
Abstract
Objectives:
The aim of this study was to investigate the effects of t'ai chi on blood serotonin levels, nicotine dependence, depression, and anger in hospitalized alcohol-dependent patients.
Method:
This study followed an experimental and nonequivalent control group in a non-synchronized design. It was performed in a hospital located in Young Ju city, Korea, from April to August 2013. Thirty-eight patients who were hospitalized with alcohol dependence were included. They were randomly divided into an experimental and a control group, with 19 patients in each group. Patients in the experimental group practiced the 24-posture yang style t'ai chi for 50 min three times per week for 8 weeks as part of the routine hospital rehabilitation program, and those in the control group followed only the routine hospital rehabilitation program. The effect of treatment was measured using blood serotonin levels and a questionnaire on nicotine dependence, depression, and anger. Both measurements were performed before and after 8 weeks of intervention. Data were analyzed using the t-test, chi-square test, and paired t-tests.
Results:
The experimental group showed a significantly increased blood serotonin level (p = 0.001) and significantly reduced nicotine dependence, depression, and anger (p = 0.001) than the control group did after 8 weeks of treatment.
Conclusions:
T'ai chi was shown to be an effective nursing intervention in hospitalized alcohol-dependent patients.
Introduction
A
Alcohol dependence shows a genetic vulnerability associated with suicidal behavior, impulses, and violence; the neurotransmitter that affects impulses and aggression is serotonin. 3 Serotonin regulates various complex behavioral patterns including emotions, appetite, sleep, and pain perception. It plays an important role in mental illnesses, such as schizophrenia and alcohol dependence, and is closely associated with depression. 4,5 Because nicotine and alcohol activate the dopamine system, the use of either substance can increase cravings for the other, 6 and alcohol-dependent patients with severe nicotine dependence experience stronger alcohol cravings. 7 Further, alcohol-dependent patients show twice as many depressive symptoms than those without alcohol dependence do, 8 and these patients are characterized by a defensive psychological state such as anxiety, anger, or personal phobia. 9 Anger is closely associated with other psychological variables such as depression and anxiety. 10 In addition, such problems associated with drinking have various negative effects on alcohol-dependent patients. Despite the great strides made in the treatment of alcoholism, patient denial is common, 9 resulting in a poor quality of life. 11 Accordingly, there remains a pressing need to identify additional effective, conservative treatment for alcohol dependency that will improve patients’ physical and psychological aspects and their overall well-being.
Treatments for alcohol dependence that have shown strong evidence of efficacy include short-term intervention, motivational approach, cognitive–behavioral approach, community-strengthening approach, behavioral self-control training, social skills training, and drug treatment. 12 Exercise therapy, referring to activities or behaviors directed toward physical and mental dynamics, is a non-drug treatment with few side effects, and has been used as an important means of enhancing mental health. 13
One of the characteristics of alcoholism is the high relapse rate, 14 the main cause of which is alcohol cravings. 15 Exercise has a positive effect on alcohol cravings and psychological problems, and it changes the secretion of physiological factors such as serotonin. 16,17 Despite the therapeutic effects of exercise therapy, it is not actively utilized in practice. 18 Few studies have applied t'ai chi to treat alcohol-dependent patients.
Although alcohol dependency causes severe somatic and psychological sequelae, the majority of affected patients are not motivated to seek treatment. In addition, the rate of forced admissions to a psychiatric healthcare facility is >70% in Korea. 19 The present study was designed to assess stages of change in patients with alcohol dependency and to screen their motivations using Prochaska's transtheoretical model of change that could minimize resistance and maximize the likelihood of successful change. Behavioral science research should provide a systematic approach to increasing the effectiveness of physical activity interventions. 20 The transtheoretical model is one of the leading integrative approaches and speaks of the necessity to match interventions to cognitive–behavioral stages in order to induce positive behavior change. 21 –23 The cumulative evidence (smoking, diet behavior, weight loss, low-fat diet, decreased use of alcohol, increase in exercise) indicates that the treatment intervention to the stage of change can enhance the outcome based on the percentage of patients completing therapy and those achieving ultimate success. 22,24
T'ai chi does not require special equipment, clothing, or location and is unaffected by the weather. Training as a group can also reduce the dropout rate. 25 The present study proposed a treatment alternative for alcohol-dependent patients that increases physical activity in a safe way and has a positive treatment effect on alcohol dependence.
It was hypothesized that the group of hospitalized alcohol-dependent patients who practiced t'ai chi would show an increase in serotonin blood levels and a reduction in nicotine dependence, depression, and anger compared with the control group after 8 weeks of treatment.
Materials and Methods
This was a quasi-experimental non-synchronized study with a nonequivalent control group, with all participants receiving 50 min of t'ai chi intervention three times a week for 8 weeks. The Institutional Review Boards of the Catholic University (MC13EASE0004) and Sam-Bong Psychiatric Hospital reviewed and approved the study.
Participants
Primary eligibility requirements included (1) written confirmation of alcohol dependence provided by the participant's physician based on the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders 4th Edition published by the American Psychiatric Association 26 ; (2) receiving inpatient treatment for alcohol dependence following alcohol detoxification in the hospital; (3) volunteered to participate; (4) a smoker; (5) in the contemplation or preparation stage of the transtheoretical model. Exclusion criteria included (1) not meeting the study requirements due to a scheduled short hospitalization period; (2) determined to be unfit to participate by the participant's physician; (3) prescribed medication determined capable of changing the blood serotonin level; (4) diagnosed with a major psychiatric disorder other than a depressive disorder such as schizophrenia and bipolar disorder, organic mental disorder, intellectual disability, or substance abuse other than caffeine and nicotine; or (5) in the precontemplation, action, and maintenance of the transtheoretical model. 22 Participants missing three or more t'ai chi interventions could be withdrawn from the study at the discretion of the principal investigator.
Participants with alcohol dependence at Sam-Bong Psychiatric Hospital were recruited via posters displayed on the ward and in other common areas of the hospital. They provided basic information about the study and invited patients to enroll. The first 50 eligible participants who volunteered were enrolled onto the study. To minimize coercion, each participant meeting all the inclusion criteria gave written informed consent. This included information assuring them that that they could quit at any time and would be at no disadvantage if they did so. Based on a previous study 13 and G*Power 3.1.5, each group required 19 patients for the t-test with an effect size of 0.94, significance level of 0.05, and statistical power of 0.80. The flow chart of subject recruitment through to completion is shown in Figure 1.
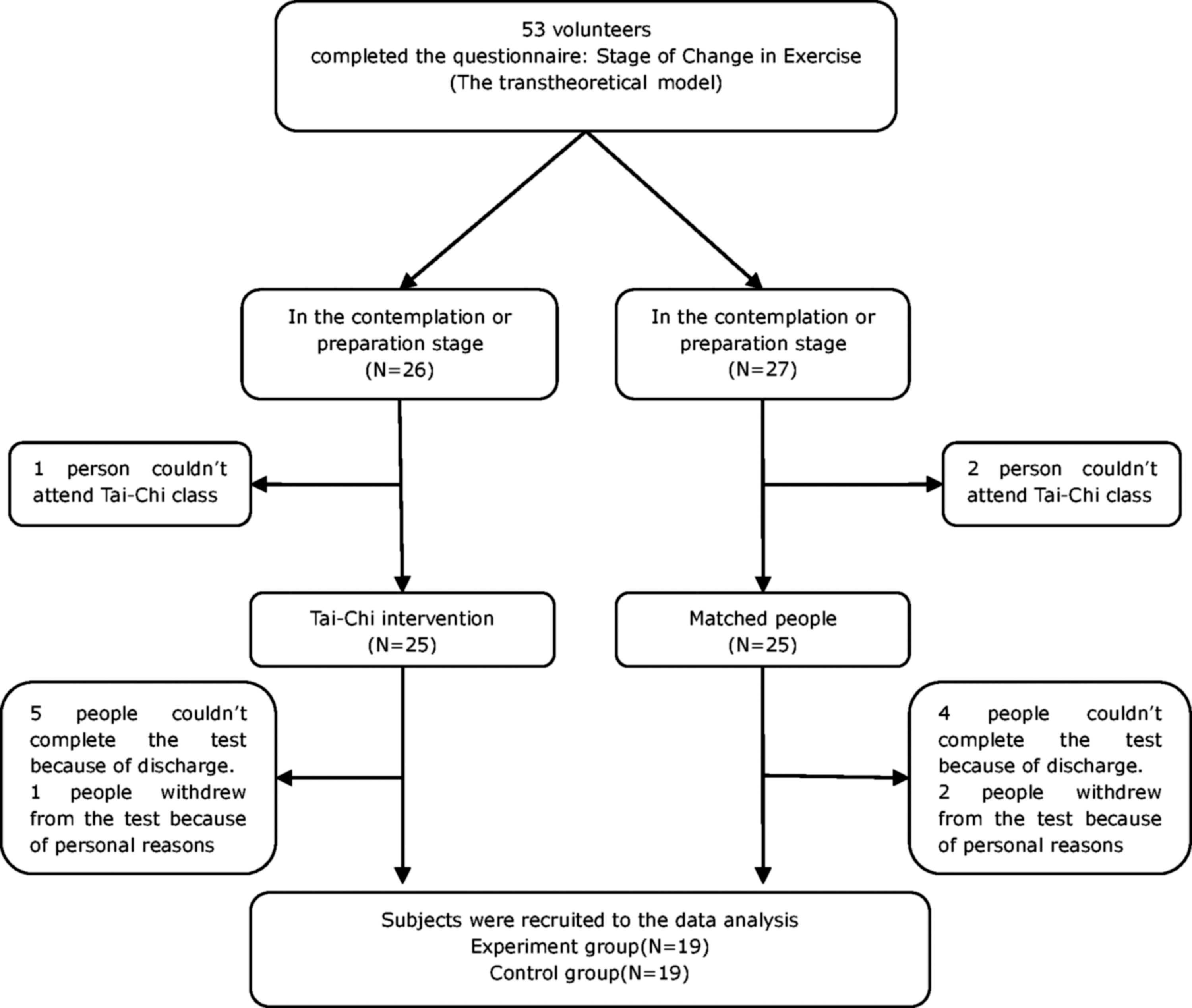
Flowchart of participant recruitment.
Experimental treatment
The experimental treatment used was the 24-posture yang style t'ai chi. T'ai chi has many types and different postures, but the principle is the same. Studies previously conducted in Korea primarily included the 12-posture sun style t'ai chi for patients with arthritis introduced by Dr. Paul Lam in 1997. In contrast, the 24-posture yang style t'ai chi is the most common form of t'ai chi and has been generalized to develop martial arts. It was also used to promote health by the Chinese government in 1955, and comprising 24 postures representative of t'ai chi from 128 postures. 25 In this study, the 24-posture yang style was used because alcohol-dependent patients have markedly reduced physical ability due to depression and alcohol dependence, despite having no limitations in physical function (Table 1).
RPE, Rated Perceived Exertion.
The exercise program comprised three 50 min sessions per week for 8 weeks based on the guidelines for adequate intervention from the Life Options Rehabilitation Advisory Council being 20–60 min three to five times a week for about 8–12 weeks. 27 T'ai chi is an aerobic exercise of low to moderate intensity, 25 conducted between 11 (fairly light) and 13 (somewhat hard) on Borg's scale of Rated Perceived Exertion. 27 –29 Patients learned the postures of the main exercise under the investigator's instruction during weeks 1–8 and repeated the main exercise of the previous week during every week of training in the multipurpose room. The content validity of the exercise was verified by a psychiatrist, a professor with t'ai chi–related research experience, and two exercise prescribers identifying intensity of 24 posture yang style t'ai chi. The format of each session was as follows: (1) warm-up—patients performed a 5 min warm-up, stretching the neck, hands, arms, chest, flanks, legs, and calf, raising and turning the shoulders, and pulling the legs; (2) main exercise—patients practiced the 24-posture yang style t'ai chi. 30,31 ; (3) wrap-up—each session concluded with 5 min of meditation and deep breathing.
Measures
Stage of change in exercise
The transtheoretical model proposed by Prochaska and DiClemente suggests that change occurs in five stages, which can be assessed using a questionaire. 32 The transtheoretical model regards the process as progression through the following five stages of change: precontemplation (those having no intention of beginning a regular exercise within 6 months; i.e., not ready); contemplation (those having such an intention; i.e., getting ready); preparation (those seriously considering regular exercise within 30 days; i.e., ready); action (those currently exercising); and maintenance (those currently exercising and maintaining an exercise).
Blood serotonin level
To measure the blood serotonin level, 5 cc of blood was drawn from each patient in the morning (at 10:00am). The samples were placed in an ethylenediaminetetraacetic acid (EDTA) sample container and shaken to prevent coagulation. The sample was centrifuged for 20 min at 900 g. using a centrifuge at the hospital, and the supernatant was separated. The samples were then sent immediately to the NEODIN Medical Institute for testing, and the test results were used as the study results.
Nicotine dependence
The Korean version of the Fagerstrom Tolerance Questionnaire was used to measure nicotine dependence. This measure was adapted and verified for reliability and validity by Ahn et al. 33 Reliability (Cronbach's α) was 0.69 in the study by Ahn et al. and 0.64 in the present study. In the present study, questions on nicotine content and the degree of inhalation were excluded. Among the six items used, four had two sublevel items each, and the score for individual items ranged from 0 to 1 point. The other two items had four sublevel items each, and the score for individual items ranged from 0 to 3 points. The total score of these six items had a range of 0–10 points. Higher scores indicated a higher severity of nicotine dependence.
Depression
A Korean version of the Beck Depression Inventory (BDI)-II was used to measure depression. The reliability of the measure (Cronbach's α) was 0.80 in study by Kim et al. 34 and 0.92 in the present study. The measure comprised 21 items, each with a four-point (0–3) rating scale. The total score had a range of 0–63 points, and higher scores indicated a higher severity of depression.
Anger
The State–Trait Anger Expression Inventory-Korean version (STAXI-K) was used to measure anger. The reliability of the measure (Cronbach's α) was 0.81 in the study by Jeon et al. 35 and 0.86 in the present study. In the present study, only the trait anger subscale (10 items) of STAXI-K was used. Individual items were scored using the four-point (1–4) Likert rating scale, with a total score range of 10–40 points. Higher scores indicated a higher severity of anger.
Data-collection procedure
The content and methods were approved by the ethics committee of the Institutional Review Board of the Catholic University (MC13EASE0004). The sampling method used was convenience sampling. Patients were randomly assigned to the experimental and control groups using a random number table.
Only patients motivated to change based on their stages of change in an exercise using the questionnaire concerning the transtheoretical model 32 were included. Only patients in the contemplation and preparation stages were included because of the ethical issue of forced exercise for those in the precontemplation stage and the difficulty of obtaining results from those in the action and maintenance stages, as they were likely to be discharged from hospital during the experiment. The average duration of stay for alcohol-dependent patients was approximately 70–90 days. After collecting the 8-week data from the control group, data were collected from the experimental group before and after 8 weeks of t'ai chi intervention in order to prevent the effect of experiment spreading from the ward. After data collection from the experimental group was complete, t'ai chi was offered to any member of the control group who wished to learn. Ten participants from the control group reached the end of the t'ai chi program. The remaining participants gave up due to being discharged, withdrawal, and so on.
Data analysis method
Paired-sample t-tests were used to examine the effects of treatment on change outcomes at baseline and immediately after intervention. The homogeneity of the experimental and control groups was tested using the chi-square and t-tests. In all analyses, statistical significance is reported using a two-tailed alpha level of ≤0.05, and 95% confidence intervals are provided for all parameter estimates. All analyses were carried out by using PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL).
Results
Patient characteristics
The two groups showed no significant differences in age, number of hospitalizations, age at early onset of drinking, marital status, level of education, income, or stage of change in exercise, indicating homogeneity between the groups (Table 2).
Exp, experimental group; Cont, control group.
Experimental effects
Blood serotonin levels
Blood serotonin levels increased for the experimental group but decreased for the control group. The data reveal a significant difference between the groups in terms of the change in blood serotonin level during the experiment (p = 0.001; Table 3).
Paired t-test; b t-test.
Nicotine dependence
The data show a significant difference between the groups with regard to the change in nicotine dependence during the experiment (p = 0.001; Table 3).
Depression
Depression decreased for the experimental group but increased for the control group. The data show a significant difference between the groups in terms of the change in depression (p = 0.001; Table 3).
Anger
The data show a significant difference between the groups in terms of the change in anger during the experiment (p = 0.001; Table 3).
Discussion
Results from this study showed that the 8-week program of t'ai chi significantly increased blood serotonin levels in the experimental group while levels decreased in the control group. Human repetitive movement exercises, such as cycling and jogging, increase the activity level of the serotonin system. 17 Previous research has reported that one kind of serotonin transporter (SERT) increased vulnerability to depression from stress. However, the research could not confirm whether people low on SERT were more depressive. 17 Although several studies concerning alcohol with SERT are reported, the findings are controversial. 36,37 Otherwise, genetic vulnerability causing individual differences is influenced by daily living and circumstance. 17 In this study, daily living and circumstances (except for t'ai chi exercise) are controlled. The results of the present study are consistent with those of previous studies, suggesting that regular t'ai chi practice increases the blood serotonin level by increasing the activity of the serotonin system. Moreover, after 8 weeks of t'ai chi, nicotine dependence for the experimental group significantly decreased. Previous studies have found that when alcohol-dependent patients are provided with a stimulus associated with cigarettes, alcohol cravings increase. 38 Brain images demonstrating alcohol and nicotine use increase the activity of the mesolimbic dopamine system. 39 In contrast, it has been argued that serotonin can improve nicotine addiction by serving as a “break” that regulates and controls the reward and punishment urges of the dopamine system and that serotonin activator reduces the number of self-administrations of nicotine in mice. 17 The results of the present study are consistent with those of previous studies, and suggest that the base level of serotonin reduces urges for nicotine in the experimental group.
The results of the present study show that 8 weeks of t'ai chi significantly reduced depression and anger in the experimental group, and increased depression in the control group. T'ai chi is a non-drug treatment that is effective for chronic schizophrenic patients, 18 as well as in reducing general psychopathology 18 and improving depression and stress. 13 It reduces anxiety, psychiatric symptoms, and depression, as well as increases psychological well-being. 40 The results of the present study are consistent with those of a previous study that t'ai chi significantly reduces sadness, confusion, anger, tension, and fear. 41 The present study suggests that t'ai chi plays a positive role in improving mood disorders such as depression and anger. An alcohol rehabilitation program in Sam-Bong Psychiatric Hospital comprises of education about alcohol, a prescribed drug, singing, painting, listening to music, writing poetry, planting, group sharing, and counseling. However, exercise was not included in this program. Alcohol-dependent patients whose alcohol intake is restricted strictly usually suffer from depression related to strong cravings for alcohol, a desperate feeling of forced admission, and the other various causes. This likely drives the patient to being more depressed and reduces their motivation to exercise. It is presumed that the outcomes showing significantly decreased serotonin levels and increased depression are related to the circumstances in control group from before to after testing.
The outcomes indicating increased serotonin blood levels and decreased nicotine dependence, depression, and anger are consistent with those of a previous study. 13,17,39 Hart claimed that serotonin itself is not a determining factor, but only regulates mood (depression, anxiety), obsession, compulsion, pain, and the drive for alcohol, nicotine, and food. 17 Therefore, caution needs to be exercised in determining whether serotonin is a casual factor in outcome findings. To clarify casual relation between variables, repetitive trials are required in the future.
This study has several limitations common to a nonequivalent control group non-synchronized studies, the possibility of intervening exogenous variable, including the small sample size (N = 38), relatively short intervention duration, and no intent to treat analysis identifying correlation between variables. However, this study provides important preliminary data about the efficacy of t'ai chi in vulnerable patients.
In conclusion, t'ai chi was effective in reducing negative emotions of depression, anger, and nicotine urges, as well as increasing the blood serotonin level in alcohol-dependent patients. This study supports the feasibility and acceptability of t'ai chi among patients with alcohol dependency. In the future, various effects of long-term t'ai chi use in alcohol-dependent patients need to be studied. If the results are confirmed in a larger and longer intervention, t'ai chi exercise could become an important component in a rehabilitation program for these patients.
Footnotes
Acknowledgments
The authors are grateful to Dr. Yoon-Young Lee of the Sam-Bong Psychiatric Hospital.
Author Disclosure Statement
No competing financial interests exist.