
Abstract
Background:
Xerostomia is one of the most common complaints in maintenance hemodialysis (MHD) patients. This problem contributes to excess fluid intake and results in poor survival outcome. Based on Traditional Chinese Medicine (TCM) theory and literature studies, the authors have been practicing auricular acupressure therapy (AAT) to help patients with xerostomia. This pilot study was conducted to demonstrate the potential of AAT for xerostomia in MHD patients.
Methods:
Eligible subjects who agreed to participate in this study were recruited and provided with AAT for 4 weeks. The Summated Xerostomia Inventory (SXI), as well as measurement of inter-dialytic weight gain (IDWG), daily inter-dialytic weight gain (daily IDWG), percentage of inter-dialytic weight gain (IDWG%), blood pressure, and biochemical parameters, were completed at baseline and after a 4-week intervention.
Results:
A total of 26 eligible participants were recruited. Of them, 10 men and 16 women (M age = 52.92 ± 11.80 years; dialysis vintage 81.86 ± 46.05 months) completed the study. After the 4-week AAT intervention, the SXI scores were significantly decreased compared with baseline (from 10.08 ± 2.26 to 9.04 ± 2.14; p < 0.05). However, the IDWG, daily IDWG, IDWG%, blood pressure, and biochemical parameters did not change significantly after the intervention.
Conclusion:
This study provides preliminary evidence that AAT may be effective in reducing xerostomia intensity for MHD patients.
Introduction
X
It is expected that MHD patients would have better fluid control if their xerostomia symptom improved. However, studies on xerostomia management are limited. Acupuncture has been proved to alleviate radiation-induced xerostomia symptoms significantly. 7 –9 Yang et al. demonstrated the potential of acupressure in reducing thirst intensity. 10 These findings imply that non-drug therapies based on the meridian theory of Traditional Chinese Medicine (TCM) might play a role in alleviating xerostomia for MHD patients.
Auricular acupressure is a therapeutic method, stimulating certain acupuncture points on the ears in order to manage multiple diseases. Stimulation is produced by pressing specific points with embedded beads, usually Semen vaccariae (wang bu liu xing) seeds or stainless steel beads. Compared with acupuncture, it is noninvasive and can be self-manipulated at home. It has been used for diverse complications, such as uremic pruritus, sleep disorder, and impaired quality of life in MHD patients. 11 –13 Based on TCM meridian theory, specific points on the auricles correspond to major organs or systems of the body, and therapeutic effects can be achieved by stimulating auricular points. Auricular acupressure therapy (AAT) has been practiced to manage a variety of discomforts such as sleep disorder, pain, and dry mouth in TCM clinics. If a proper AAT protocol is developed to alleviate xerostomia effectively for dialysis patients, they might restrict their fluid intake and control their IDWG better than they did before. Thus, this intervention study was conducted to demonstrate the potential of AAT for MHD patients with xerostomia and to lay the necessary foundations for further randomized control trials.
Methods
Participants and setting
The MHD patients were recruited from Guangdong Provincial Hospital of Chinese Medicine, China. The inclusion criteria included: aged ≥18 years and on regular hemodialysis for at least 3 months; IDWG ≥1 kg at the beginning of the study; and agreed to participate in the study. Those with acute cardiovascular event, acute infection, poor control of diabetes mellitus, psychiatric disorders, allergy to S. vaccariae seed, and a malformed ear were excluded.
Intervention
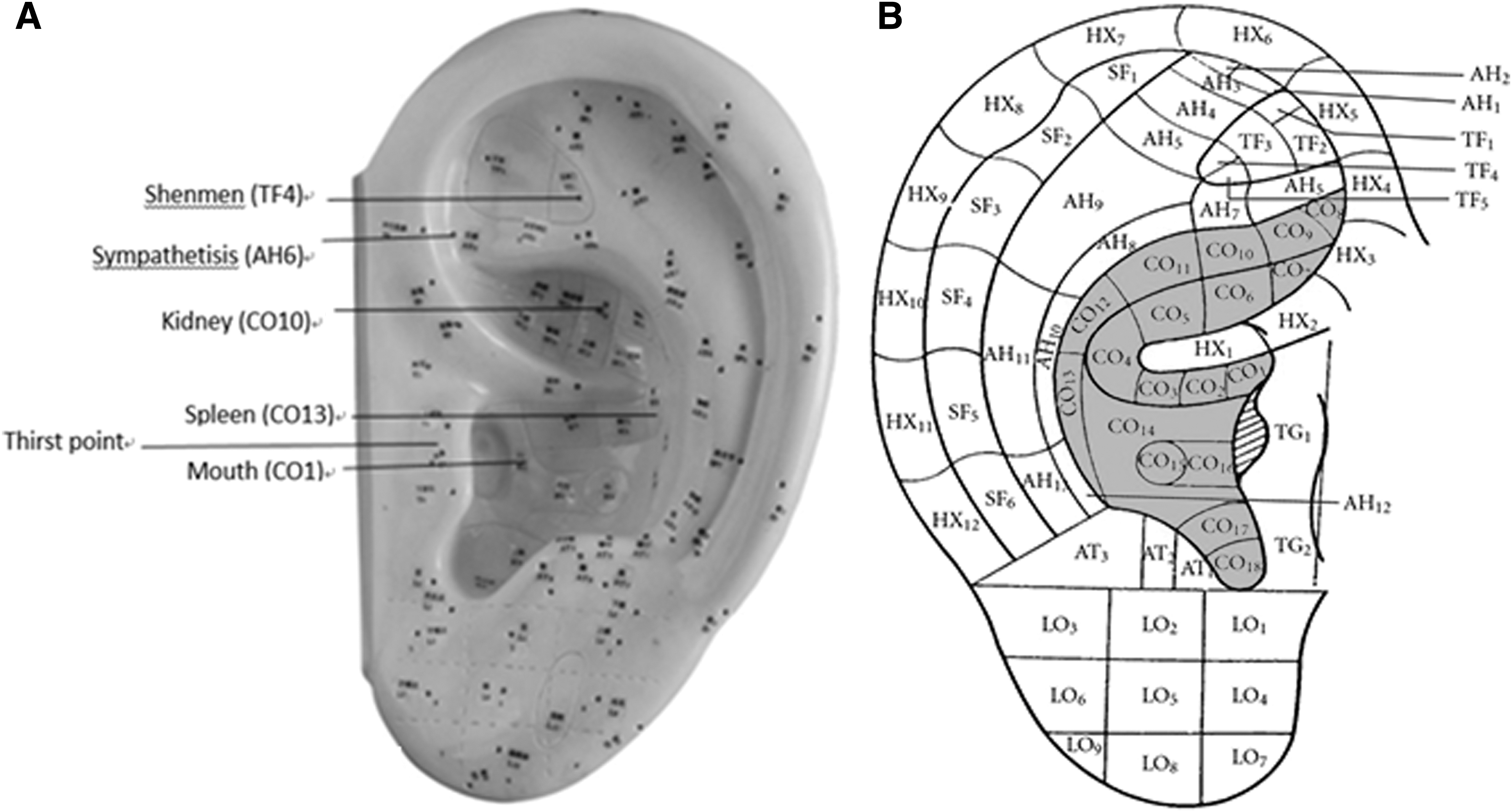
The study was a prospective interventional pilot study. All the patients received AAT on six acupoints: Shenmen (TF4), Sympathetisis (AH6), Kidney (CO10), Spleen (CO13), Mouth (CO1), and Thirst point, as indicated in Figure 1A. The treatment duration was 4 weeks. The Summated Xerostomia Inventory (SXI), an instrument for assessing the intensity of xerostomia, was completed at baseline and after a 4-week intervention.
(
Acupoint selection
Auricular points chosen were based on TCM meridian theory, results of a literature review, and clinical practice experience. In TCM theory, both the Spleen and Kidney are in charge of normal distribution of body fluid and saliva secretion. Patients with Spleen-yin or Kidney-yin insufficiency syndrome usually present with a dry mouth. The acupoints of Kidney (CO10), Spleen (CO13), Shenmen (TH4), Sympathetisis (AH6), and Mouth (CO1) are located at the triangular fossa, where the auricular branch of the vagus nerve and the auriculotemporal nerve distribute. These nerves play an important role in activating the parasympathetic nervous system, which may increase the amount of saliva flow. 14 –16 The thirst point is an extra point based on acupuncturists' experience in treating xerostomia. The auricular point selection protocol has been confirmed by two experienced acupuncturists.
Auricular acupoint identification
In accordance with the national standards of the nomenclature and location of auricular acupoints published in China, 17 the auricular acupoints chosen were as follows: Shenmen (TF4), at the apex of the triangular fossa, in the bifurcating point between the superior and inferior crura of the antihelix; Sympathetisis (AH6), at the end of the inferior antihelix crus; Kidney (CO10), on the posterior portion of the concha inferior to the inferior crus of the helix; Spleen (CO13), on the posterior and superior portion of the inferior or concha, inferior to the BD line; Mouth (CO1), on the anterior one-third of the concha, under the inferior crus of the antihelix; and the Thirst point, slightly superior to the midpoint between the apex of the tragus and the point of the external nose.
To help researchers recognize the location of acupoints accurately, an ear model with a map of acupoints was provided (Fig. 1B).
Standard operation procedure for AAT
Two practitioners were well trained concerning the trial's procedure and had their competency assessed by a senior acupuncturist before the intervention. AAT was performed when patients were receiving hemodialysis in a relaxed state. Each point was disinfected with 75% ethanol before manipulation. Thereafter, an adhesive plaster (1 cm × 1 cm) with one bead (S. vaccariae, globes approximately 2.0 mm in diameter; surface: smooth; color: black) was imbedded. The beads were pressed with an appropriate strength of 0.3–0.4 kg until a slight soreness was felt on the points for about 5 min on each point. Participants were instructed to press the beads three times a day. Both ears were used alternately to avoid skin lesions caused by long-term adhesion. The participants were visited two or three times a week when they came for hemodialysis treatment. During that time, their adhesive patch was renewed, and they were assessed for their compliance. The manipulation instructions for participants were also repeated in order to enhance the consistency of the pressure.
Outcome measurements
The intensity of xerostomia was measured by the SXI. The SXI consists of five items. Each item has a five-point Likert-scale and three-response format (1 = “never,” 2 = “hardly ever and occasionally,” and 3 = “frequently and always”). Therefore, the SXI score for each patient ranged from 5 (no xerostomia) to 15 (extreme xerostomia). The Chinese version of the SXI has been tested for its applicability. 18 The SXI score was evaluated at baseline and after a 4-week intervention. In addition, demographic characteristics and clinical data were collected from patient files, such as age, sex, blood pressure (BP), dialysis vintage, pre-dialysis weight, post-dialysis weight, dry weight, primary disease of end-stage renal disease (ESRD), and biochemical parameters. BP was performed on patients after being recumbent for 10 min in the arm without arteriovenous fistula. IDWG is defined as the difference between pre- and post-dialysis weight, and it was collected at the midweek dialysis session. On this basis, the ratio of the IDWG to the patient's dry weight is defined as IDWG%, and the ratio of IDWG to inter-dialytic phase is daily IDWG. All of these data were collected at baseline and after a 4-week intervention.
Statistical analysis
All data were analyzed by IBM SPSS Statistics for Windows v19 (IBM Corp., Armonk, NY). The data are presented as mean ± standard deviation, median (interquartile range), frequencies, or percentages, as appropriate. A two-sided paired Student's t-test was applied to test for normally distributed variables. Wilcoxon's signed-rank test was applied to test for non-normal distributions. Pearson's chi-square test was applied for nonparametric variables. p-Values of <0.05 were considered statistically significant.
Ethics
This study was approved by the Ethics Committees of Guangdong Provincial Hospital of Chinese Medicine Research, with registration number B2015-052-01.
Results
Participant recruitment
The MHD patients were recruited from Guangdong Provincial Hospital of Chinese Medicine during June 2015. Recruitment was conducted via hospital postings in the hemodialysis unit. A total of 135 patients underwent the initial screening. Of these, 65 had a daily IDWG >1 kg and were invited to participate in the study. Forty patients gave their consent, but 14 were excluded for infections (n = 5), acute heart failure (n = 3) and hospitalization for other events (n = 6). Finally, 26 MHD patients were enrolled and underwent 4 weeks of AAT.
Participant characteristics
Twenty-six MHD patients agreed to participate in this study. Their mean age was 52.92 ± 11.8 years. The mean dialysis vintage was 81.86 ± 46.05 months. The primary diseases of ESRD were chronic glomerulonephritis, hypertension, diabetes, and nephrotic syndrome. The patients' demographic characteristics and clinical data were comparable, as shown in Table 1.
Data are presented as mean ± standard deviation or frequencies (percentages).
ESRD, end-stage renal disease; Kt/V, urea clearance index.
Primary outcome
Table 2 shows the results of the SXI before and after a 4-week AAT intervention. After the 4-week intervention, the SXI scores significantly decreased compared with baseline (from 10.08 ± 2.26 to 9.04 ± 2.14; p < 0.05). Patients reported reduced scores of oral dryness (p < 0.05), less difficulty in eating dry foods (p < 0.05), and difficulty in swallowing certain foods (p < 0.05). However, the symptoms of dry lips and dryness when eating a meal did not change significantly (p > 0.05). According to the survey, after the 4-week AAT intervention, a shift from experiencing a dry mouth from more frequently to less frequently was revealed (Fig. 2A). Moreover, six patients stopped complaining of feeling a dry mouth compared with none at the beginning. Likewise, the number of patients who frequently or always had difficulty eating dry food apparently decreased after the AAT intervention (Fig. 2B). Paradoxically, more patients complained of their mouth feeling dry when eating a meal, although it did not change significantly (from 4 to 12; Fig. 2C). After the 4-week AAT intervention, the problem of swallowing certain food also decreased (Fig. 2D). The composition of different frequencies of having dry lips did not seem to change (Fig. 2E). However, the data failed to show any significance.

(
Values are expressed as mean ± standard deviation or median (interquartile range).
Two-sided paired Student's t-test.
Wilcoxon's signed-rank test was used because data were not normally distributed.
AAT, auricular acupressure therapy; SXI, Summated Xerostomia Inventory.
Secondary outcomes
The IDWG, daily IDWG, and IDWG% did not change significantly after the 4-week intervention (Table 3). Likewise, systolic blood pressure (from 134.2 ± 28.9 mmHg to 137.1 ± 27.3 mmHg; p > 0.05) and diastolic blood pressure (from 79.46 ± 14.35 mmHg to 80.15 ± 15.35 mmHg; p > 0.05) did not change significantly either (Table 3).
Values are expressed as mean ± standard deviation or median (interquartile range).
Two-sided paired Student's t-test.
Wilcoxon's signed-rank test was used because data were not normally distributed.
IDWG, inter-dialytic weight gain; daily IDWG, daily inter-dialytic weight gain; IDWG%, percentage of IDWG; SBP, systolic blood pressure; DBP, diastolic blood pressure.
The biochemical parameters were shown in Table 4. Serum creatinine, urea nitrogen, calcium, phosphorus, albumin, potassium, and calcium phosphorus product (Ca × Pi) did not change significantly after the 4-week intervention (p > 0.05). However, there was an increase in serum sodium (p < 0.05).
Two-sided paired Student's t-test.
Safety
Compared with acupuncture, AAT is noninvasive and relatively safe. No side effects related to AAT were reported by participants in this study except for mild discomfort or pain.
Discussion
Xerostomia is a highly prevalent accompanied condition that prevents dialysis patients from restricting their fluid intake. Clinicians have been pursuing effective and safe therapeutic measures to alleviate xerostomia symptoms in MHD patients, thereby further restricting their water intake. Nevertheless, the problem remains unresolved. Thus, AAT was performed for dialysis patients in order to help relieve xerostomia and to reduce their inter-dialytic water intake further. An encouraging response was obtained in this pilot study. It was found that a 4-week AAT on the acupoints Shenmen, Sympathetisis, Kidney, Spleen, Mouth, and Thirst reduced patients' self-reported SXI scores, as well as the number of patients suffering from extreme xerostomia. It was confirmed that as a non-invasive therapy based on TCM meridian theory, AAT could play a role similar to that of acupuncture for xerostomia. 8,9,19,20
The findings suggest that AAT might have potential in alleviating xerostomia. However, this effect did not show subsequent benefit for fluid intake restriction of patients. It was assumed that the treatment duration was relatively short for the patients to change their habitual water intake. 21 Another possible reason was that the change of body weight could not reflect the exact change of their fluid intake. Additionally, pre-dialysis serum sodium concentrations were found to be elevated after the intervention compared with those at baseline. This implied that the total water body fluid might be reduced in the condition that the patients maintained their routine sodium intake. In other words, patients might drink less water when their symptom of xerostomia improved. Some objective measurements such as diet diary and body composition measurement, if possible, might help clarify this issue. As a pilot observational study, these findings have provided important implications for both clinical and research work.
The mechanism of AAT on xerostomia in MHD patients has not been fully studied. It was postulated that AAT might activate the areas of the brain correlated with the amount of saliva flow, just as acupuncture does. 22,23 Auricular acupoints were found to be connected to modulation of the vagus nerve. The autonomic and central nervous systems could be modified by auricular vagus stimulation via projections from the auricular branch of the vagus nerve to the nucleus of the solitary tract, which may influence the amount of saliva flow. 15,16,24 Further studies should involve measurement of the amount of saliva flow and vagus nerve activity in order to investigate the underlying relationship.
A decreased amount of saliva flow was common in dialysis patients, leading to symptoms of xerostomia or thirst and excessive intake of water. 25 Solitary dietary education often failed to refrain these patients from drinking excessive water. The saliva substitutes or stimulation of salivary glands by mechanical means that included angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, pilocarpine, or chewing gum failed to reduce the xerostomia due to ineffectiveness or side effects. 21,26 –28 The present study showed that AAT could be a complementary treatment for dialysis patients to manage their xerostomia. The emphasis has been on symptom management for dialysis patients to improve their compliance with health caregivers. With proper protocol modification and a longer duration of treatment, some inspiring outcomes such as improvement of quality of life, better control of blood pressure, and less cardiovascular events could be reasonably expected.
There were several limitations to this study. First, the sample size was small, and the follow-up was short. Moreover, as a pilot study, it lacked a control group and randomization, which weakened the results of the study. However, this pilot study demonstrated the potential effect of AAT on alleviating the symptom of xerostomia. Further research with larger sample sizes, a control group, and longer follow-up should now be conducted.
Conclusion
In summary, AAT has the potential to alleviate xerostomia for MHD patients and could be applied as a complementary treatment. Further studies are required.
Footnotes
Acknowledgments
This work was a part of a research project funded by the Guangdong Administration of Traditional Chinese Medicine (no. 2014807) and supported by State Administration of Traditional Chinese Medicine (no. 2012KT1301), Research Project for Practice Development of National TCM Clinical Research Bases, China.
Author Disclosure Statement
No competing financial interests exist.