
Abstract
Objectives:
To introduce research that presents scientific evidence regarding the effects of mantra and mindfulness meditation techniques and yoga on decreasing blood pressure (BP) in patients who have hypertension.
Methods:
A literature search was performed to identify all studies published between 1946 and 2014 from periodicals indexed in Ovid Medline, EMBASE, CINAHL, PsycINFO, KoreaMed, and NDSL by using the following keywords: “hypertension,” “blood pressure,” “psychotherapy,” “relaxation therapy,” “meditation,” “yoga,” and “mind-body therapy.” The Cochrane's Risk of Bias was applied to assess the internal validity of the randomized controlled trial studies. Thirteen studies were analyzed in this meta-analysis by using Review Manager 5.3.
Results:
Among 510 possible studies, 13 met the selection criteria. Seven examined meditation, and six examined yoga. The meta-analysis indicated that meditation and yoga appeared to decrease both systolic and diastolic BP, which were within similar baseline ranges, and the reduction was statistically significant; however, some results showed little difference. After an in-depth analysis of those results, BP range and patient age were revealed as the factors that affected the different results in some reports. In particular, meditation played a noticeable role in decreasing the BP of subjects older than 60 years of age, whereas yoga seemed to contribute to the decrease of subjects aged less than 60 years.
Conclusions:
While acknowledging the limitations of this research due to the differences in BP and the participants' ages, meditation and yoga are demonstrated to be effective alternatives to pharmacotherapy. Given that BP decreased with the use of meditation and yoga, and this effect varied in different age groups, scientifically measured outcomes indicate that these practices are safe alternatives in some cases.
Introduction
T
Comparing national hypertension rates among adults older than 30 years of age, differences emerge. Generally, the global average is 30%, but it is projected that by 2025, global prevalence will have increased to 60%. 6 The usual treatment regimen is for patients to take antihypertensive medication regularly for the rest of their lives. However, physicians indicate that their patients often suffer from psychological stress in addition to hypertension, including job-related stress. 7 –9 Stress, including the related tension, anger, and aggression, triggers physiological responses in the sympathetic nervous system, specifically the secretion of excess stress hormones, which increase BP. 10,11 Therefore, it is important for hypertensive patients to manage their stress levels, including the use of mandatory stress-reducing adjuvant therapy, to manage BP.
The relaxation response is a term coined by Herbert Benson in a book of the same name, in which he describes his research into the effects of meditation. 12 The relaxation response is a model that uses meditation to stabilize the sympathetic nervous system while activating the parasympathetic system, thus operating on both physiological and psychological levels. 12,13
Current popular types of stress management include meditation, breathing exercises, biofeedback, and progressive muscle relaxation. Research has reported that the use of the relaxation response for stress management has increased on the assumption that it can decrease BP by inhibiting the sympathetic nervous system's stress response. Variable factors such as age, BP, and lifestyle habits account for inconsistent results. 14 –17
Although there is no consensus among scholars regarding the definition of meditation, it is divided into five broad categories: mantra meditation, mindfulness meditation, yoga, Qi Gong, and Tai Chi. 18 Systematic reviews of the effects of meditation on BP reduction were conducted in 2004 for transcendental meditation, 16 in 2013 for yoga 19 and Tai Chi, 20 and in 2015 for Qi Gong, 21 but all were found to lack sufficient evidence for BP control due to methodological weaknesses. Rainforth's study using 17 randomized controlled trials (RCTs) in 2007 concluded that adequate evidence was lacking to support relaxation therapy as an effective method of reducing BP. 15 In 2008, Cochrane conducted 25 research studies in attempts to verify the effects of relaxation therapy as applied in hypertensive patients; in addition to progressive relaxation therapy, the studies included biofeedback, cognitive behavioral therapy, and yoga for stress management. 17 The Agency for Healthcare Research and Quality (AHRQ) also tested the effects of relaxation therapy twice, in 2007 22 and 2014. 18 In a 2007 review, a meta-analysis of patients with hypertension showed a significant reduction in BP, but the study was determined to be of a low quality. In 2014, it was concluded that there was no advantage of meditation programs over the specific therapies that they were compared with.
Currently, hypertension treatment based on compliance and medication has reached its realistic limits, especially compared with diabetes or kidney disease. For hypertension treatment not be restricted to medication alone, it is recommended that patients integrate various daily adjuvant therapies such as diet, exercise, meditation, and yoga into their healthcare regimens. 23,24 Although the effectiveness of stress management for hypertensive patients has not been thoroughly examined, public interest in meditation programs and yoga is increasing, and they are increasingly being used as methods of stress management. 25
Therefore, it is logical to apply proper methodologies to studies of meditation programs and yoga to determine their effectiveness in stress management in patients who have hypertension with systematic severity; studies on effectively reducing BP by using alternative means would be significant and meaningful on many levels.
The meditation reviewed in this study includes mantra and mindfulness techniques, as described in the report of the AHRQ. 18 Yoga not only includes meditation but also focuses on physical relaxation, 26 and these practices were examined separately. The primary goal of this study was to use systematic research to provide a scientific basis for the effectiveness of meditation and yoga in the management of hypertension based on RCT results.
Methods
This research was based on the Cochrane Handbook for Systematic Reviews of Interventions 27 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 28
Criteria for considering studies for this review
Types of studies
RCTs of a parallel design that had an intervention period of at least 8 weeks and allowed an intention-to-treat analysis were included. Intention to treat signified that participants were analyzed in the treatment groups to which they were assigned. The reason for selecting an intervention period of at least 8 weeks is that Kabat-Zinn recommends a period of at least 8 weeks before results are observed. 29
Types of participants
We targeted adult patients older than 18 years of age who were diagnosed with prehypertension, or stage 1 or stage 2 hypertension. However, among participants older than 60 years or in cases of uncertainty regarding hypertension, we selected only those with a systolic blood pressure (SBP) between 140 and 159 mmHg or a diastolic blood pressure (DBP) between 90 and 99 mmHg.
Types of interventions
This study focused on meditation and yoga as interventions. Yoga includes meditation but focuses on physical relaxation; meditation focuses on psychological and spiritual relaxation. 25 Meditation in this study indicates transcendental meditation and mindfulness techniques, and it was reviewed separately from yoga. There were no limits placed on control groups; participants received usual treatments or no active treatment and/or had social support or prior general health education.
Types of outcomes measured
This study aimed at revealing the differences across studies in average SBP and DBP measured before meditation or yoga therapy and at the end of the follow-up period. If the mean or standard deviation (SD) of BP was not reported, the difference between the pre-therapy baseline and the end of the study (change score) was used if its SD was available. If BP was measured in diverse postures or locations, we preferred clinic, ambulatory, and sitting measurements.
Database and search strategies
We searched seven computer-based electronic databases: MEDLINE, EMBASE, the Cochrane Library, CINAHL Complete, PsycINFO, KoreaMed, and the National Digital Science Library (NDSL). The search was performed on February 22, 2015. The search strategy was constructed and developed further within MEDLINE, and it was adjusted accordingly with these specific databases: “exp hypertension,” “blood pressure,” “exp meditation or meditation.tw,” “exp mind body therapy,” “(mind body and relaxation techniques).mp,” “exp breathing exercise or breathing exercise.tw,” “exp mindfulness or mindfulness.tw,” “exp music therapy or music therapy.tw,” and “psychotherapy.” To filter the studies for RCTs, search strategies developed by the Scottish Intercollegiate Guidelines Network were applied. 30
Study selection and data extraction
For references, we also searched through the published references of studies on pre-hypertension subjects. For adults aged 18 years and older who had stage 1 or stage 2 hypertension, this study reports the differences in average SBP and DBP from the beginning of the study to the end of the follow-up across studies. Findings were published in both Korean and English and had been peer reviewed. If the research participants had normal BP, stage 2 hypertension, pregnancy-induced hypertension, or secondary hypertension, the main intervention was other types of relaxation therapy; subjects who were not a part of the actual RCT were excluded. All duplicates among the initially retrieved articles were removed. Then, inclusion and exclusion criteria were applied by examining the title and abstract; the main text was examined if it was difficult to make an accurate judgment based only on the title and abstract. Data sampling was based on the evidence table, and data were used after their relevance was examined. Among the selected studies, we extracted place of study, methods of randomization and blinding, study inclusion criteria, gender ratios, average age, intervention, and average SBP and DBP from the beginning to the end of follow-up. Two authors independently reviewed the entire process and then made selections by discussion until consensus; any disagreements were resolved through third-party intervention.
Quality assessment
The methodological quality of included trials was independently assessed by two reviewers using Cochrane's Risk of Bias developed by the Cochrane Collaboration. It consists of criteria that assess seven areas: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. Each criterion was assessed by three risk levels of bias (high, low, and unclear) depending on the study description.
Statistical analysis
We conducted a meta-analysis of the articles selected by using Review Manager 5.3 (Cochrane Collaboration, London, United Kingdom); the reported results consisted of continuous data. The meta-analysis examined individual studies based on one-coin, number of subjects in the control group, averages, and SDs. With these numbers, we could also calculate weighted mean differences. Our meta-analysis of the summary estimates from a fixed-effects model suggested mean difference, SD, and 95% confidence interval (CI) by using general inverse estimation. Heterogeneity between studies was calculated by using Cochran's Q and Higgins' I2 statistics. I2 statistics categorize study variance attributable to heterogeneity as 0%–40% (might not be important), 30%–60% (moderate heterogeneity), 50%–90% (substantial heterogeneity), and 100% (considerable heterogeneity). 31 The existence of publication bias was demonstrated by using a funnel plot.
Results
Description of included studies
A total of 690 studies were initially found through electronic databases from Ovid Medline, EMBASE, Cochrane Library, CINAHL, PsycINFO, KoreaMed, and others. Among these articles, 180 studies were duplicates and were eliminated. According to inclusion and exclusion criteria, 475 studies were excluded based on information in the titles and abstracts. The full text articles of 35 studies were reviewed, and another 22 studies were excluded due to nonqualification of eligible criteria. In sum, 497 of 510 studies (97.5%) were eliminated; 13 studies were selected for the current meta-analysis. The detailed process of selection is outlined in the flow chart in Figure 1.
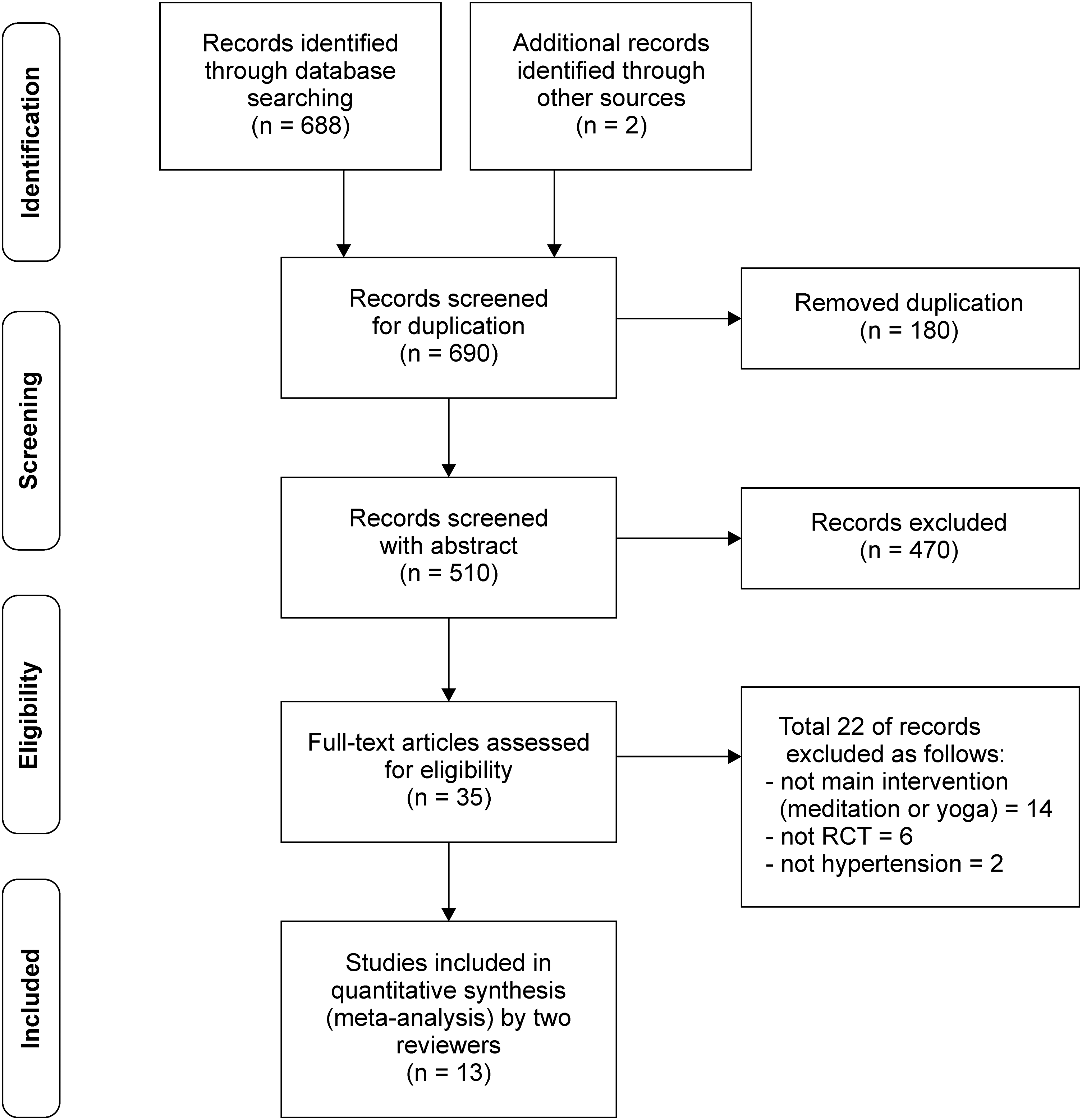
Flow diagram of article selection.
Methodological quality of included studies
All 13 studies 32 –44 were of a high quality and met the risk of the bias tool's seven criteria, including using concealment during random allocation. Only eight 32 –35,40,41,43,44 of the selected studies used blinded controlled trials; most studies evaluated participants' BP with an automatic BP machine, so the lack of double blinding might not have affected those results. However, two studies 38,42 were assessed to be of a low quality in four or five areas (Fig. 2).
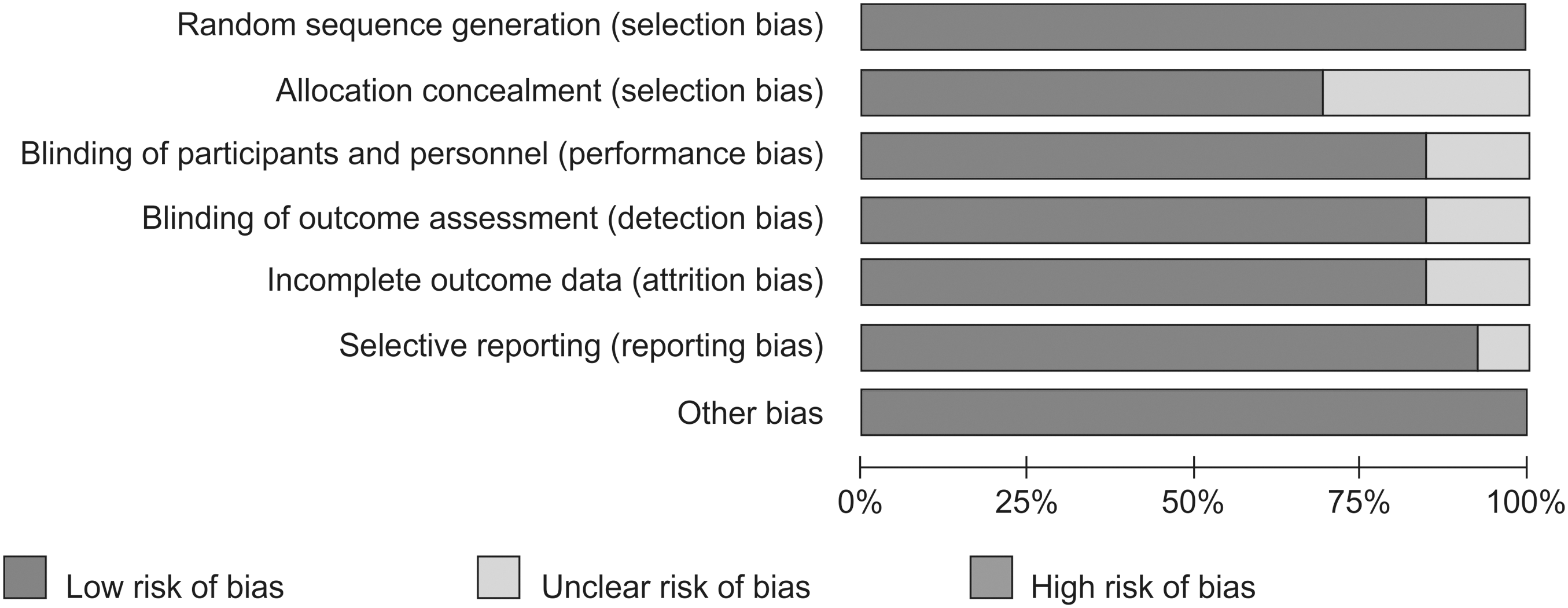
Risk of bias graph.
General characteristics of selected studies
The 13 studies investigated a total of 753 participants aged 18 years and older, and the assessments pertained to meditation and yoga as treatments for hypertension. More specifically, 7 studies 32,35,37,39,41,43,44 with 359 participants investigated meditation, and 6 studies 33,34,36,38,40,42 with 394 participants examined yoga. Among the selected studies, six (the majority 37,38,40,41,43,44 ) were from the United States, two each were from India 34,42 and Canada, 32,35 and one each was from Sweden and South Korea. Most studies had between 50 and 100 participants, three had more than 100, and three had fewer than 50. Most of the participants were patients with hypertension; one study 35 investigated prehypertensive participants, and five 32,34,36,38,43 targeted stage 1 hypertension. Hagins' study 33 targeted both pre- and stage 1 hypertension. Two studies 40,41 targeted both stage 1 and stage 2 hypertension, and in four studies 37,39,42,44 researchers were unable to conclusively identify unclassified hypertension. The studies were conducted by age bracket: Two 38,40 investigated participants in their 40s; five 32,33,35,39,41 studied people in their 50s; three 34,36,43 looked at patients in their 60s; and two 37,44 studied participants older than 70 years. Before the interventions, no participants had a baseline BP within the normal range, defined as an SBP <120 mmHg and a DBP <80 mmHg. Moreover, participants were either prehypertensive (SBP 120–139 mmHg, DBP 80–89 mmHg) or had stage 1 hypertension (SBP 140–159 mmHg, DBP 80–89 mmHg); only one study 42 examined stage 2 hypertension. Three studies 35,37,39 had an 8-week follow-up period after meditation or yoga; eight studies 32,34,36,38,41,43,44 had a 12-week follow-up period. Alexander et al. 44 only reported SBP results (Tables 1 and 2).
24-h ABP, 24-h ambulatory BP; BP, blood pressure; Con., control group; DBP, diastolic blood pressure; Exp., experimental group; F, female; M, male; MBSR, mindfulness-based stress reduction; SBP, systolic blood pressure.
p < 0.05; ** p < 0.01; *** p < 0.001.
CI, confidence interval.
BP response to meditation
In the seven meditation studies 32,35,37,39,41,43,44 with 359 participants, this meta-analysis found that both SBP (mean difference: −7.37 mmHg, 95% CI: −8.28 to −6.46, Z = 15.90, p < 0.001) and DBP (mean difference: −5.43 mmHg, 95% CI: −5.98 to −4.89, Z = 19.43, p < 0.001) systematically decreased after the introduction of meditation. However, some studies reported different results and concluded that meditation did not reduce either SBP (I2 = 90.0%, X 2 = 57.68, p < 0.001) or DBP (I2 = 92.0%, X 2 = 64.25, p < 0.001) (Fig. 3).
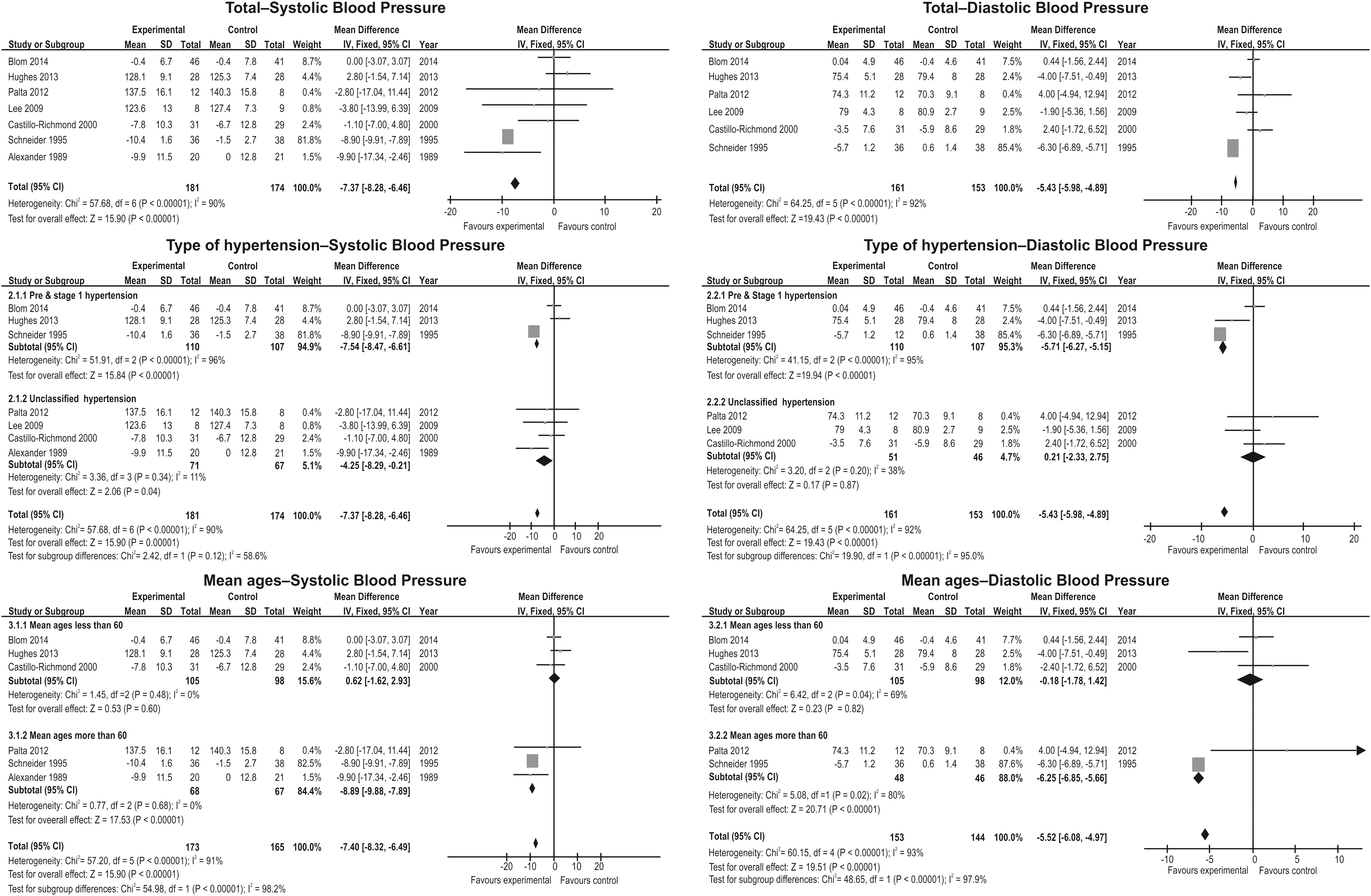
Blood pressure responses to meditation.
By group, meditation systematically decreased BP in pre- and stage 1 hypertensive patients (SBP mean difference: −7.54 mmHg, 95% CI: −8.47 to −6.61, Z = 15.84, p < 0.001; DBP mean difference: −5.71 mmHg, 95% CI: −6.27 to −5.15, Z = 19.94, p < 0.001). However, there were contradictions in studies that exceeded the 95% CI. With unclassified hypertension, only SBP (mean difference: −4.25 mmHg, 95% CI: −8.29 to −0.21; Z = 2.06, p = 0.040) showed a resulting decrease, whereas DBP (mean difference: 0.21 mmHg, 95% CI: −2.33 to 2.75, Z = 0.17, p = 0.870) showed no such effect. However, the heterogeneity between studies decreased to 40%.
In the detailed analysis of participants in their 60s, there was no significant decrease in either SBP (mean difference: 0.62 mmHg, 95% CI: −1.69 to 2.93, Z = 0.53, p = 0.600) or DBP (mean difference: −0.18 mmHg, 95% CI: −1.78 to 1.42, Z = 0.23, p = 0.820). However, in subjects aged 70 years and older, there were marked reductions in both SBP (mean difference: 0.62 mmHg, 95% CI: −1.69 to 2.93, Z = 0.53, p = 0.600) and DBP (mean difference: −6.25 mmHg, 95% CI: −6.85 to −5.66, Z = 20.71, p < 0.001). In addition, heterogeneity among studies was 0.0% in terms of SBP in subjects aged 70 years and older, indicating no difference in the results for this age group.
BP response to yoga
The results for the meta-analysis of six studies 33,34,36,38,40,42 showed that yoga can systematically decrease both SBP (mean difference: −4.59 mmHg, 95% CI: −5.54 to −3.64, Z = 9.48, p < 0.001) and DBP (mean difference: −3.65 mmHg, 95% CI: −4.26 to −3.03, Z = 11.56, p < 0.001). However, there was heterogeneity between studies in terms of both (SBP: I2 = 90.0%, X 2 = 52.42, p < 0.001; DBP: I2 = 83.0%, X 2 = 29.91, p < 0.001) (Fig. 4).

Blood pressure responses to yoga.
In the detailed analysis by type of hypertension, for both pre- and stage 1 hypertension, both SBP (mean difference: −9.44 mmHg, 95% CI: −12.17 to −6.72, Z = 6.79, p < 0.001) and DBP (mean difference: −2.38 mmHg, 95% CI: −4.07 to −0.69, Z = 2.76, p = 0.006) decreased. There was also less heterogeneity between studies in terms of SBP (I2 = 69.0%, X 2 = 9.64, p = 0.020) and DBP (I2 = 0.0%, X 2 = 1.92, p = 0.590). With unclassified hypertension, both SBP (mean difference: −3.92 mmHg, 95% CI: −4.93 to −2.91, Z = 7.59, p < 0.001) and DBP (mean difference: −3.84 mmHg, 95% CI: −4.50 to −3.18, Z = 11.33, p < 0.001) decreased systematically and significantly. There was 90% heterogeneity in these studies.
In the detailed analysis of research participants below the age of 60 years, both SBP (mean difference: −3.61 mmHg, 95% CI: −4.61 to −2.61, Z = 7.08, p < 0.001) and DBP (mean difference: −3.65 mmHg, 95% CI: −4.30 to −2.99, Z = 10.95, p < 0.001) showed significant decreases. No heterogeneity between studies was found in terms of SBP (I2 = 0.0%, X 2 = 0.20, p = 0.910) or DBP (I2 = 0.0%, X 2 = 0.66, p = 0.720). In patients aged 70 years and older, both SBP (mean difference: −11.40 mmHg, 95% CI: −14.57 to −8.22, Z = 7.03, p < 0.001) and DBP (mean difference: −2.37 mmHg, 95% CI: −4.35 to −0.38, Z = 2.34, p = 0.020) decreased significantly. Heterogeneity between studies was as follows: SBP I2 = 75.0%, X 2 = 3.95, p = 0.050; DBP I2 = 46.0%, X 2 = 1.85, p = 0.170.
Publication bias
Although there was no obvious asymmetry in either the meditation or the yoga results, there was publication bias in terms of how articles were distributed. In addition, there was no statistical verification in the funnel plot (Fig. 5).
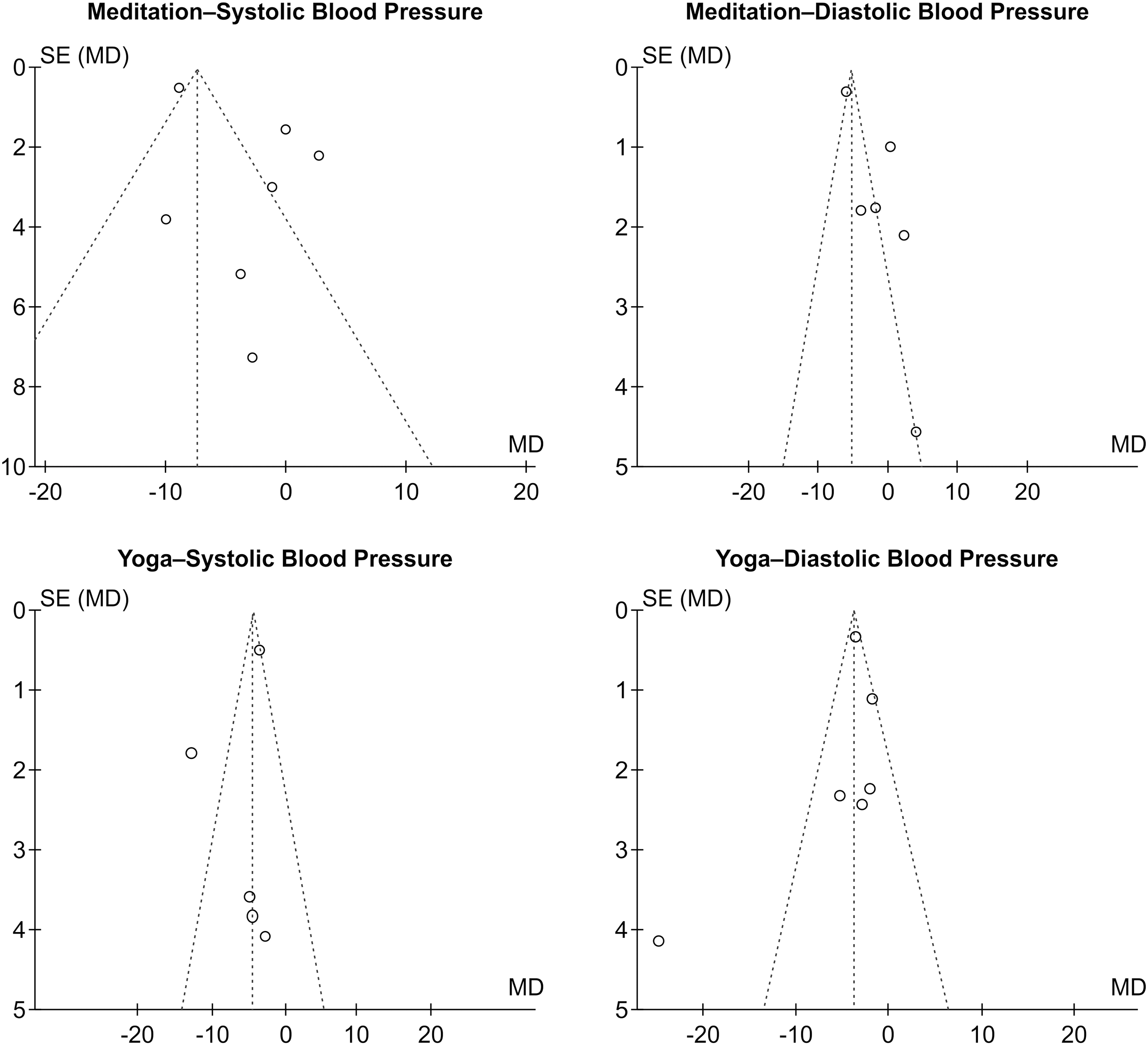
Funnel plots.
Discussion
This study was a systematic review and meta-analysis of 13 RCTs regarding the effect of meditation and yoga in the management of hypertension. The findings provide scientific evidence for the efficacy of meditation and yoga in hypertensive adults. The meta-analysis indicated that meditation and yoga appeared to decrease both systolic and diastolic BP statistically within a similar range.
Notably, some studies 16 included target subjects within the normal range of BP, one used a juvenile target group, 46 and another included non-RCT results. 19 Due to these nontypical factors, it remains difficult to independently verify the effects of relaxation therapy for hypertension. Therefore, this research sought to recognize the potential influence of meditation and yoga on decreasing BP among typical hypertension patients. To demonstrate the effect, this research applied systematic integration and studied 13 RCT results, and the interventions were analyzed by age and type of hypertension. With systematic review and integration, this study also attempted to suggest concrete evidence using meta-analysis.
The 13 selected studies revealed that meditation and yoga have been researched more actively in the United States and Canada than in Asia. However, meditation and yoga may have been increasingly used globally as alternative medicines for hypertension. In addition, the research participants in this meta-analysis using a fixed-effects model were mostly between the ages of 40 and 60 years, an age range with a high prevalence of hypertension. As such, this group was suitable for this research in terms of producing results that can augment clinical nursing practices for the population that is the most likely to be afflicted with hypertension.
The research participants had a systolic BP below 159 mmHg and a diastolic BP below 99 mmHg. Their basal BP was classified as stage 1 hypertension. All subjects used the same meditation and yoga practices as their interventions. The reasons for using the fixed-effects model are as follows. One, we considered the lack of integrated studies of hypertension related to meditation and yoga, and two, there was a possibility of publication bias. We decided to apply the fixed-effects rather than the random-effects model to avoid this bias. 47,48 We found no heterogeneity between studies in the actual analysis. In particular, meditation research showed a systematically significant difference in the summary estimates from the fixed-effects and random-effects models, indicating publication bias.
The meta-analysis incorporated a total of seven studies on the use of meditation to treat hypertension, and the result presented evidence that meditation can have a systemically significant effect in decreasing both systolic (mean difference: −7.37 mmHg) and diastolic (mean difference: −5.43 mmHg) BP. Although the findings were not consistent with regard to CIs and heterogeneity was high (more than 90%), the results did indicate that the CIs for reduced BP were clinically similar. When we conducted a detailed analysis to determine the causes for the heterogeneity observed between studies, we divided the research participants by age and stage of hypertension, and the heterogeneity between studies decreased significantly. In particular, in the detailed analysis of participants in their 60s, heterogeneity in SBP was absent, and it decreased for DBP as well. Meanwhile, the forest plot reflects that meditation had the effect of reducing BP, as indicated by consistent results in terms of similar directions of the effects, similar effect sizes, and similar differences in efficacy. The results showed that meditation among participants in their 70s and older had the widest range of effects on BP reduction (SBP: −8.89 mmHg; DBP: −6.25 mmHg).
The effect of yoga for reducing BP was integrated by six studies. Although the conclusions for yoga indicated lower effectiveness compared with meditation in reducing BP (SBP: −4.59 mmHg; DBP: −3.65 mmHg), the results did confirm an effect on BP reduction that was similar to that found with meditation. Moreover, as shown in the forest plot (Fig. 4A), there was a consistent trend of CIs in the respective studies, and this result applied to both SBP and DBP. In a subgroup analysis to identify the heterogeneity among studies, it could be concluded that the reduction in BP after yoga was consistent with and similar to the studies' estimated results. That is, yoga can reduce BP, and these results showed stability without heterogeneity, especially in participants below the age of 60. Yoga was associated with a less significant decrease than was meditation, particularly regarding SBP in subjects older than 60 years of age.
Finally, subgroup analysis revealed that different ages and BP levels of subjects are the cause of heterogeneity among studies. High heterogeneity among studies and publication bias are the limitations of this study.
Conclusions
Globally, pharmaceutical treatments and many types of therapy have been developed to treat hypertension. Despite their availability, hypertension prevalence remains high and control rates remain low. Thus, prevention and control of hypertension are still priorities; effective resources to achieve these goals benefit individuals, improve healthcare, and promote national health. The results of our systematic review of the literature based on 13 RCTs suggest that meditation and yoga can effectively reduce BP. Despite the limitations of this analysis, meditation and yoga were shown to be scientifically effective alternative therapies for decreasing BP. Therefore, we look forward to continued studies that support the application of meditation and yoga for hypertension treatment in clinical practice.
Footnotes
Acknowledgment
This work was supported by the Soonchunhyang University Research Fund.
Author Disclosure Statement
No competing financial interests exist.