
Abstract
Objectives:
Health history questionnaires (HHQs) are a set of self-administered questions completed by patients prior to a clinical encounter. Despite widespread use, minimal research has evaluated the content of HHQs used in general internal medicine and family medicine (GIM/FM), integrative medicine, and complementary and alternative medicine (CAM; chiropractic, naturopathic, and Traditional Chinese Medicine [TCM]) clinics. Integrative medicine and CAM claim greater emphasis on well-being than does GIM/FM. This study investigated whether integrative medicine and CAM clinics' HHQs include more well-being content and otherwise differ from GIM/FM HHQs.
Methods:
HHQs were obtained from GIM/FM (n = 9), integrative medicine (n = 11), naturopathic medicine (n = 5), chiropractic (n = 4), and TCM (n = 7) clinics in California. HHQs were coded for presence of medical history (chief complaint, past medical history, social history, family history, surgeries, hospitalizations, medications, allergies, review of systems), health maintenance procedures (immunization, screenings), and well-being components (nutrition, exercise, stress, sleep, spirituality).
Results:
In HHQs of GIM/FM clinics, the average number of well-being components was 1.4 (standard deviation [SD], 1.4) compared with 4.0 (SD, 1.1) for integrative medicine (p < 0.01), 3.2 (SD, 2.1) for naturopathic medicine (p = 0.04), 2.0 (SD, 1.4) for chiropractic (p = 0.54), and 2.0 (SD, 1.5) for TCM (p = 0.47). In HHQs of GIM/FM clinics, the average number of medical history components was 6.4 (SD, 1.9) compared with 8.3 (SD, 1.2) for integrative medicine (p = 0.01), 9.0 (SD, 0) for naturopathic medicine (p = 0.01), 7.1 (SD, 2.8) for chiropractic (p = 0.58), and 7.1 (SD, 1.7) for TCM (p = 0.41).
Conclusions:
Integrative and naturopathic medicine HHQs included significantly more well-being and medical history components than did GIM/FM HHQs. Further investigation is warranted to determine the optimal HHQ content to support the clinical and preventive health goals of general internal medicine, family medicine, integrative medicine, and CAM practices.
Introduction
H
Recent healthcare reforms have sought to promote a medical home model of primary care better tailored to the unique needs of patients, particularly those with chronic medical diseases. 10 In 2013, the Agency for Healthcare Research and Quality published a step-by-step guide promoting periodic use and customization of HHQs in primary care medical clinics to better understand and engage patients in their health status, risk factors, and lifestyle. 11 Little is known about the content of HHQs, including length, format, and types of questions used nationally.
Integrative medicine and complementary and alternative medicine (CAM) claim greater emphasis on holistic and well-being–oriented care than mainstream allopathic GIM/FM. 12,13 Holism, from the Greek term holos meaning “whole,” is a concept inherent to understanding patients' well-being and includes exploring beyond physical function to also include the social, emotional, cognitive, and spiritual aspects of health. 14 Given the clear paucity of research evaluating question content and overlapping overarching goals and philosophies of these fields, this study evaluated HHQs used in GIM/FM, integrative medicine, and CAM clinics.
The aims of this study were to (1) evaluate the content of GIM/FM HHQs, (2) compare HHQ content used by integrative medicine and CAM, which claim greater emphasis on holism and well-being than does GIM/FM, and (3) explore possibilities to promote further research to develop and validate HHQ content and use for specific aims and populations (e.g., prevention, behavioral change initiatives). The hypothesis was that integrative medicine and CAM HHQs would include more well-being components than do GIM/FM HHQs and that GIM/FM HHQs would include more medical history components.
Materials and Methods
Study timing and sites
HHQ data were collected from July 2013 until September 2013, and data analysis occurred in 2014. Study sites included a range of clinic types that participate in primary care services. 15,16 Individual clinician offices were not included in the study. GIM/FM clinics were defined as allopathic medical clinics, which provide first contact primary medical care and are led by medical doctors (MDs) or doctors of osteopathy (DOs) who completed an accredited U.S. residency training program in internal or family medicine. 17
Integrative medicine clinics were defined as clinics led by physicians who emphasize a medical care model that is oriented toward a “holistic” and/or “integrative” philosophy. 12 –14 Given the variety of definitions and practice specifics, integrative medicine clinics were classified as community or academically affiliated clinic types. Community integrative medicine clinics were defined as privately operated, non–academically affiliated clinics offering general “integrative” medical services and staffed by a MD or DO. Academic integrative medicine clinics were defined as clinics that were member institutions of the Academic Consortium for Integrative Medicine and Health (ACIMH). 18 Naturopathic medicine clinics were defined as clinics led by a state-licensed naturopathic doctor (ND); chiropractic clinics were defined as clinics led by a state-licensed doctor of chiropractic (DC); and Traditional Chinese Medicine (TCM) clinics were defined as clinics led by a state-licensed nonphysician acupuncturist (licensed acupuncturist [LAc). 19
Search strategy and sample collection
Integrative medicine and CAM
A Google online search for “integrative medicine clinic[s],” “traditional Chinese medicine clinic[s],” “naturopathic medicine clinic[s],” and “chiropractic clinic[s]” located in the western region of Los Angeles County, including West LA, Santa Monica, and adjacent neighborhoods was used. All clinics that met the clinic type definition criteria and were in the target region were selected. An attempt was made to download the HHQ used for new patient visits from each website. If an HHQ was unavailable to download, it was requested by contacting via email or by visiting the clinic. There was only one ACIMH-member clinic in the target region, so the region was expanded to include all ACIMH member clinics located in California. 18
GIM/FM
A two-pronged search strategy was used. First, by using Google maps, local knowledge, and Google web search, a list of the following was compiled: academic university medical center, Veterans Affairs hospital–based, large private health system GIM residency teaching, low-income public teaching, private community-based GIM, and managed care hospital-based clinics located in the western region of Los Angeles County. Attempts to obtain the HHQs were first made via clinic website download, and if they were unavailable or if there was no clinic website, the clinics were visited in person. Second, because there were no Los Angeles County hospital clinics in the target area, two of the three county hospitals that draw on populations in this area were contacted.
Data Analysis
HHQs were evaluated for the presence of one or more questions relating to nine medical history components (chief complaint, past medical history, surgical history, prior hospitalizations, medications, medication allergies, social history, family history, and review of systems [a series of questions, organized by body organ systems, designed to elicit various symptoms] 20,21 ), two health maintenance procedure components (immunizations and screenings), and five well-being components (diet/nutrition, exercise, psychological stress, sleep, and spirituality). The percentage of HHQs was calculated for each clinic type that included each medical history, health maintenance, and well-being components (Table 1).
Unless otherwise noted, values are percentages.
Non-GIM/FM: combined data for IM, ND, DC, and TCM.
HHQ, health history questionnaire; GIM/FM, general internal medicine and family medicine; IM-A, academic integrative medicine; IM-C, community integrative medicine; ND, naturopathic medicine; DC, chiropractic medicine; TCM, Traditional Chinese Medicine.
The medical history components were based on the commonly used questioning topics used during routine annual physical examinations and new patient visit documentation in allopathic medical practice. 20,21 The social history component was counted as present when a question was included about tobacco, alcohol, illicit substance use, or sexual history. The healthcare maintenance procedure components were selected as those set forth by the U.S. Preventive Services Task Force (USPSTF) 22 and the Centers for Disease Control and Prevention adult vaccination schedule. 23 Other USPSTF recommendations that did not involve a specific test procedure, such as depression screening and healthy behavior assessments, were excluded from health maintenance categorization to avoid overlap with well-being history components. The well-being history components were chosen on the basis of a phenomenologic definition of health and common aspects reflecting proactive health-promoting patient behaviors or characteristics. 24,25
The mean number of review of system and well-being questions per HHQ was determined for each clinic type when the component was present (Table 2; reference Table 1 for percentage of HHQs that included each component). The percentage of HHQs including questions on medications and clarifying medications use as over-the-counter, vitamins, supplements, and herbs/botanicals for each clinic type was calculated (Table 3). Also calculated was the percentage of HHQs that included specific social history components, in order to show the variety of questions included (e.g., substance use, sexual history, caffeine use, relationship status) (Supplementary Table S1; Supplementary Materials are available online at
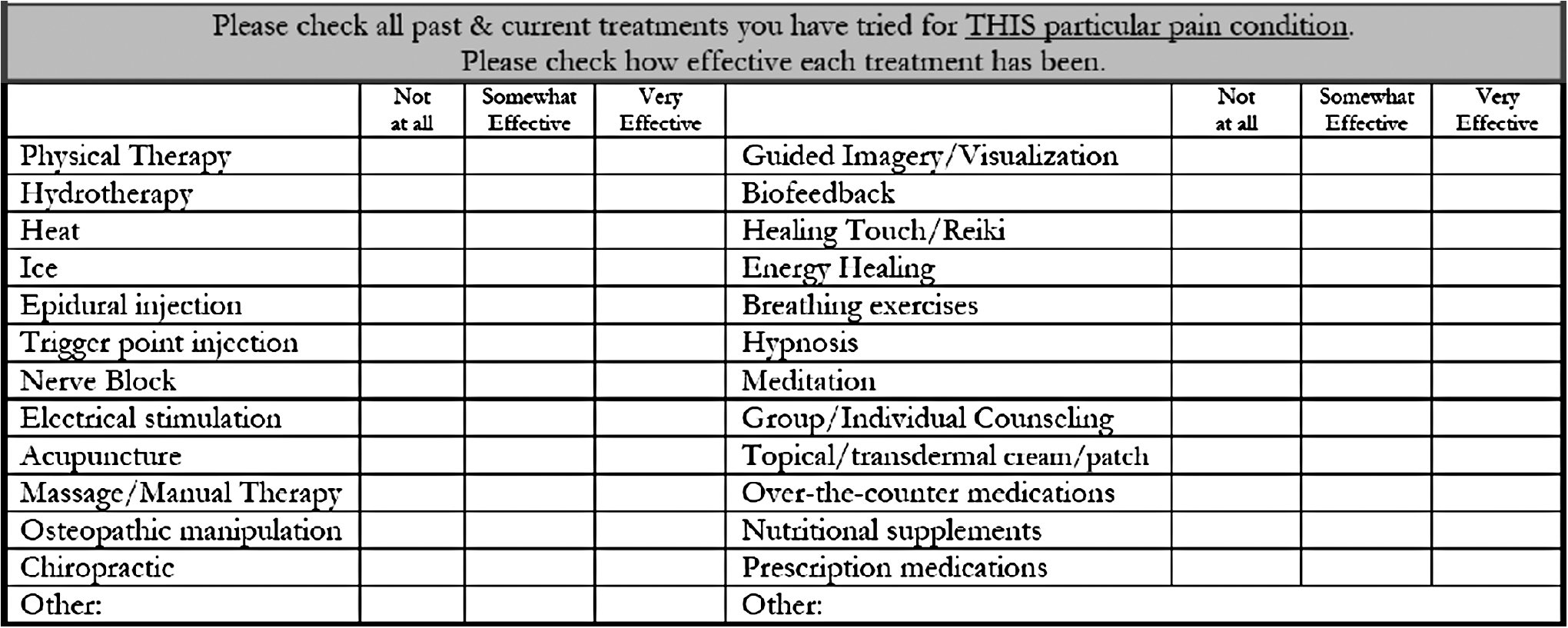
Questions regarding prior exposure to complementary and alternative medicine and mainstream therapies and their perceived effectiveness.
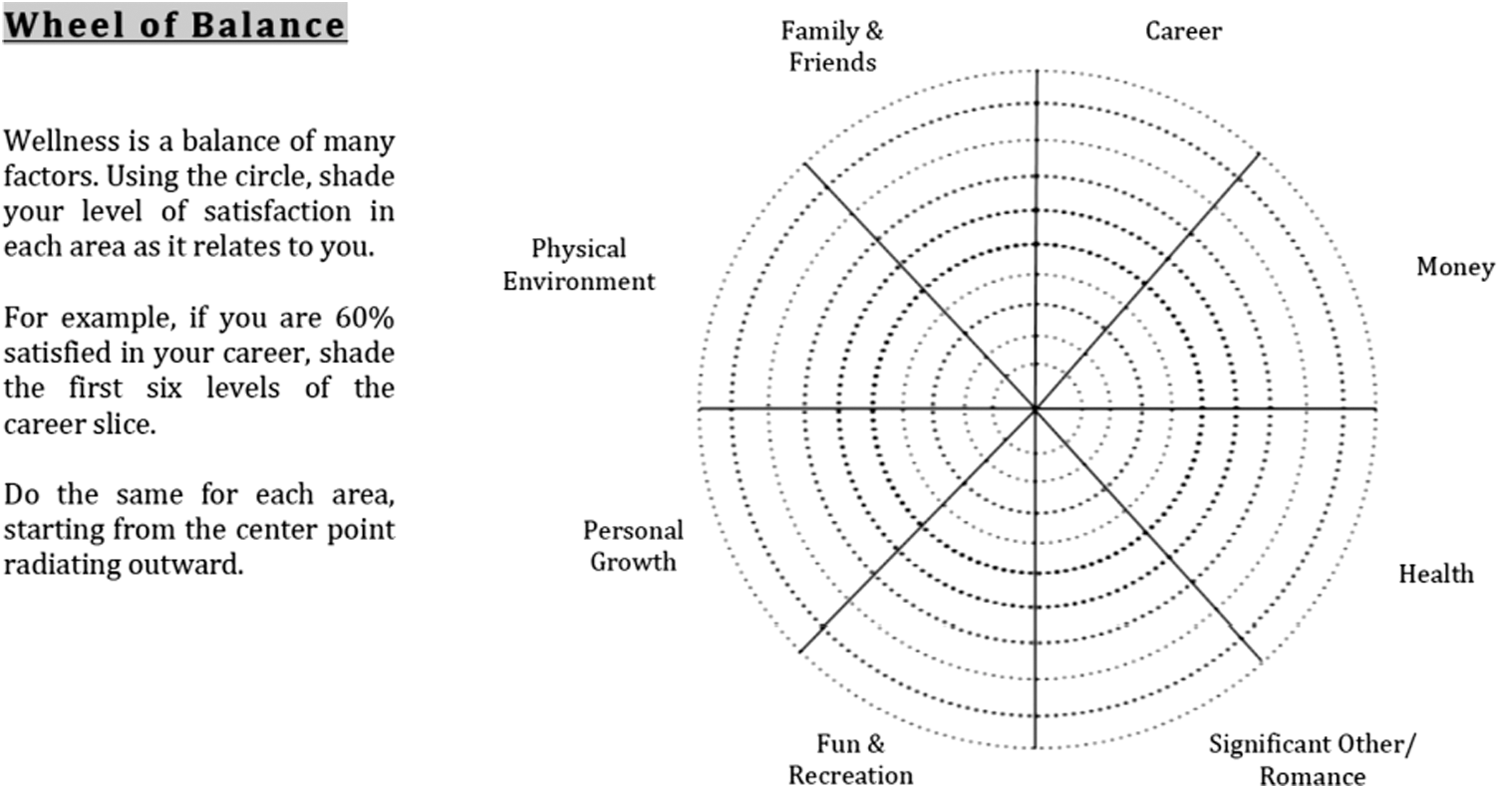
“Wheel of balance” well-being assessment.
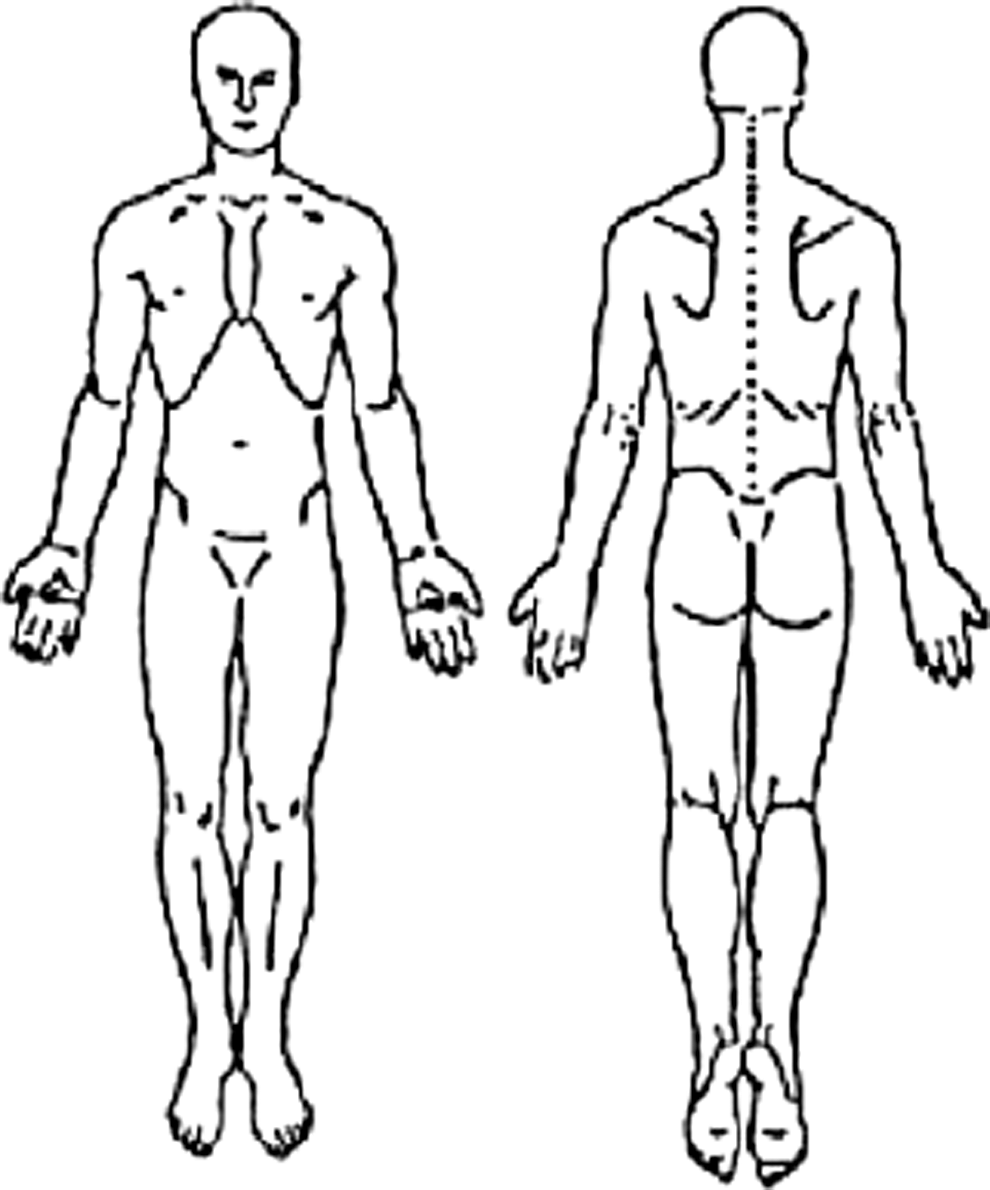
Body map used to draw pain/symptom location.

Traditional Chinese Medicine Health history questionnaire review of systems section categorized by the Chinese five-element Zhang/Fu organ systems.
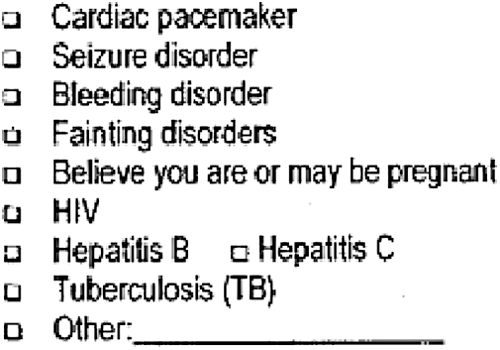
Traditional Chinese Medicine history questionnaire screening questions pertaining to risks to the patient or practitioner from receiving/performing acupuncture.
Values are expressed as mean (standard deviation).
Non-GIM/FM: combined data for IM, ND, DC, and TCM.
–, standard deviation unable to be calculated because only 1 HHQ included in the analysis; NA, no questions included in any HHQ in this clinic type.
Unless otherwise noted, values are percentages.
Statistical analysis
An analysis of variance model was used to compare the average number of components included among the nine medical history components, five well-being components, and two health maintenance procedures components of HHQs among all clinic types. Appropriate contrasts were constructed for the comparison between two clinic types. Analyses were performed with SAS software, version 9.3 (SAS Institute, Cary, NC). All tests were two sided, and a p-value <0.05 was considered to represent statistical significance.
Results
HHQ sample
Integrative medicine and CAM
The Google search identified a total of 9 community integrative medicine clinics, of which 6 HHQs were obtained by website download (2 did not use an HHQ and 1 did not respond to the authors' request), and 5 academic integrative medicine clinics, of which all used HHQs (4 were obtained by website download and one by email correspondence). A total of 16 CAM clinics were identified, including 6 naturopathic medicine clinics, of which 5 HHQs were obtained by website download (1 did not respond to the authors' request); 8 chiropractic clinics, of which 4 HHQs were obtained by website download (two did not respond to the authors' request and 3 were using the same HHQ, which were treated as 1); and 7 TCM clinics, of which all used HHQs that were obtained by website download.
GIM/FM
The first clinic search strategy identified a total of 15 GIM/FM clinics in the western LA county area, and 9 HHQs were obtained (8 GIM and 1 FM). The clinics identified included 5 academic university medical center clinics (1 GIM residency teaching clinic, 1 FM residency teaching clinic, and 3 satellite/community GIM practices; all used HHQs and were obtained by website download), 1 Veterans Affairs hospital–based GIM clinic (paper HHQ provided to authors), 1 large private health system GIM residency teaching clinic (paper HHQ provided to authors), 2 low-income public teaching clinics (1 each of GIM and FM; neither used an HHQ according to clinic staff), 4 private community-based GIM clinics (2 obtained by website download, and 2 did not use a HHQ), and 2 managed care hospital–based clinics (1 each of GIM and FM; neither used an HHQ according to clinic staff). The second clinic search strategy identified 3 county hospital–based clinics (2 GIM and 1 FM; none used an HHQ according to clinic staff).
Medical history
In HHQs of GIM/FM clinics, the average number of medical history components was 6.4 (standard deviation [SD], 1.9) compared with 8.3 (SD, 1.2) for integrative medicine (p = 0.01), 9.0 (SD, 0) for naturopathic medicine (p = 0.01), 7.1 (SD, 2.8) for chiropractic (p = 0.58), and 7.1 (SD, 1.7) for TCM (p = 0.41) (Fig. 6).
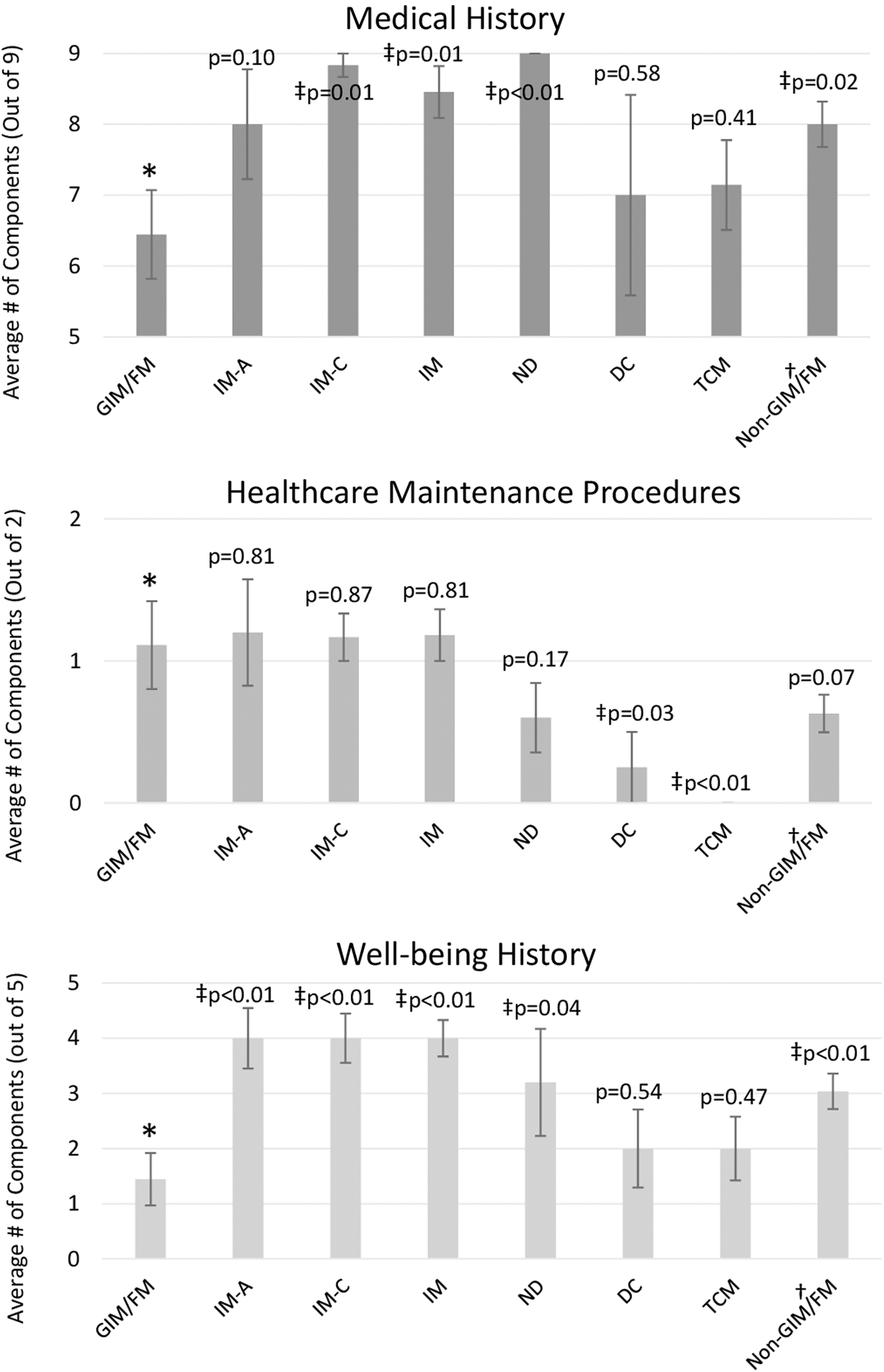
Average number of components included for each type of clinic health history questionnaire. Error bars presented as standard error of the mean. *General internal & family medicine (GIM/FM) comparison group. †Non-GIM/FM, combined data for integrative medicine (IM) (IM-academic [A] and IM-community [C]), naturopathic medicine [ND], chiropractic medicine [DC], and Traditional Chinese Medicine [TCM]). ‡Statistically significant at p < 0.05.
Health maintenance procedure history
No practice type consistently included both health maintenance procedures (immunizations and screenings). In HHQs of GIM/FM clinics, the average number of health maintenance procedure components was 1.1 (SD, 0.9) compared with 1.2 (SD, 0.6) for integrative medicine (p = 0.81), 0.6 (SD, 0.6) for naturopathic medicine (p = 0.17), 0.25 (SD, 0.25) for chiropractic (p = 0.03), and 0 (SD, 0) for TCM (p < 0.01) (Fig. 6).
Well-being history
In HHQs of GIM/FM clinics, the average number of well-being components was 1.4 (SD, 1.4) compared with 4.0 (SD, 1.1) for integrative medicine (p < 0.01), 3.2 (SD, 2.1) for naturopathic medicine (p = 0.04), 2.0 (SD, 1.4) for chiropractic (p = 0.54), and 2.0 (SD, 1.5) for TCM (p = 0.47) (Fig. 6).
Medical history and health maintenance procedure: subgroup analysis
In HHQs of GIM/FM clinics, a chief complaint or main reason for the visit was included only 44% of the time compared with 100% in all other clinic types (p = 0.02). HHQs of all clinic types included questions on past medical history, surgical history, social history, allergies, medications in 75% or more of HHQs. HHQs of GIM/FM clinics included a review of systems 67% of the time compared with 93% for all non-GIM/FM clinics (combined data for integrative, naturopathic, and chiropractic medicine and TCM).
In HHQs of GIM/FM clinics, 67% included a question on immunization history compared with 22% in all non-GIM/FM clinics. HHQs of chiropractic and TCM clinics were the least likely to include questions on immunizations and screenings. HHQs of integrative medicine clinics more frequently included a question on screening history compared with other clinic types (82% inclusion versus ≤44% for all other clinic types) (Table 1).
Well-being subgroup analysis
HHQs of integrative and naturopathic medicine clinics more frequently included questions on diet, exercise, stress, and sleep compared with all other clinic type HHQs. HHQs of GIM/FM clinics were the least likely to include diet, exercise, stress, and sleep questions compared with all non-GIM/FM clinic types. HHQs of chiropractic and TCM clinics variably included well-being components and did not include questions on spirituality (Table 1).
Average pages
In HHQs of GIM/FM clinics, the average page length was 3.3 (SD, 3.4) compared with 7.1 (SD, 5.1) for integrative medicine (academic, 7.8 [SD, 7.9]; community, 6.7 [SD, 3.2]), 5.4 for naturopathic medicine (SD, 2.4), 4.0 (SD, 2.0) for chiropractic, and 3.6 (SD, 1.6) for TCM; none differed significantly from GIM/FM HHQs.
Number of questions for specific components
The average number of review of systems questions per HHQ ranged from 43 in chiropractic to 143 in community integrative medicine. Compared with HHQs of GIM/FM clinics, the HHQs of all non-GIM/FM combined included about twice the average number of review of system questions. HHQs of community integrative medicine clinics included the most questions on nutrition, including on average 18.3 (SD, 25.2). Only 1 GIM/FM clinics' HHQ included questions on nutrition (8 items). HHQs of integrative and naturopathic medicine clinics included the most questions per HHQ on exercise, stress, and sleep compared with other clinic types (Table 2).
Medication and social history: prevalence of specific components
HHQs from all clinic types varied greatly in the average inclusion of specific questions regarding vitamins, supplements, and herbs/botanical use, yet GIM/FM clinics included them the least frequently: in only 11%–22% of HHQs (Table 3). The most consistently included social history questions for all clinic types was tobacco and alcohol use (Supplementary Table S1).
Unique HHQ components
A variety of unique question components were included in the different clinic types. In HHQs of integrative medicine clinics, 42% included a series of questions exploring prior use of CAM therapies (Fig. 1; Supplementary Table S2). The HHQs of naturopathic and integrative medicine, 40% and 9%, respectively, included a “wheel of balance” assessment that explores patient's subjective well-being (family/friends, career, money, health, partnership, fun/recreation, personal growth, physical environment; Fig. 2, Supplementary Table S2). A body map that allows patients to draw the location of their pain was included in 75% of chiropractic, 71% of TCM, and 27% of integrative medicine HHQs (Fig. 3, Supplementary Table S2). HHQs of integrative, naturopathic, and TCM clinics frequently included questions on environmental and food allergies and a 24-hour food intake recall tool (Supplementary Table S2).
Discussion
This is the first study, to the authors' knowledge, that examined the content of health history questionnaires used in practice at GIM/FM, integrative medicine, naturopathic medicine, chiropractic, and TCM clinics.
Integrative and naturopathic medicine HHQs included significantly more well-being components than GIM/FM HHQs, in line with the study hypothesis. In particular, integrative and naturopathic medicine HHQs included more questions per HHQ evaluating a patient's holistic health. Integrative and naturopathic medicine HHQs often included questions on health-promoting behaviors (quality of diet, exercise, stress, sleep), personal history (extended social history beyond just substance use) and use of nonprescription medication (vitamins, supplements, and herbal/botanical products) compared with all other clinic types. Integrative and naturopathic medicine HHQs were longer in average page length and likely had more page space to include more extensive questioning compared with other clinic types.
Contrary to the study hypothesis, GIM/FM HHQs included fewer medical history components than all non-GIM/FM combined HHQs, except the medication use component. Medical history components were the most consistently included questions for all HHQs in the study, with regular inclusion of past medical history, surgical history, social history, allergies, and medications. No clinic type consistently asked about both prior health maintenance screenings and immunizations. Despite the common practice of reviewing health screenings and immunizations at a GIM/FM annual physical, these were included in only 44% and 67% of HHQs, respectively. Integrative medicine and GIM/FM HHQs most frequently included health maintenance procedure questions compared with other clinic types, which fits with actual practice because both integrative medicine and GIM/FM are practiced by mainly MD/DO practitioners, who are trained and likely have access to delivery of these services.
Chiropractic and TCM HHQs were shorter and included more limited, problem-focused content. For example, chiropractic HHQs often asked questions relating to disability and acute/chronic pain, which are common to musculoskeletal conditions often addressed by chiropractors. The treatment nature of chiropractic and TCM clinics, focused on chiropractic manipulation and acupuncture, respectively, may explain the less extensive questions about general health behaviors and healthcare maintenance. For example, two of seven TCM clinic HHQs included a series of questions about diseases and symptoms that could potentially increase the risks of acupuncture and herbal treatments (Fig. 6).
Overall, academic and community integrative medicine HHQs included similar question components. One notable difference was the inclusion of questions relating to toxin exposures (e.g., heavy metals) in two thirds of community versus none of academic integrative medicine HHQs (Supplementary Table S2). Some of these nonacademic clinics offered regimens for chelation (a controversial alternative treatment, outside of documented high-level exposures, that is typically not covered by insurance) and thus likely explains their inclusion of this questioning.
Even within clinic types there was significant variability in question areas and the number of questions included beyond the common medical history component questions. This variability may reflect individual clinic customization based on its unique population needs or a lack of uniformity within clinic types as to the minimum pre-visit information needed from specific visit types.
Future work and challenges
Attempts to create a more standardized HHQ aligning question priorities among various mainstream and CAM providers have been challenging. One study, using a Delphi survey technique, attempted to develop a standardized HHQ to be used by medical doctors, naturopaths, chiropractors, and licensed acupuncturists. They noted significant difficulty in reconciling the different underlying philosophies of health and disease from CAM clinic representatives with western biomedicine terminology. 26 This study found that nearly half of HHQs of TCM clinics include a TCM-specific review of systems that reflects the underlying traditional theories that differs substantially from mainstream western biomedicine (Supplementary Table S2, Fig. 4). A one-size-fits-all approach may not be the ideal way to proceed with HHQ development.
It would be helpful to create clear guidelines to include basic questions for a new patient visit versus a return visit, depending on the priorities of a clinic type. For example, a GIM/FM new patient visit HHQ may benefit from including more well-being components that are in line with national priorities for improved nutrition, exercise, and stress management of patients. 27 Each clinic has its own unique population and needs, and customizability of HHQs for specific goals should be encouraged. HHQ development efforts may benefit from exploring innovative question content, formatting, and layout that engages patients and elicits patient's unique health journeys, such as the examples in Supplementary Table S2 and Figures 1 –3.
Study limitations
The study examined a small number of clinics, by clinic type. The sampling strategy likely represents the range of such clinics serving the population in the western region of Los Angeles County and similar areas of California, but the generalizability to other areas is unclear. The HHQs were obtained primarily through online sources and may favor newer or electronically savvy clinics that would have a website to upload their forms. The HHQs do not account for questions asked verbally by a rooming medical assistant or checklists entered into an electronic medical record (e.g., chief complaint or immunization history), and this may have affected the accuracy of the GIM/FM HHQ data.
Conclusion
HHQ content varies considerably within and across clinic types. Integrative and naturopathic medicine HHQs included significantly more well-being components than GIM/FM HHQs. Surprisingly, GIM/FM HHQs included fewer medical history components than all non-GIM/FM practice types. No clinic types consistently asked about prior health maintenance screenings and immunizations. Further investigation is warranted to determine the optimal HHQ content to support the clinical and preventive health goals of GIM/FM, integrative medicine, and CAM practices.
Footnotes
Acknowledgments
The authors thank Chi-Hong Tseng, PhD, UCLA Department of Medicine Statistics Core, for his expert assistance in providing further statistical analysis for this manuscript.
Preliminary data and analysis were presented as a poster May 13–16, 2014, at the International Research Congress on Integrative Medicine and Health in Miami, Florida, USA. The poster abstract was subsequently published in JACM (Laube J, Shapiro M. J Altern Complement Med 2014;20:A117.).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.