
Abstract
Objectives:
Integrative medicine (IM) has been recognized and introduced into Western healthcare systems over the past two decades. Limited information on IM models is available to guide development of an optimal healthcare service. A scoping review was carried out to evaluate IM models in the extant literature, including the distinctive features of each model, to gain an understanding of the core requirements needed to develop models of IM that best meet the needs of patients.
Design:
Directed content analysis was used to classify the IM models into systems based on coding schema developed from theoretical models and to identify the key concepts of each system.
Results:
From 1374 articles identified, 45 studies were included. Models were categorized as theoretical and practical and were subdivided into five main models: coexistence, cooptative, cooperative, collaborative, and patient-centered care. They were then divided into three systems—independent, dependent, and integrative—on the basis of the level of involvement of general practitioners and complementary and alternative medicine (CAM) practitioners. The theoretical coexistence and cooptative models have distinct roles for different health care professionals, whereas practical models tend to be ad hoc market-driven services, dependent on patient demand. The cooperative and collaborative models were team-based, with formalized interaction between the two medical paradigms of conventional medicine and CAM, with the practical models focusing on facilitating communication, behaviors, and relationships. The patient-centered care model recognized the philosophy of CAM and required collaboration between disciplines based around patient needs.
Conclusions:
The focus of IM models has transferred from providers to patients with the independent and integrative systems. This may require a philosophical shift for IM. Further research is required to best understand how to practice patient-centered care in IM services.
Introduction
I
The growth in IM practice has been paralleled by debate in the literature regarding optimal models of IM and patient care. This debate has lagged behind delivery of care, with an ad hoc growth of CAM services within community and hospital-based systems. Consequently, there has been opportunistic service development, often without adequate support for sustainable growth and long-term delivery of care. 7 In practice, comprehensive access to health promotion, disease prevention, and community-based CAM is often absent, with conventional medicine taking precedence over CAM. 8 When CAM does occur in hospitals, it is rarely integrative in nature. Although hospitals view CAM as profitable, devaluation of CAM by conventional medicine leads to marginalization in the hospital system. 9
Few studies have described how IM services are delivered and what IM models are used. The aim of the current study was to (1) describe the characteristics of selected models of IM, (2) describe the types of IM models according to their theoretical and practical frameworks, (3) categorize the practical models based on a coding schema developed from selected theoretical models, and (4) describe the key concepts and issues for each system.
Materials and Methods
Literature search
By following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 10 a scoping review was performed in five stages: (1) identifying the research question, (2) systematically identifying studies, (3) study selection, (4) data extraction, and (5) collating and summarising results. 11
The literature was searched for models of IM, including type, process, and structure. The search strategy was based on the following Medical Subject Heading (MeSH) terms: complementary and alternative medicine/Traditional Chinese Medicine, integrative medicine, and integrative system or model. A variety of terms and definitions of CAM and comprehensive and inclusive MeSH terms were used and are shown with the complete search strategy in Supplementary Appendix I, Supplementary Table A.1 (Supplementary materials are available online at
The following databases were searched, from inception through October 2015: PubMed, Ovid Medline, PreMEDLINE, EBM Reviews All, Allied and Complementary Medicine (AMED), PsycINFO, Global Health, and CINHAL (Supplementary Appendix I, Supplementary Table A.2). Additionally, a keyword search was performed in Google Scholar and the reference lists of identified studies.
Study inclusion and exclusion criteria
English-language studies using any methods were included, as were articles discussing the theoretical frameworks of models or development of practical models of integrative medical programs. Excluded were articles that were not model or system based (e.g., those reporting use or patterns of CAM or IM); studies of a single treatment modality (e.g., yoga or acupuncture only); news articles, letters, non–full-text articles; unpublished abstracts; and ongoing studies. Articles restricted to particular populations (e.g., pediatrics) and individual diseases (e.g., HIV) were excluded.
Non–peer-reviewed articles, including conference proceedings, interview papers, reports, and dissertations, were included if sufficient data were available. All articles were screened by title, keywords, and abstract according to the flow chart of inclusion and exclusion criteria (Fig. 1). Figure 2 summarizes the reasons for excluding articles at each step.
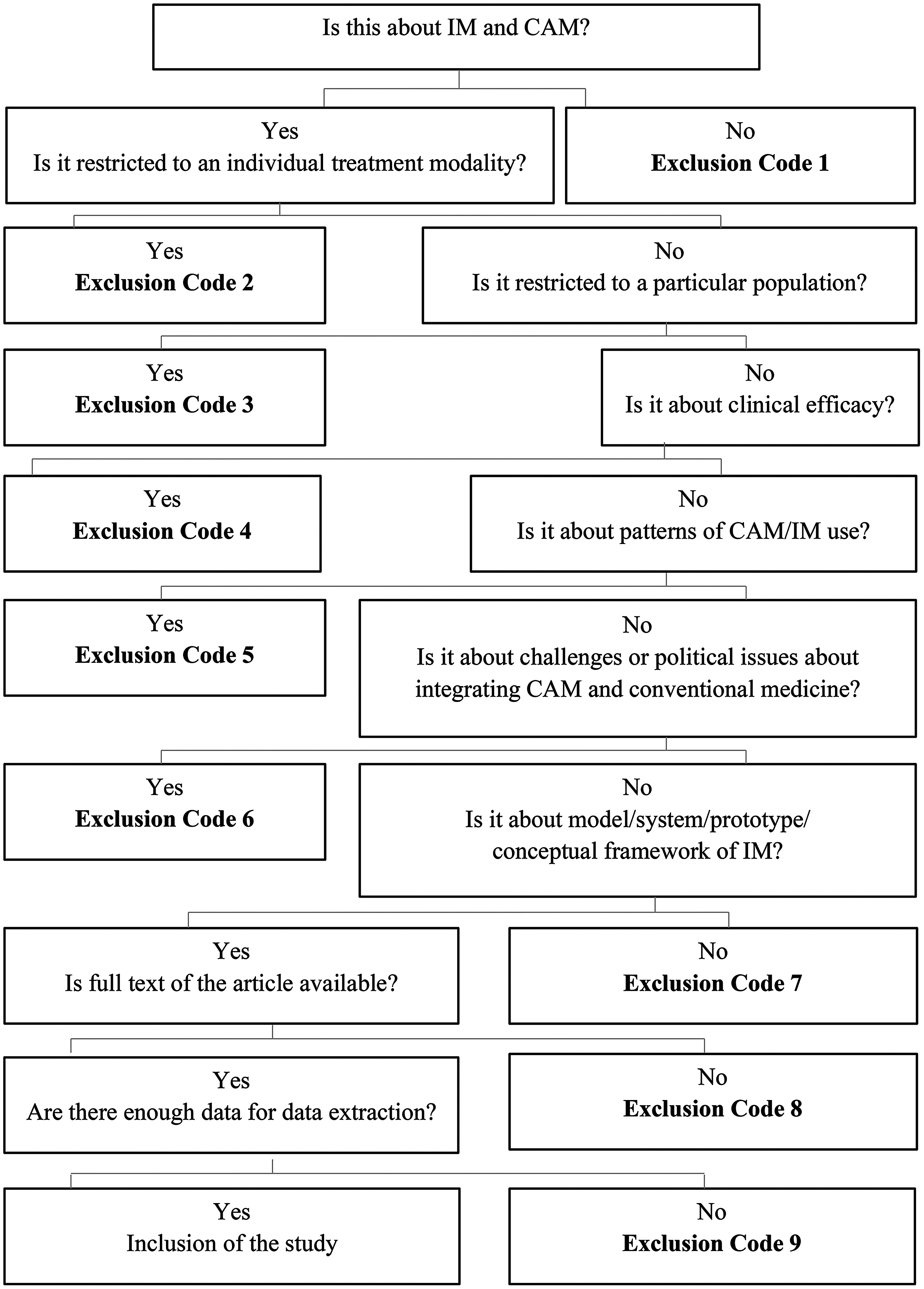
Flowchart of study screening and eligibility. Code 1, articles not about models of integrative medicine (IM) and complementary and alternative medicine (CAM) (n = 83); code 2, studies evaluating an individual modality (e.g., acupuncture) (n = 158); code 3, studies in specific group (e.g., pediatrics) (n = 164); code 4, studies about clinical efficacy of intervention (n = 117); code 5, studies on patterns, beliefs, and perception of CAM/IM use (n = 256); code 6, studies on cost-effectiveness, scientific evidence issues, policy, and health reform (n = 238); code 7, studies on general definition and philosophy of IM (n = 114); code 8, studies without full text or not in English (n = 26); code 9, insufficient data to extract for analysis (n = 26).
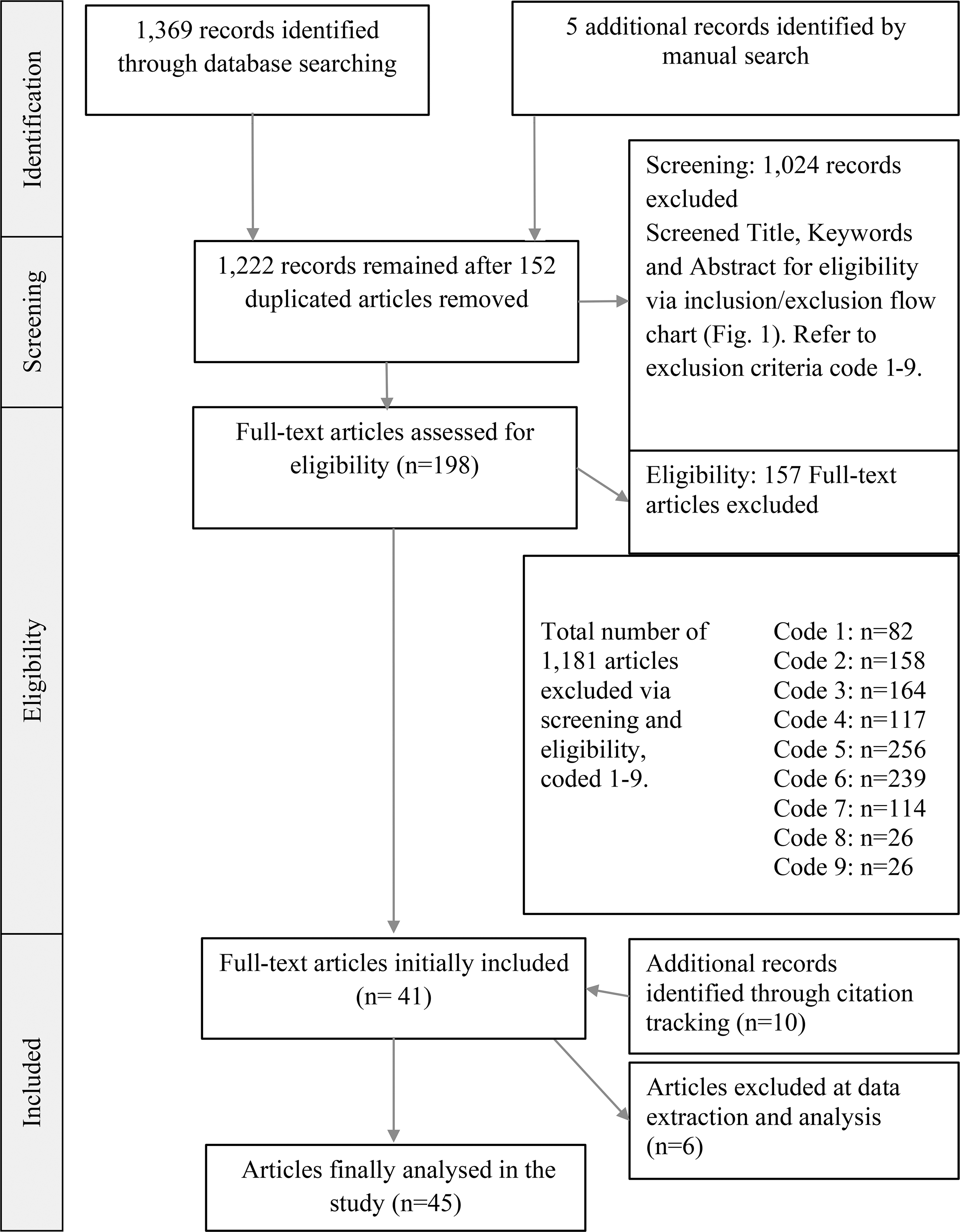
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) process of study identification. Codes are defined in legend to Figure 1.
Data extraction and analysis
The data extracted included author(s), year, country, study design, types of models, description of the model, objectives, and study findings. Two investigators (E.J.L. and H.M.D.) randomly selected 10 studies from the included articles and independently extracted data, resolving any discrepancies by discussion to reach consensus.
A qualitative directed content analysis approach 12 was used to conceptually extend a theoretical framework or theory. The selected papers were divided into two frameworks: theoretical and practical. First, to develop an initial coding schema, the descriptions, definitions, or key features of 20 models were extracted from six randomly selected papers suggesting theoretical IM models. Data were then entered into HyperRESEARCH (version 3.0, ResearchWare, Inc.) for coding into main themes. To further refine the coding schema, the schema was applied to the remaining theoretical models to assess its comprehensiveness, with codes for new concepts added when necessary. Second, the practical models were categorized into systems based on the coding schema. Finally, the contextual data were collected and analyzed according to each system.
Results
The initial search identified 1374 articles; 152 were duplicates, leaving 1222 articles to be screened. Initially, 41 articles were included, with another 10 added after reference list checking. Six studies were excluded at data extraction because of insufficient data. A total of 45 studies were included (Fig. 2) and divided into theoretical or practical frameworks (Table 1). The 14 theoretical and 31 practical models are summarized in Supplementary Appendix II (Supplementary Table B.1.2).
IM, integrative medicine.
Coding schema
From the 14 theoretical models, four main themes were identified (patient, cooperation, medical framework/philosophy, and provision of CAM services), along with 14 subthemes (Table 2). Each model was conceptualized into systems based on the themes.
IM, integrative medicine; CAM, complementary and alternative medicine; GP, general practitioner; IP, integrative physician; HCP, healthcare provider.
Categorization of models
The IM models were categorized into five main models based on Table 2: coexistence, cooptative, cooperative, collaborative, and patient-centered care (PCC). These fit into three main systems: independent, dependent, and integrative (Fig. 3).
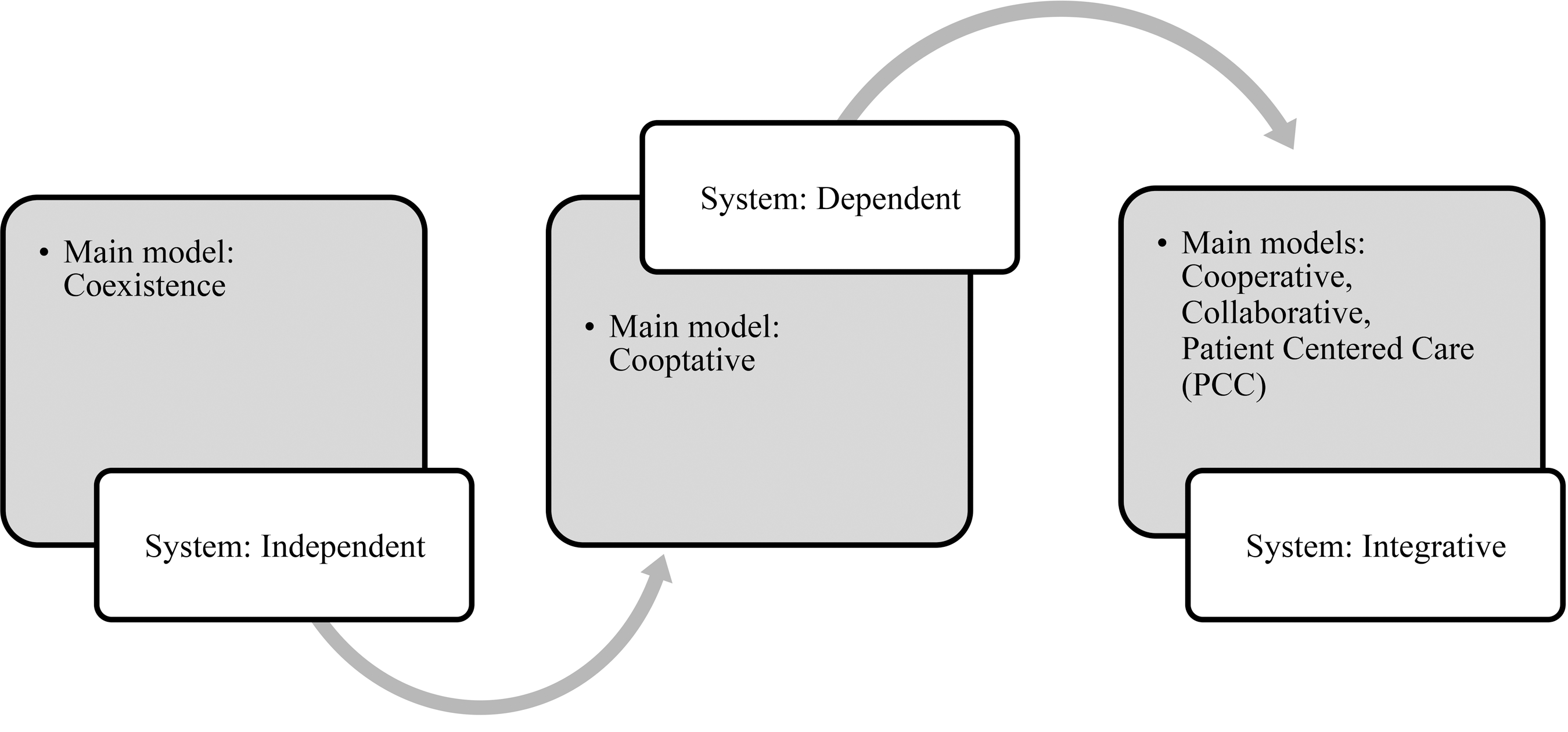
Classification of systems and main models applied models in the literature.
Independent systems
The coexistence model, the main model of independent systems, involves minimal interaction between the two medical systems, with each working independently in practice and clinical decision-making. This has been termed a parallel system, 13 or avoidance patterns, in which an integrative approach is avoided because of conceptual conflict rooted in distrust between the two systems. 14
Theoretically, the definition of the coexistent models showed clear distinctions between CAM and conventional medicine in the scope and role of practice, based on patients' freedom to choose treatment and being responsible for their decision. 8,15,16 The challenges were knowledge flow between the two medical practices and practical implementation, which differed depending on healthcare provider (HCP) preferences and issues of safety, cooperation, and resources required. 8,16,17
Most practical models could be defined as variations on the parallel model, wherein conventional medicine and CAM are practiced and practitioners educated separately within the health system (e.g., in Taiwan, South Korea, India, and Africa). 18 –20 A series of case studies explored five coexistent-model approaches that included sessional CAM practitioners onsite with conventional medical services; the services operated independently, with a variable level of GP involvement. Often the GP owned the practice, renting space to CAM practitioners, but their structure, setting, and funding varied. These models originated from a desire by some GPs to work with CAM, or from local health needs, and were funded from a health authority or a charitable trust. 21
CAM practitioners preferred a model that enabled them to maintain professional autonomy but described a cultural divide with GPs. GPs preferred a model that did not need involvement of CAM practitioners in regular meetings, but CAM practitioners wanted more communication and interaction with primary care staff. 21
Theoretically, coexistent models have a distinct separation between CAM and conventional medicine, but some practical models had characteristics of the dependent system, such as the requirement for GP referral or control over CAM treatment. Additionally, CAM practitioners indicated concerns regarding cooperation, communication, and functional operation (e.g., inadequate number of referrals, lack of funding) in these settings. These concerns are different from those of Bodeker's parallel models. 20 Bodeker highlighted the importance of retaining theoretical concepts as the basis of CAM, an idea supported by other parallel models, which advocate for reconciliation of different theories and philosophies of human health during the integration of CAM into conventional medicine. 20 Some authors suggested that CAM must first be integrated into a national health care system before cooperation in these parallel models can be considered. 18,19,22 Systematic approaches for integration included individual, institutional, and political integration to control the legitimacy of CAM provision, particularly with regard to fees, insurance, and patient safety. 2,8,19,20,22 –24
Dependent systems
The cooptative model, the main model of dependent systems, conceptualises IM as the process of selective incorporation of CAM elements, but based on the diagnostic methods of conventional medicine. 25 Consequently, CAM services are highly dependent on conventional medicine. 8,25 The International Bioethics Committee described dependent systems as inclusive systems, in which CAM is recognized within the public health system, but no CAM legislation or education curriculum are established. 13 Two different modes of delivering CAM services are physician-provider, 14 in which CAM-trained physicians provide the CAM service, and dominating integration pattern, in which GPs make referrals to CAM services, 14 thereby providing an interface connecting the two medical systems. 25
Cooptative theoretical models reflect dominating integration patterns, which are likely to be ad hoc in nature and on a case-by-case basis. This model allows limited interaction between professionals, but feedback mechanisms were absent. 15
The physician provider model may be suboptimal as bringing the two medical paradigms into one risks loss of CAM's natural context, which may reduce its clinical impact, and marginalize the provision of CAM. 8,16 The strength of these models is that the GPs are knowledgeable about CAM. 16,17 This improves communication with patients, reduces risk to patients' health and GPs' reputation, enables a broader range of service provision for patients, and permits reimbursement for the fees for CAM services. 8 Conversely, both models require additional resources (financial outlay, CAM education programs, and professional time) with CAM education for GPs and accreditation of CAM practitioners. 17
Three types of CAM service provision, grouped by provider, were identified in practical models. In the first (GP gatekeeping), the CAM trains GP/integrative physician (IP) consults with the patient before CAM provision and then refers or directly provides CAM. In the second Allied Health Practitioner (AHP-led), HCPs, including nurses, provide CAM services or referrals. In the third (ad hoc type), HCP or CAM practitioners are trained to provide a range of CAM services, based on patient demand and availability of services. The third model is most commonly used in hospital settings. 26
The literature highlighted issues with lack of connection between the services, in both the theoretical and practical models. Problems identified included absence of feedback and referral mechanisms, poor quality of referral information, and lack of time for patient case discussions and CAM education. CAM service provision depended on primary health care services, raising concerns regarding the risk of losing the essential features of CAM in the theoretical physician provider model. From a practical stance, the models were concerned with obtaining referrals and ensuring that CAM service provision was multidimensional and able to meet patient requirements and demands, and were seen as market driven.
Integrative systems
The integrative system, conceptualized as transformative integration patterns, is a dynamic and interactive relationship between the two medical paradigms with multidisciplinary arrangements. 14 This definition allows flexibility in developing the model to suit individual institutional environments. This system was divided into three main models: cooperative, collaborative, and PCC. Each involves interaction between teams or disciplines. The main cooperative models are characterized by separate decision-making but consist of multidisciplinary teams. The collaborative models are based on shared decision-making, building consensus from the collaborative team and a partnership with patients and involving interdisciplinary teams with a nonhierarchical blending of CAM and conventional medicine. 27 The PCC models are an advanced version of the collaborative models, with greater focus on patient involvement in planning of treatment. They are more patient-led, with less professionally centered structure, and greater acknowledgement of the clinical value of both medical paradigms compared with the collaborative model.
Main model 1: cooperative
Theoretically, CAM practitioners and HCPs make their own clinical decisions but engage in a formalized interaction, such as communication and sharing of patient records between teams. 27 A case coordinator or team leader may oversee information and develop treatment plans.
The practical cooperative models also highlight commitment to working as a team but with variable GP/IP involvement. GPs were highly involved in a patient advocacy role and as team leader for CAM provision. One study expressed concerns regarding discrepancies in integration, negative perceptions about weekly team meetings, and power conflicts between professionals. 21
The consultative or multidisciplinary model facilitated interaction within the team, with the GP/IP as an interface between disciplines and stakeholders. The consultative care model was reported to be the most common form of IM delivery in the United States. The IP, CAM practitioners, and patient's GP worked as a team throughout the referral process, 28 with an IP providing a consultation and treatment plan when referring patients to CAM services. 29 This model was called the linking model, 30 with networking among stakeholders a core value.
Reason et al. identified three concerns in the evaluation of a multidisciplinary practice: different diagnostic approaches between therapists, obtaining general agreement between HCPs for the psychosocial context of patients, and the relationship between practitioner and client. 31 They recommended collectively working on developing expertise to gain a deeper understanding of the patients' condition, 31,32 with more focus on clinical aspects and finding agreement between practitioners in a team.
Main model 2: collaborative
Theoretically, collaborative models were characterized by several disciplines working together to develop a consensus for patient care. Boon named the models emerging from the multidisciplinary model interdisciplinary and integrative. 27 It differs from the cooperative model in that it involves the creation of a new structure with the aim of shared decision-making and consensus building. Many studies expressed the importance of providers from both medical paradigms forming a nonhierarchical, interdisciplinary team, with focus on the team rather than their individual professions. 33 Kaptchuk and Miller articulated concern about the maintenance of the integrity of CAM, indicating that it was limited or controlled by conventional medical practices. They argued that conventional medicine and CAM are incompatible in their philosophies, epistemologies, and clinical practices. 34
In practical models, Bodeker defined collaborative IM as the integration of conventional medicine and CAM/Traditional Chinese Medicine (TCM), through medical education and practice. 20 Examples include health systems in China and Vietnam, 20 where medical practitioners receive training in CAM/TCM as part of their medical training at universities. 20,35 There is an emphasis on eliminating unscientific or non–evidence-based aspects of CAM/TCM, thereby controlling the terms and process of integration. 20,35 However, Bodeker argues that this results in a loss of important aspects of traditional theory and practice. 20
Several studies focused on the relationship between stakeholders in this model. Gaboury et al. described interprofessional collaboration as “the interaction between health professionals who work inter-dependently to provide care.” 36 A survey of CAM practitioners and GPs working in IM clinics found skills and behavior processes of the team (knowledge exchange, communication, trust, cooperation, GP centrality) were more relevant to the outcome of collaboration (job satisfaction, personal growth, level of conflict) than was team structure. 36 These models included explicit philosophical statements regarding patient involvement and aimed to provide multidimensional support during and after conventional medical treatments. 36,37
The collaborative model required specific interest from GPs to provide the required organization and guidance. In Weeks and colleagues' study, GPs did not value CAM highly but still expressed interest in CAM education. Seventy-one percent of GPs believed better integration would lead to satisfied patients, and up to 93% of CAM practitioners expressed interest in educational programs to facilitate integration, including referral procedures, resource management, insurance, medical records, and the role of the GP as gatekeeper. 38
Main model 3: PCC model
The pluralization model contains characteristics of both independent and integrative systems; it has separate IM clinics that preserve the respective systems but integrates around shared decision-making. 14,25 The most notable distinction from the other models is recognition of CAM philosophy and diagnostic methods. Both medical systems are practiced independently but are integrated with all aspects of treatment being patient centered. The main type of pluralist model is the PCC model, in which health consumers decide on the level of integration. 25 The relationship between medical pluralization, PCC, and true integration is important for understanding this model.
In theoretical models, Kaptchuk and Miller believe that the pluralization model fosters tolerance and cooperation between conventional medicine and CAM. It demands education on both sides, but each system's strengths can flourish, and weaknesses can be perceived through collaboration and self-reflection. 34 They argue that as it accepts and recognizes the philosophical differences between CAM and conventional medicine in developing a method of integrated medical knowledge, it can foster integrity in both systems, and that expansion of legitimate treatment options may improve informed choice and facilitate communication between HCPs and patients. 34 This links to Lekridge's PCC model, which promotes freedom of choice through information and empowerment. Lekridge emphasized the biopsychosocial model as capable of integrating two opposite medical paradigms: mechanism (conventional medicine) and vitalism (CAM). 16,39,40 The biopsychosocial model fits the integration category as it maintains the middle ground between the biomedical approach and the holistic-energy approach, 40 synthesising empirical evidence with clinical knowledge. 8 This type of model is the one most likely to support the development of “truly” integrated medicine. 16,25
In practical models, the concept of the pluralization model goes beyond structural integration. Johnson listed 25 interpretations and definitions of integrated medicine. 41 The key themes were (1) PCC, (2) collaboration of health management and treatment, (3) connectivity for consensus and mutual understanding, and (4) encompassing a philosophy that goes beyond inserting CAM into a medical system. He described PCC as the patient being seen as an entire entity rather than as a case or disease, and he revised the term from “patient” to “person,” viewing PCC as an essential component of evidence-based practice that incorporates clinical experience and patient values. 41
While Johnson provided a definition of PCC and interpretation of IM, Maizes and colleagues focused on structuring care, interacting with patients according to their needs, and imparting the concept of health to patients. PCC was described as care that informs and involves patients in medical decision-making and self-management, providing physical and emotional support, understanding cultural beliefs, and applying the principles of disease prevention. 7 They suggested a team-based IM model in which a team tailored for each patient's condition is formed. The practitioners are selected from both hospital and community according to the patient's treatment plan, with communication facilitated by an IP. 7 This concept is similar to the Tibetan model, in which conventional medicine and CAM work independently but with cross-referral according to patient need. 42
Maizes et al. stated that systematic change, with a commitment to disease prevention and health promotion, is needed for IM healthcare service providers and models. Preventive care and health promotion require different skills, such as motivational skills and ability to elicit and understand patient beliefs and values. 7 Giordano et al. developed this concept in a public health framework parallel to biomedical evidence. 43 Several authors support Maizes' model as representing a combination of selected effective treatments of both CAM and conventional medicine.” 6,44 The model emphasized that equal autonomy, input, and standing between CAM and GPs; biomedical evidence; clinical efficacy; and health outcomes are all valued. 6 Although described as the most effective model, it is rarely achieved in healthcare settings 9 and may be an unachievable ideal given the epistemological divide. 6,44 However, Giordano et al. argued that an epistemological shift is important to investigate, validate, and evaluate the practices within the different forms of care. 43
Discussion
While previous research has described IM service models, details regarding the models have generally been brief or noncomparative descriptions. This scoping review identified 45 papers discussing aspects of IM models, which were categorized into theoretical and practical models, and further classified into systems, to identify the goals of IM care and the concerns associated with each type of service. The findings illustrate that while theoretical concepts provide a distinctive framework for each model, there are some discrepancies between theoretical and practical models.
The theoretical models of the dependent and independent systems describe differentiated roles for HCPs and CAM practitioners, but most practical models tended to be ad hoc, with a loosely coordinated structure and crossover of professionals' roles. In the integrative system, the cooperative and collaborative theoretical models outlined team-based multidisciplinary and interdisciplinary types of services, while the practical models focused on teamwork and the relationship between professionals and patients.
In general, changes in the IM models used occurred over time, with the provider-oriented IM models (coexistence and cooptative) moving to team-oriented (cooperative and collaborative) and then patient-oriented (PCC) models. Concurrently, there was a move from independent to integrative systems, with both theoretical and practical settings emphasizing a transfer of focus in IM healthcare delivery from providers to patients. The PCC model combined concepts of the independent and integrative systems, requiring collaboration within teams, and acknowledgment of CAMs clinical value.
Open communication was regarded as the key facilitator to overcome the lack of structural cohesion, 30,45,46 but team cooperation and building of interdisciplinary relationships between professionals and patients were often reported to be challenging. Communication barriers between the disciplines were compounded by philosophical differences between the two medical paradigms and concerns by CAM practitioners regarding maintaining the integrity of CAM due to the dominance of conventional medicine and GPs in IM. 9,25,47 This was seen as impeding the development of truly equal, integrative teams. 47 Approaches such as improving doctor training and attitudes toward CAM, 48 improving biomedical knowledge among CAM practitioners, and acknowledging the limitations of each system were recommended. 42
Poor coordination in CAM service provision was evident. 45,49 CAM practitioners, including AHPs, indicated concerns with lack of GP referrals and cross-referrals between practitioners, leading to overservicing by other IM healthcare providers due to lack of coordination. 47 Fragmentation of CAM provision was thought to have led to the development of structurally complex multidisciplinary models. 41
This review is the first to systematically investigate theoretical and practical approaches to IM systems and models and provide a framework to further integrate conventional medicine and CAM. On the basis of this review, the authors recommend the PCC model. It acknowledges the value of both paradigms, facilitates collaboration between team members, and places the patient as the focus of primary importance. Focus on the following factors is likely to significantly improve patient outcomes and be key to successful integration: reciprocal knowledge exchange; providing GP education on referral guidelines to CAM practitioners; competency of CAM practitioners; individual characteristics of care providers; and communication, trust, and cooperation between professionals. 6,36,50
This review has several limitations. Models were classified according to the coding schema of the theoretical models. Classifications proved difficult, with individual models plausibly fitting into more than one system. Models with multiple characteristics were categorised according to their main conceptual characteristic. Hospitals that provide multiple types of IM services and models may be underrepresented. This review focused on broad conceptual models of complementary and integrative medicine to describe the context of integration, but the search terms were limited to CAM and TCM (including Chinese herbal medicine or acupuncture). Inclusion of a broader range of search terms for individual CAM therapies may have led to identification of additional references describing models of care. Thus, further reviews, including other CAM terms, may add to the findings of this review. Because many of the articles were written by practitioners with a personal interest in CAM, issues presented may overrepresent their opinions.
IM models of care remain susceptible to institutional culture, 30,51 structure, and funding, 25 as well as clinical conflicts between the two medical paradigms. 22 Further research is therefore required to investigate IM in different settings, concentrating on how best to offer PCC, and to bridge the philosophical divide. Without this, the establishment of improved practical models of IM will remain challenging.
Despite major differences between the models, all are encompassed under the term “integrative medicine.” This highlights the need for a clearer definition of integrative medicine. Furthermore, some authors recommend that “integrative healthcare” differs from integrative medicine, 52 believing that the former term acknowledges a broader range of determinants and inter-relationships of human health. 53
Conclusions
Three primary systems support the integration of CAM and conventional medicine (independent, dependent, and integrative). Articulating the systems that support integration of the two medical paradigms enables individual services, practitioners, and patients to consider the model most appropriate for their needs and setting. For the field to progress, a deeper understanding of the concerns of the two systems and the implications for integration is required. To achieve this, greater openness and communication are essential.
Footnotes
Acknowledgment
This work was supported by University of Sydney Postgraduate Awards, Australia.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.