of medicinal plants in GERD other than anti-secretory properties appear to provide more efficient treatment and helped to manage the histopathological changes associated with this disorder. Further studies are needed to understand the effects of medicinal plants on GERD better.
Introduction
G
The main pathophysiology of GERD is reflux of the gastric contents, including gastric acid, followed by esophageal mucosal injury or acid stimulation of the esophageal mucosa, even without injury. 9,10 In recent years, the accelerated pace of life, increasing work pressure, and changes in diet have increased the incidence of GERD, 11 and this has a considerable negative impact on patient quality of life. 12 –15
A major therapeutic strategy for GERD is inhibition of acid secretion by using proton pump inhibitors (PPIs). 16 –18 However, in clinical practice, troublesome GERD symptoms persist in 20–30% of patients, despite daily treatment with a standard PPI dose. 19 Discovery of new pharmacological agents for GERD appears to be necessary. One invaluable source for the discovery of novel drugs is medicinal plants. The World Health Organization (WHO) reports that the use of herbal remedies worldwide exceeds that of conventional drugs by two- to threefold. 20,21
About 80% of people in developing countries continue to rely on traditional medicine based largely on species of plants for their primary healthcare. At present, about 25% of pharmaceutical prescriptions in the United States contain at least one plant-derived ingredient. 22 Gastrointestinal disease, including inflammatory bowel disease, irritable bowel syndrome, and peptic ulcer, are among the disorders that are frequently treated using medicinal plants. 23 –25 The present study is a review of animal and human studies investigating the effect of medicinal plants used for the management of GERD and the mechanisms underlying their therapeutic effects.
Methods
Medline, Scopus, and the Cochrane Central Register of control trials were searched for all animal or human studies that examined the effect of any herbal preparation on GERD, as well as investigating their possible mechanisms in this disease. With regard to human studies, any uncontrolled or controlled study that investigated the effects of any herbal preparation alone or compared to placebo or conventional therapies in any outcomes related to GERD was included. Unpublished works, non-English articles, and studies investigating complementary medicines rather than herbal medicines were excluded. Data were collected for the period January 1966–October 2015. The search terms were “gastroesophageal reflux” in the title and abstract and “plant,” “extract,” or “herb” in the body of the text.
The results of the primary search were screened by two independent investigators. The references of the retrieved articles were also evaluated for relevant studies. The articles were reviewed to extract plant, scientific names, complete ingredients of the product (in combined preparations), the part and extract of the plants, active components (if mentioned), model for animal investigations, and type for human studies. The results were abstracted in Tables 1 and 2.
GERD, gastroesophageal reflux disease; ↓, decrease; ↑, increase; MDA, Malondialdehyde; GSH, glutathione; SOD, superoxide dismutase; MPO, myeloperoxidase; GSSG, oxidized glutathione; MnSOD, manganese superodxide dismutase; GPX, gluatathione peroxidase; CAT, catalase; LES, lower esophageal sphincter; TBARS, thiobarbituric acid-reactive substance; TNF-α, tumor necrosis factor alpha; IL-1β, interleukin-1 beta; ICAM-1, intercellular adhesion molecule-1; CINC-2, cytokine-induced neutrophil chemoattractant-2; MCP-1, monocyte chemotactic protein-1.
RE, reflux esophagitis; NERD, non-erosive reflux disease; PPI, proton pump inhibitor, ↓, decrease in; ↑, increase in.
The quality of animal studies was determined according to Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines, 26 and this is represented in Table 3.
+, meet the mentioned criteria; −, doesn't meet the mentioned criteria; ARRIVE, Animal Research: Reporting of In Vivo Experiments.
In human studies, the study design, number of patients, intervention, duration of treatment, Jadad score, and the efficacy and tolerability of the herbal treatment were also recorded. The Jadad score rates the quality of the study based on its description of randomization, blinding, and dropouts (withdrawals), and was used to assess the methodological quality of trials. The quality scale ranged from 0 to 5 points. A score of ≤2 was considered low quality, and a score of ≥3 was considered high quality. The risk of bias for the human studies was determined according to Cochrane Collaboration's tool for assessing the risk of bias, and this is demonstrated in Table 4.
+, sign of bias; −, no sign of bias; ?, judgment unclear.
Findings and Results
The electronic search yielded 639 items (Fig. 1): 70 from Medline, 567 from Scopus, and two from Cochrane Central Register of control trials. Of these, 23 reports were excluded because they duplicated findings, 39 because they were opinions, and 473 on the basis of title and abstract. A total of 104 papers were retrieved, and 82 were excluded. Of these, 19 were excluded because they studied non-herbal drugs in combination with plants or other types of complementary medicine, 53 because they were about GERD but were non-interventional, one because it was not in English, and nine because the treatment exacerbated GERD. Of the 22 studies included in this review, nine were animal-based and the rest were human studies. Most animal studies met all criteria for quality assessment according to ARRIVE guidelines, except for validity (Table 3). From 13 human studies, seven obtained Jadad scores of ≥39,11,19,27–30 and six obtained a Jadad score of <331–36 (Table 2). In human studies, the most risk of bias was observed for uncontrolled studies (Table 4).
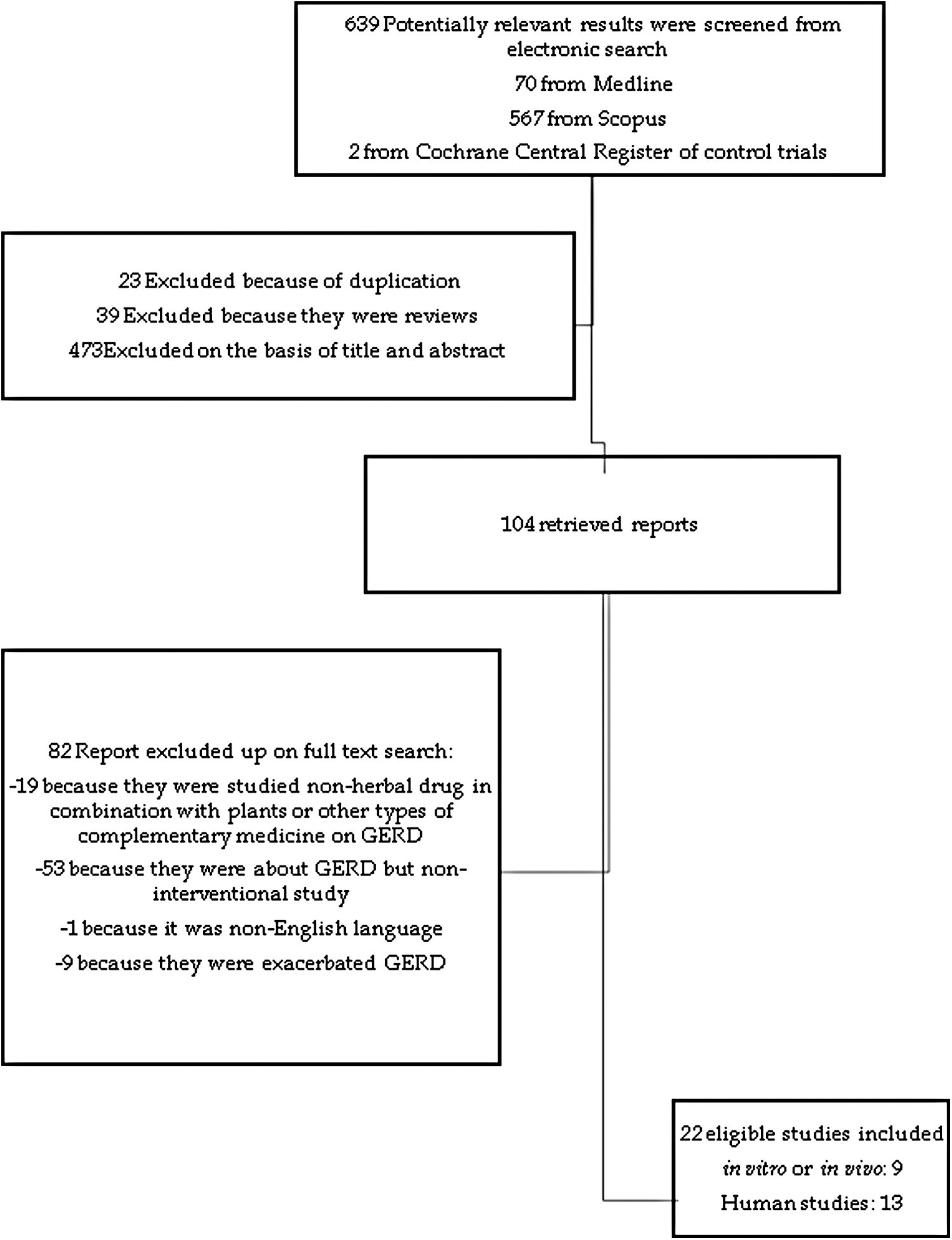
Flow diagram of study design.
Animal studies
Artemisia asiatica
Pretreatment with extract of Artemisia asiatica (DA-9601) decreased the overall thickness of the esophageal wall and extent of ulceration over the ranitidine group. Ranitidine failed to decrease the severity of reflux esophagitis (RE). Only DA-9601 pretreatment showed a statistically significant decrease in mean score for extent of mucosal ulceration and mucosal inflammation. The mean inflammation score of the DA-9601-treated groups was significantly lower than those of the ranitidine-pretreated group. Esophageal mucosa showed excellent regeneration in the DA-9601 pretreatment groups, whereas no or scant evidence of regeneration was observed using ranitidine. 37 The possible mechanisms of action of DA-9601 in attenuating RE are antioxidant and decrease in inflammatory factors, including NF-kB and COX-2, as well as a decrease in iNOS expression. 37,38 Ranitidine did not affect oxidative stress in the esophageal mucosa. 37
Curcuma longa
Curcumin is a compound isolated from the rhizome of Curcuma longa and plays a preventive role in the formation of acute acid RE. It was not effective in prevention of chronic acid RE. However, its combination with dimethyl sulfoxide as an antioxidant agent reduced the mortality rate and severity of the esophagitis ulcer index to approximately that of lansoprazole. Intraduodenal administration of curcumin also markedly prevented the formation of acute mixed RE and reduced neutrophil infiltration. By contrast, lansoprazole tended to increase the severity of all histopathological changes over the control and curcumin-treated groups. The antioxidant and anti-inflammatory activity of curcumin seemed to play a crucial role in its beneficial effects on GERD. 39
Lonicera japonica
Pretreatment of rats with Lonicera japonica flowers inhibited the induction of RE in rats and was probably mediated by antioxidant activity that was similar to alpha-tocopherol. 40
Morus alba
Treatment with Morus alba leaf extract in rats prior to induction of GERD increased the gastric wall mucus. The level of plasma histamine and H+-K+-ATPase decreased significantly. Morus alba extract demonstrated antioxidant activity by inhibition of lipid peroxidation and an increase in the level of antioxidant enzymes. 41
Panax quinquefolium
Pretreatment of rats with Panax quinquefolium significantly attenuated the severity of RE-induced tissue damage and caused a dose-dependent reduction in lipid peroxidation and increase in antioxidant status. By contrast, omeprazole, although effectively improving mucosal damage, failed to show antioxidant activity. Panax quinquefolium also significantly downregulated the genes encoding proteins that play a role in acute inflammation, including intercellular adhesion molecule 1 (ICAM-1) and cytokine-induced neutrophil chemoattractant 2 (CINC-2) expression. It showed no effect on monocyte chemotactic protein 1(MCP-1), a marker of chronic inflammation. 42
Rubus spp. (black raspberry)
Dietary supplementation of black raspberry did not alter the levels of cellular antioxidant or lipid peroxidation compared to the control diet in a short-term study of gastroesophageal reflux (GER) induction in an esophagoduodenal anastomosis animal model. Moreover, it did not alter or ameliorate the grade of esophagitis or the induction of Barrett's esophagus. 43
Salvia miltiorrhiza
Salvia miltiorrhiza appears beneficial for the management of GERD by inducing tonic contraction of the lower esophageal sphincter (LES) of rats. The extracellular Ca (2+) influx pathway was revealed to be an underlying mechanism of this contractile effect. 44
STW 5
STW 5 (Iberogast) is a multicomponent herbal medicine composed of hydroethanolic extracts of nine herbs and is prepared for functional gastrointestinal disorders, including GERD and irritable bowel syndrome. 24,45 STW 5 did not affect esophageal pH in an acute model of RE in rats, but dose dependently reduced the severity of esophageal lesions and normalized the deranged level of proinflammatory cytokines, including tumor necrosis factor alpha (TNF-α) and interleukin-1 beta (IL-1β). 46 It normalized changes in the level of oxidative stress markers for myeloperoxidase (MPO) and thiobarbituric acid-reactive substances (TBARS) 45 . It was also shown to improve gastric accommodation, 46,47 reduce visceral hypersensitivity, 48,49 and increase the tonic contractions of the LES, 50 all of which are factors that play an important role in the pathogenesis of GERD. 51
Human studies
Acidinol syrup
Administration of acidinol syrup, a polyherbal formulation, for 4 weeks to patients with chronic complaints of heartburn or acid regurgitation resulted in relief from the symptoms of general heartburn, abdominal pain, bloating, loss of appetite, nausea caused by heartburn, and dyspepsia in a significant percentage of patients. The ingredients are reported to act as PPIs and reduce gastric secretion in the stomach. 34
Ceratonia siliqua
The gum obtained from the seeds of Ceratonia siliqua is commonly known as locust bean or carob bean gum. Results of human trials showed that infant milk containing carob bean gum ameliorated the clinical symptoms of regurgitating infants, such as vomiting and weight loss, and significantly decreased the percentage of time with an esophageal pH of <4.0, but did not significantly alter gastric emptying time. 30,31
Another clinical trial revealed a significant effect for carob bean gum combined with milk on a decrease in the frequency 36 and amount of regurgitation by decreasing the number of nonacid (pH >4) GER episodes and the mean reflux height reached in the esophagus, but the frequency of acid GER did not decrease. 29 Another clinical trial demonstrated that milk containing carob bean gum may be clinically effective for infant GERD, it but can lead to occult episodes of GER of long duration, possibly increasing the risk for esophagitis or respiratory dysfunction. 35
Cydonia oblonga (quince)
Administration of a syrup derived from the fruit of Cydonia oblonga to children with GERD resulted in a significant decrease in symptoms compared with before treatment. However, compared to the control group, the decrease was not significant. Despite the use of omeprazole, quince syrup remained effective for 2 weeks after its discontinuation. 28
Myrtus communis
In a randomized controlled trial, administration of aqueous extract of Myrtus communis fruit significantly decreased reflux and dyspeptic scores. 27 The protective effect of different fruit extracts were shown for gastric ulcers in rats. Moreover, the extracts reduced gastric juice volume and total acidity. 52
Olea europea
Administration of olive oil for 2–6 months to postgastrectomy patients with severe symptomatic duodenogastroesophageal reflux who did not respond to conventional therapies resulted in the patients being symptom free or caused a significant improvement in symptoms. 32
Rikkunshito
Administration of rikkunshito, a traditional Japanese multiherbal medicine, combined with rabeprazole, to patients with GERD for 4 weeks significantly decreased the frequency of GERD symptoms. 9 Similar intervention in elderly PPI-refractory NERD patients with acid-related dysmotility symptoms caused significant improvement in GERD symptoms, particularly abdominal bloating, feeling of heaviness in the stomach, and feeling ill after meals. 19 The effects of rikkunshito have been also evaluated for children with GERD. The frequency of GERD symptoms decreased in these patients after 7 days of administration. Furthermore, the percentage time for which esophageal pH <4.0 was recorded and the mean duration of reflux decreased markedly. The number of acid reflux episodes per hour did not change significantly. 33
Possible mechanisms of the action for rikkunshito have been investigated in RE models in rats, and these indicate that rikkunshito did not reduce the average total area of erosive lesions in the esophageal mucosa. Rikkunshito significantly suppressed intercellular space dilation and significantly increased the level of NP-40-insoluble claudin 3, but had no affect at the mRNA level, suggesting that it promotes tight junction formation by facilitating translocation of proteins. 53 Moreover, rikkunshito ameliorated the symptoms of RE by improving the barrier function of esophageal mucosa 53 and gastric emptying. 19
Tongjlang granules
Administration of a multiherbal Chinese medicine, tongjlang granules, to patients with NERD for 4 weeks improved symptoms and their quality of life. No adverse event was found during the study. 11
Discussion
This study reviewed in vitro animal and clinical studies focusing on medicinal plants for the management of GERD. All the studies are summarized in Tables 1 and 2. The most frequently studied simple and compound herbal medicines were Ceratonia siliqua and rikkunshito, respectively. All herbal preparations used in human studies have led to the alleviation of symptoms related to GERD. In two human studies, one on Myrtus communis 27 and another on Cydonia oblonga, 28 the effect of herbal preparation was compared to a conventional drug, omeprazole. Both of these studies showed marked reduction in GERD symptoms comparable to that of omeprazole. However, in one of these studies investigating the effect of Cydonia oblonga, 28 the relapse rate in the Cydonia oblonga group was significantly lower than omeprazole 2 weeks after drug discontinuation.
Two human studies, one on tongjlang granules 11 and another on rikkunshito, 9,19 have examined the effect of herbal preparations on PPI-refractory NERD. Both of the mentioned preparations could alleviate symptoms of GERD in comparison to placebo and even PPI.
Studies on one of the medicinal plants, Ceratonia siliqua, have been solely focused on infant regurgitation, and its bean gum has been administered as an additive to cow's milk. All of these studies showed a remarkable decrease in regurgitation. Only in one study was the decrease in regurgitation not significant. However, a marked reduction was shown in the reflux index.
The major underlying mechanisms for the effect of medicinal plants on GERD are antioxidant and anti-inflammatory activity. The medicinal plants and herbal preparations that act by these mechanisms are Artemisia asiatica, Curcuma longa, Panax quinquefolium, Lonicera japonica, and STW 5. Other mechanisms include downregulation of the genes encoding proteins that play role in acute inflammation, including ICAM-1 and CINC-2 (Panax quinquefolium), improving the barrier function and gastric mucus (Morus alba, rikkunshito, Curcuma longa, STW 5), decreasing gastric acid (Curcuma longa, Morus alba, acidinol syrup, tongjlang granules), increasing of tonic contractions of the LES (Salvia miltiorrhiza, STW 5), and inhibiting the proinflammatory cytokines TNF-α and IL-1 β (STW 5).
The pathophysiology of GERD is multifactorial. 54 Oxidative stress, inflammation, and acid secretion are pathophysiologic factors that contribute to GERD. 37,41,55,56 Anti-secretory treatment alone has not been effective in attenuating inflammation or the degree of RE and thus does not promote complete healing. 37,57 For example, omeprazole is an anti-secretory drug that improves mucosal damage. However, it failed to attenuate RE-associated changes in oxidative stress and inflammatory parameters significantly. 42 Most medicinal plants investigated for GERD show anti-inflammatory and antioxidant activity rather than anti-secretory properties. One advantage of medicinal plants over conventional anti-secretory agents is their promising effect on NERD, an area for which PPIs do not show potential effect. Moreover, medicinal plants appear to have a longer-lasting therapeutic effect than conventional anti-secretory agents have. For example, Cydonia oblonga was still effective 2 weeks after discontinuation.
Some studies reported a meta-analysis of the efficacy of Chinese herbal compounds on GERD. A Chinese compound called vendan that contains Pinellia ternate rhizomes, Zingiber officinale rhizomes, fruit exocarp of Citrus grandis, Citrus aurantium flowers, Phyllostachys nigra stems, and Glycyrrhiza uralensis root was effective for bile reflux gastritis and GERD. It alleviated symptoms significantly, and the relapse rate was markedly lower than that of conventional therapies. 58 A meta-analysis on a compound medicine called si-ni-san (SNS) that combines Bupleurum falcatum root, Paeonia lactiflora root, Citrus aurantium flowers, and Glycyrrhiza uralensis root showed that it had a better effect on duodenogastric reflux and GERD than conventional therapies. 59
One limitation of this review was the insufficient number of studies on the effect on reflux of each plant investigated. The number of human studies was few, and their sample sizes were low. It is suggested to conduct further clinical studies with larger sample sizes on the efficacy and safety of medicinal plants for GERD. Symptom alleviation was investigated in most studies, but the underlying mechanisms were not considered. Thus, it would be beneficial to design studies to investigate the mechanisms of action of medicinal plants for GERD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.