
Abstract
Objectives:
Low back pain (LBP) is a chronic condition. Although Western treatments are available, Kampo (traditional Japanese) medicine is widely prescribed and covered by health insurance in Japan. Goshajinkigan (GJG), a Kampo formula, is commonly used to treat LBP. However, cases we have occasionally been encountered in which GJG did not show the expected effects. Hence, the purpose of this retrospective study was to investigate patient factors important in developing the effects of GJG.
Methods:
This was a retrospective observational study based at the Center for Kampo Medicine, Keio University Hospital. Data were retrieved from the medical records of 28 patients who visited our hospital between May 2008 and March 2013 and who received GJG for LBP. The patients were divided into responders and non-responders based on whether their LBP improved post treatment. The groups were compared with respect to daily GJG dose, incidence of spine disease, and side effects.
Results:
Ten patients (responders) reported an improvement in LBP within 6 months. One patient experienced decreased appetite as a side effect. Nine patients reported no improvement (non-responders). The number of patients prescribed the usual daily dose of GJG (7.5 g) was significantly higher among responders than it was among non-responders (p = 0.023), and the number of patients with spine disease was significantly greater among non-responders than it was among responders (p = 0.020). The number of patients with spinal stenosis was significantly higher among non-responders than it was among responders (p = 0.011). Therefore, the usual daily dose of GJG provided significant relief of LBP, particularly in patients without any spine disease.
Conclusions:
Routine daily administration of GJG in patients without spine disease seems to lead to the effects of the product. However, further investigations using the above-mentioned parameters are needed to confirm these findings.
Introduction
T
Goshajinkigan (GJG), a Kampo formula, is considered to be an effective treatment for LBP in elderly patients and has been used empirically in Japan. Recent evidence has shown that it is also very effective for treating numbness in patients with peripheral nerve disorders caused by anticancer agents, 6 –8 diabetes mellitus, 9,10 and nocturia. 11
The authors routinely prescribe GJG to patients with LBP. However, occasionally cases have been encountered in which GJG did not show the expected effects. Hence, the purpose of this retrospective study was to investigate patient factors important in developing the effects of GJG. To this end, patients who had LBP and received GJG were divided into responders and non-responders, and the differences between the two groups were investigated. Patient factors important in developing the effects of GJG were identified.
Methods
Study design
In this retrospective study, data were collected for patients who visited the Center for Kampo Medicine at Keio University Hospital and who were treated with GJG for LBP between May 2008 and March 2013. The patients were followed up until the end of March 2013, and the data up to this point were collected and analyzed. The study was approved by the Institutional Review Board at Keio University School of Medicine, and written or digitally recorded informed consent was provided by all registered patients.
Participants
The inclusion criteria were a consultation for LBP at the department and undergoing treatment with GJG. The exclusion criterion was refusal of informed consent.
Drugs
GJG extract granules are marketed by Tsumura & Co. (Tokyo, Japan). A single dose contains 2.5 g, and the usual daily dose for an adult is 7.5 g. This dose contains 4.5 g of a dried extract of the following mixed crude drugs: Rehmannia glutinosa Liboschitz, radix 5.0 g, Achyranthes fauriei H. Lev. & Vaniot or Achyranthes fauriei Blume, radix 3.0 g, Cornus officinalis Siebold & Zucc., fructus 3.0 g, Dioscorea japonica Thunb. or Dioscorea batatas Dence., rhizoma 3.0 g, Plantago asiatica L., semen 3.0 g, Alisma orientale (Sam.) Juz., rhizoma 3.0 g, Poria cocos Wolf, sclerotium 3.0 g, Paeonia suffruticosa Andrews, cortex 3.0 g, Cinnamomum cassia Blume, cortex 1.0 g, and Aconitum carmichaelii Debeaux or Aconitum japonicum Thunb., radix 1.0 g.
GJG is produced by Tsumura & Co. under the national health insurance service in Japan. The harvest site of the crude drugs contained in GJG did not change during the study period. The quality of the product is checked regularly and rigorously by a pharmaceutical company to meet the Japanese pharmacopeia under the good manufacturing practice regulations.
Outcome measures
General patient characteristics (e.g., sex, age, body mass index, medical history, daily dose of GJG, and combination therapy including GJG) were assessed from the medical chart on the first visit to the clinic. In the medical history, spine diseases causing LBP were carefully collected and counted for each disease (e.g., compression fracture, spinal stenosis, herniated disc, and spondylolisthesis), with some overlapping in some patients.
The effect of GJG on LBP was investigated by medical chart review, and the data were analyzed as the first endpoint of the research. When there were patient statements indicating improvement in LBP at the follow-up consultation, the treatment was considered to be “effective” at that time. Conversely, when there were statements of no improvement in LBP at the follow-up consultation, the treatment was considered to be “ineffective” until the end of March 2013 or the time Kampo formula was changed. If there was no statement concerning a change in LBP at the follow-up consultation, the effect of GJG was counted as “no mention.” Side effects of GJG were also investigated by medical chart review throughout the follow-up period. Consensus was reached by the investigators regarding the data extracted from the medical charts.
The duration from the start of treatment with GJG to the time when GJG was judged to be “effective” was also noted. Finally, with respect to general characteristics, the differences between responders and non-responders were investigated by comparing the two groups, in which a dose of GJG was considered to be the one prescribed for the longest duration during the entire follow-up period, and a typical case was noted.
Statistical analysis
Statistical comparisons were performed using R v3.1.1 (The R Foundation for Statistical Computing, Vienna, Austria;
Results
Twenty-eight patients (aged >65 years) received GJG, and their general characteristics are listed in Table 1. The median duration from onset of LBP to the start of treatment with GJG was 60 months (range 2–576 months). The types of treatment prescribed in combination with GJG were analyzed. Of these 28 patients, 16 received GJG combined with Western medicine, and three received it in combination with other alternative therapies, including acupuncture, moxibustion, or massage (Table 2).
BMI, body mass index; GJG, goshajinkigan; LBP, low back pain.
CAM, complementary and alternative medicine; NSAIDs, non-steroidal anti-inflammatory drugs.
The therapeutic effects and side effects of GJG were analyzed. Of the 28 patients, 10 reported an improvement in their LBP, nine reported no improvement, seven did not report their treatment outcome, and two visited the center only once (Table 3). The rate of non-response to GJG among the 28 patients is shown using the Kaplan–Meier method in Figure 1. The median duration from the start of treatment with GJG to improvement of LBP in the responders was 2.5 months (range 0.75–6 months). Among the responders, decreased appetite as a side effect was observed in one patient (Table 4).
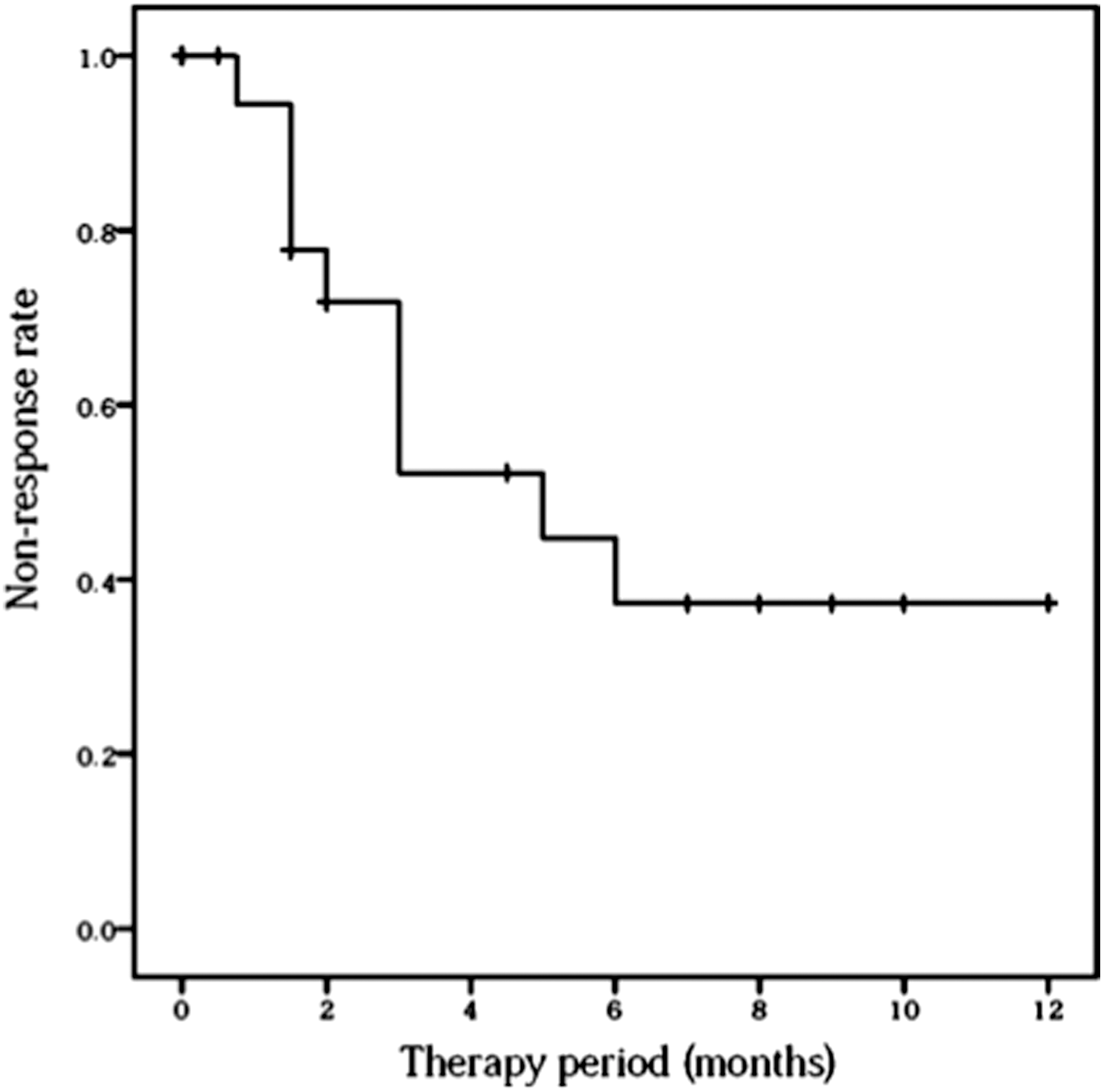
Rate of nonresponse to treatment with goshajinkigan among 28 patients.
A comparison of general characteristics was performed between the responders and non-responders. The daily dose of GJG was not changed throughout the follow-up period in either the responders or the non-responders, except for one responder whose daily dose was changed from 5.0 g to 7.5 g, and the period for which the 7.5 g dose was prescribed was much longer than that for 5.0 g. So this patient's daily dose was treated as 7.5 g in line with the study methods. Significantly more responders than non-responders were prescribed the usual daily dose of GJG (7.5 g; p = 0.023), and there were significantly more non-responders than responders with spine disease causing LBP (p = 0.020). A subgroup analysis of spine disease causing LBP revealed that significantly more non-responders than responders had spinal stenosis (p = 0.011; Table 5).
The daily dose of GJG was deemed to be the dose prescribed for the longest duration during the follow-up period.
p < 0.05.
Typical case
The case is reported of an 80-year-old woman who had suffered from chronic LBP since her mid-50s and had a medical history of hypertension and diabetes mellitus. She was prescribed topical non-steroidal anti-inflammatory drugs (NSAIDs), and had undergone acupuncture and moxibustion. From 70 years of age, her LBP had worsened. At the age of 80 years, she underwent a Kampo examination in the authors' department. The orthopedic cause of her LBP was unclear, but it tended to worsen with exposure to cold temperatures, and she also complained of general fatigue, dizziness, nocturia, and cataract. GJG (7.5 g/day) was prescribed, and one month later her fatigue resolved and she became more active. Three months later, she felt a warm sensation in her lower back, and her LBP improved. Finally, her self-reported visual analog scale score decreased from 100 to 50.
Discussion
This study retrospectively investigated patient factors important in developing the effects of GJG, a Kampo medicine formula. Twenty-eight patients were treated with GJG for LBP, and these patients were divided into two groups—responders and non-responders—based on whether their LBP improved after treatment. The general characteristics of the two groups were compared. It was found that the daily GJG dose was significantly higher and that spine disease causing LBP were less frequent in responders. A side effect in the form of mildly decreased appetite was seen in only one patient, and so it can be inferred that GJG is a safe treatment.
NSAIDs and acetaminophen are recommended first-line for LBP in medical treatment guidelines, 12,13 and most of patients included in our research also received these Western treatments. From research on combination therapy, when the patients who did not report their outcomes were excluded, 16/20 (80.0%) patients received Western medication. Further, 12/20 (60.0%) received oral or topical NSAIDs. According to these data, most patients with LBP probably received Western treatment first, and those who did not experience any improvement in LBP then likely opted for other treatments, such as Kampo medicine.
GJG is used primarily to treat symptoms associated with kidney qi deficiency in Kampo medicine. Characteristic symptoms associated with kidney qi deficiency include general fatigue, weakness in the lower back and knees, dizziness, tinnitus, pollakiuria, and nocturia. 14 These symptoms are found more frequently in the older population, and for this reason GJG is empirically considered an effective treatment for LBP in elderly patients. The focus of this study was improvement of LBP, and so other symptoms were not recorded in detail. However, some patients did report improvement in other symptoms, including fatigue, neck and shoulder stiffness, night sweats, dizziness, and tinnitus. The typical case mentioned above reported that not only the patient's LBP but also other symptoms such as fatigue and decreased activity were improved by treatment with GJG. Based on the concept of Kampo medicine, these improvements are believed to be because of the improvement of kidney qi deficiency.
In this study, only two daily doses of GJG were explored. The effect of GJG extract granules, not a decoction, was investigated. The daily dose is specified under the national health insurance service in Japan. A single dose of GJG extract granules contains 2.5 g, and the usual daily dose for an adult is 7.5 g. Normally, 7.5 g per day is prescribed for an adult, and sometimes this is reduced to 5.0 g per day depending mainly on the patient's body weight and bowel status. Therefore, all patients included this study took 7.5 g or 5.0 g per day, and these daily doses are common.
To use GJG more effectively, it is necessary to understand what types of LBP would be refractory to treatment. First, according to a recent report, if LBP that involves the lumbar spine structures does not resolve within 3 months, the risk of developing chronic LBP increases. 15 In this study, the median time since the onset of LBP was 60 months, so LBP of this duration could perhaps be more difficult to cure. Second, it has been reported that the natural clinical course of spinal stenosis is often poor, and patients often undergo surgical treatment. 16 In this study, sub-analysis of spine disease causing LBP found that if patients had spinal stenosis, their LBP tended to be refractory to treatment. Western methods are not always satisfactory for treating LBP caused by spinal stenosis, but the analyses suggest that the same is the case with Kampo medicine.
However, GJG was possibly effective in many cases of LBP refractory to Western medicine in the current research. With regard to the effects of GJG, if the seven patients who did not report their treatment outcomes and the two patients who visited the center only once were excluded, 10/19 (52.6%) patients showed a good effect of GJG on LBP. Moreover, if cases of spinal stenosis are excluded, this number increases to 10/14 (71.4%). Although LBP improved in 2.5 months from the start of GJG treatment when taking the average value in the responders, the last patient with LBP took 6 months to improve (Fig. 1). Although the responders comprised only 10 patients and the evidence does not directly mean that it is worthwhile to continue treatment for 6 months, it has occasionally been found that Kampo formulae take 6 months of daily clinical consultation to show their effects.
One of the herbs in GJG is processed Aconiti radix, which has well-known analgesic properties. It is reported that the mechanism of analgesia differs between processed Aconiti radix and NSAIDs. Suzuki et al. reported that processed Aconiti radix stimulated spinal kappa-opioid receptors via release of dynorphin, which subsequently activates the descending pain inhibitory system and increases the anti-nociceptive effect. They also indicated that GJG and processed Aconiti radix showed dose-dependent anti-nociceptive effects in mice. 17 Their findings could be one explanation for the observation that the combination of GJG and NSAIDs was useful in some patients, and that GJG at a daily dose of 7.5 g/day controlled pain significantly better than the lower daily dose. It also seemed that GJG showed its effects if the daily dose was increased to 7.5 g/day in non-responders who previously received the daily dose of 5.0 g/day, and the same improvement was found in one patient among the responders.
Further, other ingredients in GJG have also been reported to have anti-inflammatory properties, and some of these have been evaluated for their analgesic properties. Catalpol, an iridoid glucose of Rehmannia glutinosa, has been shown to have an anti-nociceptive action associated with modulation of neuroinflammation in the spinal cord in rats. 18 Achyranthosides E and F, triterpene glycosides isolated from Achyranthes fauriei, have also shown anti-inflammatory properties via inhibition of the interaction between neutrophils and E-selectin. 19 Cornuside, a secoiridoid glucoside compound isolated from the fruit of Cornus officinalis, suppresses lipopolysaccharide-induced inflammatory mediators in macrophages. 20 Extract of Dioscorea japonica was shown to modulate markers of peripheral neuropathy in a mouse model of type 2 diabetes. 21 Further, Aucubin, one of the main components of Plantaginis asiatica, was shown to inhibit exacerbation of paclitaxel-induced mechanical allodynia in mice. 22 Sesquiterpene, diterpene, and triterpene, the main terpenoids included in Alisma orientale, have been shown to have diverse pharmacological actions, including diuretic, nephroprotective, anti-hyperlipidemic, anti-atherosclerotic, anticancer, anti-inflammatory and anti-oxidative activities. 23 3β-p-hydroxybenzoyldehydrotumulosic acid, a triterpene derivative isolated from Poria cocos, showed marked inhibitory activity against ear inflammation in mice. 24,25 Paeniflorin and oxypaeniflora, the two major compounds in Paeonia suffruticosa, showed anti-oxidative and anti-inflammatory activities in vitro. 26 E-cinnamaldehyde and o-methoxycinnamaldehyde, the most abundant compounds in Cinnamomum cassia, showed anti-inflammatory activity in vitro. 27 However, it should be noted that the above findings come from basic research and cannot be extrapolated directly to humans. Although less is known about the mechanism via which GJG exerts its analgesic activity in LBP, it may be that this effect is not only attributable to processed Aconiti radix but also other ingredients in this compound.
In this study, one (3.6%) patient experienced decreased appetite, which indicates gastrointestinal disturbance as a potential side effect. This might have been caused by Rehmanniae radix or processed Aconiti radix. This side effect of Rehmanniae radix is well known empirically, and one of the components, stachyose, is thought to be the cause. It can be treated by stopping GJG. Gastrointestinal disturbance is also a well-known side effect of processed Aconiti radix, and is caused by its constituent alkaloids, which include aconitine, mesaconitine, and hypaconitine. Regarding the clinical features of toxicity, patients present with a combination of neurologic, cardiovascular, and gastrointestinal features. However, the Aconiti radix is used only after processing, which reduces the alkaloid content by up to 90%. 28 Unfortunately, the frequency of toxic effects of processed Aconiti radix has not yet been reviewed thoroughly. However, there is no report of a serious side effect leading to death resulting from prescription of GJG extract. If a side effect appears, it can be reversed by stopping GJG.
This study had several limitations that warrant mention. First, it was retrospective and non-randomized in nature and included a small sample size. Second, observational bias may have affected the results. The improvement in pain was not quantified using, for example, the visual analog scale, but was based on subjective information obtained from medical records. So there is a possibility that relevant details on the medical record were incomplete. Moreover, although attempts were made to minimize bias by reaching consensus about information drawn from medical charts, some degree of observational bias might have been inevitable. Third, patient compliance could not be assessed. Ideally, a check should have been as to whether the patients took GJG according to the prescription, but the medical chart review method used in this retrospective study precluded gathering of this information. Fourth, other symptoms should have been investigated, such as general fatigue, dizziness, and tinnitus, which are also associated with kidney qi deficiency, to be able to conclude that improvement in LBP was the result of amelioration of this deficiency. In view of these limitations, a prospective study is needed for more accurate evaluation of the efficacy of GJG. A future study would need to include an adequate evaluation scale (including more symptoms associated with kidney qi deficiency), a clear endpoint, implementation of regular follow-up and monitoring, assessment of compliance, use of the usual daily dose of GJG (7.5 g), evaluation of spine diseases causing LBP, and a clearly defined observation period. With regard to the sample size in a future prospective study, in order to have 80% power while maintaining a significance level of 5% in a two-sided test when the difference in visual analog scale score between a GJG group and a control group is 15 and the standard deviation is 15 at the endpoint, 17 patients per group would be required to compare the two treatment groups using a chi-square test. To allow for possible dropouts, a minimum of 20 patients would need to be enrolled in each group (40 in total). This sample size would be similar to those used in previous studies of GJG. 9 –11
Conclusion
Routine daily administration of GJG in patients without spine disease seems to develop the effects of this product. However, further investigations using the above-mentioned parameters are needed to confirm these findings.
Footnotes
Acknowledgments
This study was presented as a poster at the 10th Annual International Congress of Complementary Medicine Research (ICCMR), Jeju, Korea, May 13–15, 2015.
Author Disclosure Statement
No competing financial interests exist in this research.