
Abstract
Objectives:
The purpose of the study was to determine (1) recruitment feasibility; (2) intervention adherence; (3) intervention acceptability; and (4) the preliminary effects of touch or foot massage interventions on anxiety during a magnetic resonance imaging (MRI).
Design:
A quasi-experimental design was used.
Intervention:
Foot massage and touch were the intervention groups and “presence” was the control group.
Setting:
The study was conducted at the Center for Neurosciences, a freestanding facility, in southern Arizona.
Participants:
The sample (N = 60) was predominantly Caucasian (58.3%), married (55%), and college educated (43.3%). There were 39 females and 21 males. Fifty-three percent of the participants had an MRI head scan.
Outcome measures:
Recruitment feasibility was the percentage of participants enrolled out of those screened. Adherence to foot massage and touch interventions was measured by the researcher's ability to apply full intervention for 20 min. Four factors measured participants' acceptance of the interventions as follows: (1) comfort; (2) acceptability of the length of the treatment; (3) perception of effectiveness; and (4) recommendation of treatment as part of routine MRI care. The MRI technologists' acceptability was measured by whether the intervention: (1) disrupted the workflow and (2) affected the length of the scan. State anxiety was assessed verbally by a single 10-point Likert type item.
Results:
Recruitment feasibility was 78.2%. There were no barriers to the intervention protocol for 91.6% participants. The overall mean value of perceived effectiveness was 8.53, SD = 2.4 on a 10-point Likert type question. There was a significant difference among the three groups in terms of perceived effectiveness of the intervention F (2, 57) = 15.19, p < 0.001. Multilevel modeling documented that the foot massage intervention was a significant predictor of decreasing anxiety (β = −1.35, SE = 0.63, p < 0.01).
Conclusion:
The use of foot massage or touch is feasible, acceptable by patients and technologists, and the use of foot massage was associated with lower state anxiety.
Introduction
M
Nonpharmacologic interventions to decrease MRI related anxiety such as counseling, relaxation, cognitive training, anxiety reduction training, 8 use of guided relaxation, 9 and the use of aromatherapy 10,11 have been studied. However, most of these interventions are not practical, are time consuming, require practice, and need to be introduced a few days before the MRI scan. Use of prerecorded music 12 and live music 13 have also been studied to decrease anxiety during MRI. However, the clanking noise of the scanner is so loud (130 dB) and frequent that it can be hard to hear the music. Sedation has been successful in decreasing anxiety, but adds additional cost and the possibility of adverse effects requiring additional patient monitoring time and care. 14 Although most MRI units use various techniques in an attempt to reduce anxiety, new interventions are needed to improve patient support and decrease disruptions during the scan. 15
Complementary and alternative medicine (CAM) approaches include nontraditional elements of health rooted in the physical, psychologic, environmental, and spiritual. 16 One particularly effective application of CAM is massage therapy, which has been shown to have various positive effects on psychologic and physical symptoms, including depression and anxiety. A meta-analysis of 37 studies that included healthy adults, HIV-positive adolescents, patients with headache, and patients with Parkinson's disease 17 reported that even a single application of massage therapy was effective in decreasing state anxiety (g = 0.37, p < 0.01), blood pressure (g = 0.25, p < 0.02), and heart rate (g = 0.41, p < 0.01). Thus, it appears that massage therapy could be a highly effective and widely applicable method to decrease MRI-related anxiety.
Higher anxiety has been reported among patients entering head-first (e.g., head or upper body MRI scans) into the bore compared to patients inserted feet-first (e.g., lower body MRI examination). 18 Foot massage, then, may be a feasible, novel, and holistic intervention for these patients whose feet are the only available body parts for massage therapy. No studies have been conducted to date to determine if foot massage reduces anxiety in patients undergoing MRI. A prior study has shown that foot massage helps reduce anxiety in hospitalized cancer patients receiving chemotherapy. 19 In another study, a simple 5-min hand or foot massage decreased perceived levels of stress. 20 Foot massage resulted in a significant decrease in diastolic blood pressure and anxiety levels among long-term care staff providing care to older patients with dementia. 21
The purpose of this study was to examine the feasibility of holistic approaches and their effects in decreasing anxiety in patients undergoing MRI. The specific aims were to investigate (1) participant recruitment rates; (2) adherence to foot massage and touch interventions; (3) provider and participant's acceptability of physical presence, human touch, or foot massage interventions; and (4) the effects of touch or foot massage interventions compared to physical presence during MRI on anxiety.
Materials and Methods
A quasi-experimental design was used for this feasibility study. There were two intervention groups as follows: foot massage and touch. Subjects in the control group received only the presence of the researcher. “Presence” was considered a confounding variable as subject's anxiety can decrease merely because someone is present at the time of the scanning. Approval to conduct this study was obtained by the Institutional Review Board (IRB) of The University of Arizona.
Participants
Subjects were recruited from the Center for Neurosciences (CNS), 22 a freestanding facility, located in the U.S. Southwest, dedicated to the diagnosis and treatment of neurologic disorders. Potential participants were evaluated for eligibility criteria (Table 1). Demographic characteristics of the participants are presented (Table 2). There were 39 females (65%) and 21 males (35%); participants were predominantly Caucasian (58.3%), married (55%), and had a college or graduate degree (55.0%). There were no significant differences in age, race, income, marital status, ethnicity, annual family income, education, or body region being scanned among the three groups.
MRI, magnetic resonance imaging.
Interventions
The researcher, previously trained in foot massage techniques, provided foot massage for 20 min to individuals assigned to that group. A hypoallergenic massage lotion was used for massage. A series of steps (Table 3) were used for foot massage on both feet. Participants receiving the touch intervention were gently stroked on the lower legs for 20 min (10 min each leg). Touch intervention was provided using both hands applying gentle pressure, slow, long rhythmic strokes on bilateral legs while keeping constant contact with the skin. After providing foot massage or touch for 20 min (10 min on each foot), the researcher remained present with the participant until the scan was completed. The researcher remained present throughout the MRI scan with the participants in the presence only group.
Measures
Recruitment feasibility was operationalized as the percentage of participants enrolled out of the number of participants screened. Adherence to foot massage and touch interventions was measured by researcher's ability to apply the full intervention for 20 min, 10 min on each foot. There were four factors that determined participants' acceptance of the interventions during MRI: (1) comfort during treatment; (2) acceptability of the length of the treatment—whether the length of the intervention was too short, too long, or just right; (3) evaluation of the effectiveness of their experienced condition (foot massage, touch, or presence) on a single item, responses on a 10-point Likert type question, with one being not effective and 10 being very effective; and (4) recommendation of treatment as part of routine MRI care (dichotomous 1 = yes and 0 = no). The MRI technologists' acceptability was measured by two factors: (1) whether the intervention disrupted the workflow and (2) whether the intervention had an impact on the length of the scan.
The effects of the interventions were examined on state anxiety. Individuals diagnosed with trait anxiety were excluded from the study as they were more likely to be taking anxiolytic medications that could confound the results of the study. Anxiety was assessed using a single item verbally administered anxiety rating (VAR) scale. VAR is a 0–10 linear numerical rating scale in which a rating of 0 means no anxiety and 10 means the feeling of being terrified. A score of 5 or greater on VAR suggests anxiety. 23 Anxiety levels were measured before the patient was taken to the MRI, right after patient was positioned in the scanner, at ∼10 min (mean 10.77, SD = 1.0) into the scan, at ∼20 min (mean = 20.55, SD = 1.4) into the scan for those whose scan lasted 20 min and longer, at ∼30 min (mean = 31.83, SD = 3.2) into the scan for those whose scan lasted 30 min and longer, and at the end of the MRI scan.
Data analysis
Descriptive statistics, including means, frequencies, and standard deviations, was used to describe sociodemographic information and state anxiety. A chi square test was used to determine group differences in acceptability for the length of the treatment and recommendation of the relevant condition (touch, foot massage, presence).
A one-way ANOVA was used to evaluate baseline group differences for all continuous demographics, state anxiety, and perceived effectiveness. Because there were differences between the groups on baseline state anxiety, it was used as a covariate in a preliminary repeated measures ANCOVA. As the data were hierarchically clustered, with repeated measurements (time) nested in participants and participants nested in intervention groups (foot massage, touch, presence), multilevel models were fit to the data. All analyses were conducted in statistical software SPSS. 24
Results
Aim 1: recruitment feasibility
Seventy-eight patients scheduled for MRI of the head and or spine were recruited at the CNS and screened for eligibility. Of the 78 patient recruits, 17 (21.8%) did not qualify for participation (Fig. 1). Since 61 participants were enrolled out of 78 screened participants, recruitment percent was 78.2%, supporting the feasibility of subject recruitment for CAM related studies during an MRI.

Flowchart of participants in the study. (Recruitment, enrollment, and data collection took place from May 2, 2015 to July 7, 2015).
Aim 2: feasibility of foot massage and touch interventions
Of the 20 participants, 18 received the full foot massage intervention for 20 min, 10 min on each foot. Two participants did not receive the full intervention because their scans lasted 15 and 18 min. Because the scan lasted less than 20 min, the researcher was able to massage the second foot for only 5 and 8 min, respectively, for these two participants.
Out of 20 participants in the touch group, 17 received touch for 20 min. There were three participants whose scans lasted for 15.2, 15.5, and 18 min; therefore the researcher was not able to provide the touch intervention for the full 20 min for these three participants. As with the application of foot massage, the touch intervention was disrupted by scan lengths of shorter duration times. As 85% to 90% received the foot massage and touch interventions without difficulty, these interventions were deemed feasible.
Aim 3: participant and provider's acceptability of the interventions
Participant acceptance
All of the study participants (N = 60) were comfortable during the foot massage, presence, or touch protocols. The length of the intervention was “just right” for the majority of the study participants (75%) (Table 4). The overall mean value of effectiveness was 8.53, SD = 2.4 on a 10-point Likert type question. There was a significant difference among the three groups in terms of perceived effectiveness of the intervention F (2, 57) = 15.19, p < 0.001. Post hoc analysis (Bonferroni) showed that participants rated touch (M = 9.1, SD = 1.1) and foot massage (M = 9.9, SD = 3) interventions as significantly more effective as did those who received the presence intervention.
The majority of the study participants (81.7%) recommended that these interventions (foot massage, presence, and touch) be part of routine MRI care. Overall, there was no significant difference among the groups in relation to participants' recommendation of the interventions (χ 2 = 9.467, p = 0.149).
MRI technologists' acceptability
There were four technologists who participated in the study. The MRI technologists' acceptability was determined by two factors as follows: (1) whether the interventions disrupted the workflow and (2) whether the intervention had an effect on the length of the scan. All the four technologists were supportive throughout the study and stated that these interventions were helpful to the participants in keeping them calm and they neither disrupted the workflow nor affected the length of the scan. An intervention that received mostly all positive remarks for each factor could be said to measure high in acceptability. There were positive remarks (97%) received for each factor determining acceptability of the interventions by the MRI technologists.
Aim 4: preliminary effect of foot massage, touch, and presence interventions on state anxiety levels during MRI
The scores on state anxiety stratified by intervention group across the four time periods, presented in Table 5, indicated mid-range state anxiety. At baseline, the state anxiety scores ranged from a mean of 3.74 (SE = 0.36) for the Foot Massage intervention group to a mean of 4.37 (SE = 0.35) for the Touch intervention group, with the presence control group with a mean of 3.81 (SE = 0.32). The Touch intervention group was significantly higher than the Foot Massage group. Notably, the state anxiety scores decreased over the four measurements for all three groups. This is illustrated in Figure 2.
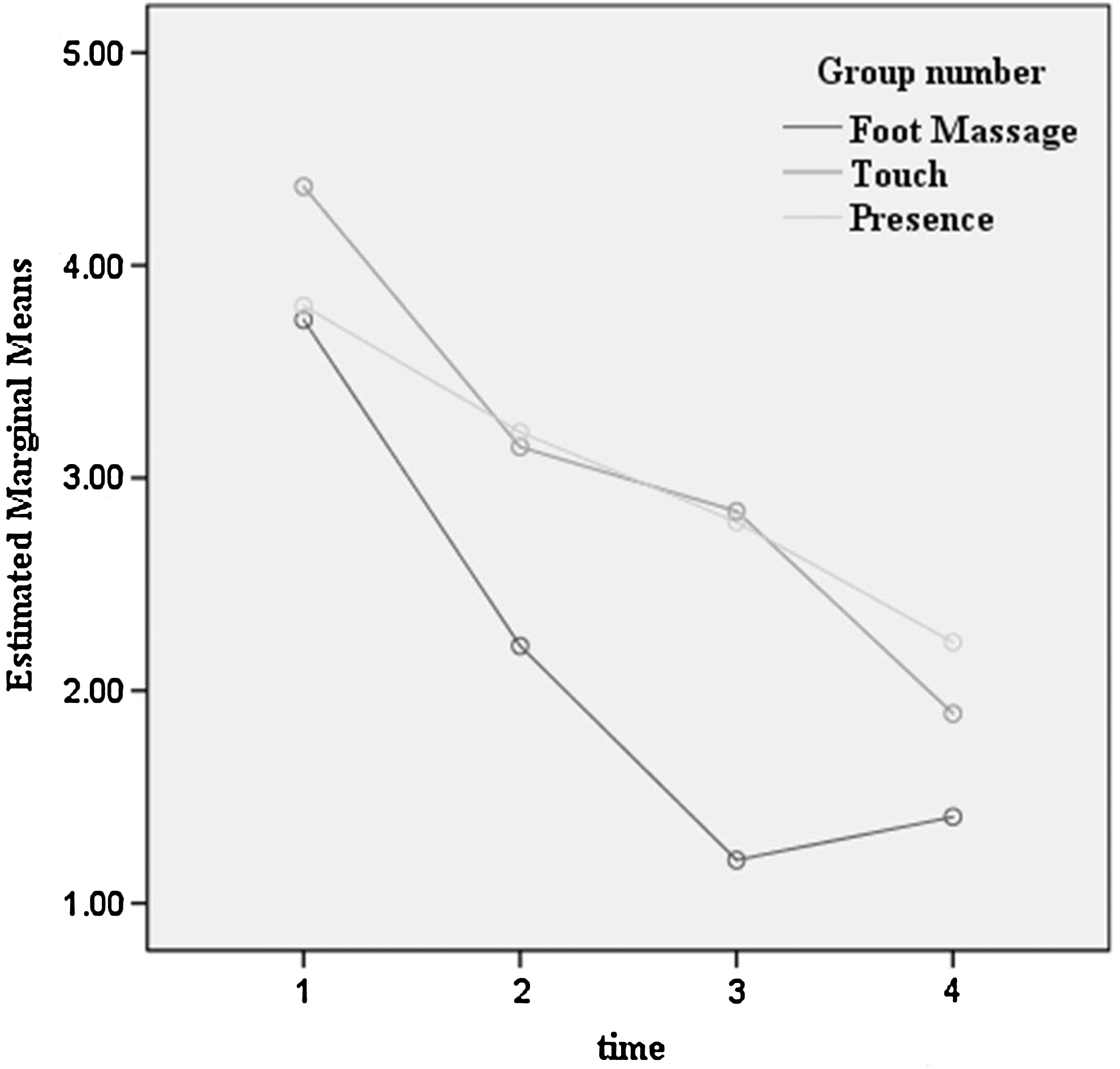
Anxiety differences over time by intervention groups for MRI scans. MRI, magnetic resonance imaging.
To determine if there were statistically significant differences over time by intervention group, the authors fit a series of multilevel models to the data. These are presented in Table 6. The first model was an unconditional model examining mean differences in anxiety at baseline. The intraclass correlation was 0.58 indicating that 58% of total variation in anxiety was due to interindividual differences. Model 2 tested the effect of time on the rate of change in anxiety over time. The value of both intercept and linear slope parameters was significant indicating that the baseline and linear growth rate significantly varied over time. The mean estimated baseline anxiety was 4.31 (SE = 0.41, p < 0.001), and the linear growth rate of the sample was −0.43 (SE = 0.77, p < 0.001), indicating that the state anxiety levels decreased almost half a point between each measurement.
p < 0.01
p < 0.001.
Models 3 and 4 tested whether the group assignment (Foot Massage, Touch, and Presence) was related to differences in state anxiety. The Foot Massage group reported significantly lower state anxiety (β = −1.33, SE = 0.63, p < 0.01) than did the Presence group (control), and the Touch group did not report a significantly lower state anxiety (β = 0.55, SE = 0.63, p = 0.390). Models 5 and 6 tested curvilinear time effects. Quadratic and cubic polynomials made significant contributions to the models (p < 0.001). The final model, model 7, included linear and curvilinear effects of time and tested whether the intervention groups reported a statistically significant difference in state anxiety over time. The negative effect of quadratic growth (β = −1.48, SE = 0.55, p < 0.01) indicated a decrease in the rate of change, and the positive effect of cubic growth (β = 0.369, SE = 0.14, p < 0.01) suggests that the decrease diminished over time. Most importantly, the Foot Massage intervention group reported a significantly greater decrease in state anxiety than did the control group (β = −1.33, SE = 0.63, p < 0.01). The Touch Intervention did not report a significant difference in state anxiety than did the control group (β = 0.54, SE = 0.63, p = 0.395). The unstructured covariant structure was the best fit to estimate the error for the overall model.
Discussion
All the participants included in this study had a previous MRI, because the study setting was a referral center where most patients coming to this center had had previous neurologic studies. It has been reported that self-reported anxiety is usually highest with the first MRI scan but decreases with subsequent scans. 4 However, in this study, 43.3% of the participants remained anxious despite a previous scan. Other studies have reported that anticipatory anxiety is experienced by about 37% of all patients undergoing this examination. 1,14,25
Female participants (46.2%) reported higher prescan anxiety compared to males (38.1%). This finding is similar to the finding by Katz et al. 1 who reported that female patients had higher prescan anxiety than males. The highest anxiety levels were reported at the beginning of the MRI session. The use of holistic measures helped decrease the anxiety level at the end of the session. Chapman et al. 4 reported that the highest anxiety levels were at the beginning and at the end of the MRI scan.
A total of 61 participants were eligible to participate in the study. One participant (1.6%) was not able to begin the scan because of claustrophobia and hence the scan had to be aborted. This finding is comparable to findings from other studies, which have revealed that estimations of terminated sessions due to anxiety ranged from about 2% 4 to 5%. 3 The length of the intervention was just right for the majority of the study participants (75%). However, 8.3% of the participants mentioned that they would have preferred the intervention (foot massage/touch) for the entire length of the scan. This is the first feasibility study that examined foot massage, touch, and presence during MRI. However, several other investigators have reported the use of 10- and 20-min long foot massage sessions during hospitalization. 26 –28 Future studies that compare the effect of different lengths of foot massage and touch interventions on anxiety during MRI are needed.
Other studies have used physiologic and psychologic measures to determine the effect of foot massage. 26 –29 Future studies should incorporate physiologic measures in addition to the psychologic measures to determine the length of foot massage session that is the most effective for patients undergoing MRI.
One survey of radiographers found that 71.6% reported that patient anxiety was an issue for MRI scans. 15 Radiographers have reported that disruptions of scans due to anxiety are still prevalent, despite the use of information provision, music, communication with radiographers, and sedation. 15 Tischler et al. concluded that there is a need for more patient support to improve patient experiences and lower the costs of disruptions due to anxiety. This finding may explain why MRI technologists were very supportive throughout this study.
Hattan et al. 27 noted a significant effect of a 20-min foot massage on self-reported calmness in patients after a coronary artery bypass graft surgery. In this study, there was a significant decrease in anxiety with foot massage. The anxiety score of the foot massage group at the end of the MRI scan remained lower compared with the other groups. Although there are no studies to date examining presence, touch, and foot massage as interventions in MRI settings, several have reported that the use of massage decreased anxiety during hospitalization 26,28 and among postoperative patients. 30 –33
This feasibility study had several limitations affecting its generalizability. First, a convenience sample was drawn from a single community neuroscience center. Participants from other hospitals or MRI centers were not included. Second, the lack of randomization limits the ability to generalize the results of this study to any other MRI settings or to the entire MRI patient population. Third, state anxiety was measured by a single 10-point Likert type Item which can have greater error than a robust scale. Finally, baseline anxiety levels may have been affected by knowledge of group assignment before the baseline measure was administered.
With respect to group assignment, those assigned to the Foot Massage group had a baseline anxiety that was lower than the other two groups. It is possible that knowledge of group assignment may account for lower anxiety in the Foot Massage group. Future studies that include patients undergoing MRI for the first time and the length of time for which the intervention is provided are needed. Nonetheless, the findings from this feasibility study suggest that these holistic interventions may also be effective in other hospital settings and/or during other diagnostic testing. In addition, for young children having an MRI, the use of holistic measures needs to be explored.
Conclusion
This study tested the feasibility, acceptability, and preliminary effects of a holistic approach to interventions and their effect on anxiety during MRI. In this study, there was a significant difference among the three groups in terms of effectiveness of the intervention. Foot massage was the most effective in decreasing anxiety.
Footnotes
Author Disclosure Statement
No competing financial interests exist.