
Abstract
Objectives:
Research demonstrates the benefits of complementary and alternative medicine (CAM) in myriad environments. Yet, the majority of CAM services are offered in outpatient settings. Incorporating CAM into hospital settings may lead to increased patient comfort, well-being, and overall satisfaction with hospital admissions. Few studies have examined CAM services among inpatients. Therefore, this study assessed inpatients' preferences and beliefs regarding CAM, as well as their stated willingness to pay for these services.
Design:
Adult patients (n = 100), ranging in age from 19–95 years (M = 53 years; SD = 19.2 years), were recruited during their hospitalization in the University of California, San Diego, Healthcare System. The inpatients completed a brief individual interview to gather their perspectives on common CAM services, including acupuncture, aromatherapy, art therapy, guided imagery, healthy food, humor therapy, massage therapy, music therapy, pet therapy, Reiki, and stress management. Inpatients were asked which CAM therapies they perceived as being potentially the most helpful, their willingness to pay for those therapies, and their perceived beliefs regarding the use of those therapies.
Results:
Inpatients most commonly perceived healthy food (85%), massage therapy (82%), and humor therapy (70%) to be the most helpful, and were most willing to pay for healthy food (71%), massage therapy (70%), and stress management (48%). Inpatients most commonly believed CAM treatments would provide relaxation (88%), increase well-being (86%), and increase their overall satisfaction with the hospitalization (85%).
Conclusions:
This study suggests that CAM services may be a beneficial addition to hospitals, as demonstrated by inpatients' interest and stated willingness to pay for these services. These findings may help organizational leaders when making choices regarding the development of CAM services within hospitals, particularly since a significant percentage of inpatients reported that CAM services would increase their overall satisfaction with the hospitalization. These results merit further attention given the need to increase cost savings while enhancing the overall patient experience in today's medical marketplace.
Introduction
C
Food/nutrition, supplements, yoga, meditation, Traditional Chinese Medicine/acupuncture, and massage are some of the most widely used CAM therapies in the United States. 4 Currently, 63% of individuals self-refer for CAM services in the medical setting and primarily receive services in an outpatient setting for preventive care and treatment of chronic ailments. 5 Many outpatient services such as acupuncture, massage therapy, meditation classes, and mind–body therapies are most often paid for by patients themselves rather than from insurance. 4 The demonstrated health benefits of outpatient CAM services, coupled with patients' interest in paying for those services, has increased national attention regarding the successful provision of CAM in hospital settings. 5
Approximately 52% of the 29 large primary-care centers affiliated with a hospital, healthcare system, medical, and/or nursing school sampled in the 2012 Bravewell report offered inpatient CAM services. 4 When available, common complementary and alternative treatment offerings for patients while they are in the hospital include: acupressure, aromatherapy, biofeedback, expressive arts, guided imagery, massage therapy, mind–body therapies, mindfulness therapy, music therapy, pet therapy, relaxation therapy, and Reiki/therapeutic touch. 4,5 Hospitals often rely on patient demand, evidence of efficacy, and practitioner availability when choosing what services to implement and must rely on out-of-pocket payment or philanthropic funds to support CAM services in the hospital. 5
A small but growing body of literature suggests there are significant health benefits, such as reductions in anxiety, distress, fatigue, nausea, and pain when patients are given the opportunity to receive CAM services during their hospital stay. 6 –9 St. John's Riverside Hospital in New York reported that when inpatients (n = 122) were offered CAM therapies, the inpatients experienced decreased anxiety (40%), reduced pain (34%), and improved sleep (34%). The inpatients additionally reported finding new ways to cope with their illness (31%). 10
In regards to pain management, the Penny George Institute for Health and Healing in Minnesota reported a 55% reduction in self-reported pain among inpatients (n = 1837) receiving CAM services. The majority of these patients had never received complementary and alternative services prior to admission (66%). The inpatients receiving therapies also had a shorter length of stay in the hospital (average of 3.99 days vs. 4.41 days for all patients at the hospital), although this finding was not statistically significant. 11
Furthermore, studies demonstrate significant cost savings related to complementary and alternative therapies, particularly with oncology inpatients. An optimal healing environment, “Urban Zen” was created in the Beth Israel (New York) inpatient medical oncology unit. This study found the average medication cost was reduced from $889 per inpatient for a 3-day stay to $420 per inpatient (47% reduction in the mean cost of medication), with the most dramatic decreases found in anti-anxiety and anti-nausea medications. 12 These studies show promise for the ability of CAM services to not only minimize inpatients' anxiety and pain, but also to reduce their medication costs.
Although the benefits of providing CAM services to inpatients are increasingly evident, it can be difficult to begin offering such services in hospital settings. Common barriers include prohibitory hospital regulations or policies, a lack of understanding about CAM among practitioners or administrators, and a lack of current insurance reimbursement for such services. 2 Furthermore, there appears to be a lack of knowledge regarding inpatients' preferences for CAM services, and no study to date has specifically examined inpatients' preferences for these services. Are inpatients interested in receiving these services during their hospital stay? If so, how do they believe these services would be helpful, and would they be willing to pay for these services themselves if necessary? The current study aims to address these questions, thereby increasing the understanding of inpatients' perspectives regarding CAM services, and striving to improve the overall landscape of inpatient care and satisfaction.
Materials and Methods
Participants
Participants were recruited from the University of California, San Diego, Healthcare System, Family Medicine Inpatient Service, between November 2013 and August 2014. Inclusion criteria were purposely broad so as to gather a wide array of inpatient preferences: being aged ≥18 years old, currently hospitalized as an inpatient, and the ability to conduct an individualized interview in English. Potential study participants were excluded if there was a current diagnosis of severe dementia, delirium, or other cognitive impairments. The research design, participant recruitment plan, as well as all other facets of the study were reviewed and approved by the Human Research Protections Program and Institutional Review Board at the University of California, San Diego.
Procedure
This cross-sectional study utilized a researcher-derived individual interview to learn about the inpatients' preferences for CAM services. The interview also examined patients' perspectives on how those services could be helpful and whether they would be willing to pay for those services if they were offered in the hospital. Inpatients were informed that these services were not currently offered in the University of California, San Diego, hospital, but that the aim of the study was to learn more about what services, if offered, would be valued by inpatients.
During each interview, the researcher described 11 commonly provided complementary and alternative services: acupuncture, aromatherapy, art therapy, guided imagery, healthy food, humor therapy, massage therapy, music therapy, pet therapy, Reiki, and stress management. 4 The CAM services described in this study were suggested by stakeholders and practitioners during an inpatient needs assessment that was conducted in September 2013 at the University of California, San Diego. Because patients had varying levels of familiarity with each of these services, a brief standardized definition (derived by our interdisciplinary team) and list of services was provided (see Table 1 for a list of the treatment descriptions used). As each service was described, the inpatients were asked, “Do you think [these services] would be helpful to you during your hospital stay?” (yes or no). If yes, the inpatient was asked, “Would you be willing to pay for these services yourself?” (yes or no). Inpatients were also asked to state whether they believed each service could: (1) help them relax, (2) help them recover more quickly, (3) help them cope with being in hospital, (4) decrease their pain, (5) decrease emotional difficulties, (6) increase their sense of well-being, and (7) increase their overall satisfaction with the hospitalization (yes or no). Each interview, lasting an average of 30 min, was conducted at the bedside of the inpatient and was administered by the research team of trained health professionals.
Results
A total of 100 inpatients participated in the study (please see Table 2 for detailed inpatient demographics). The inpatients ranged from 19 to 95 years of age (M = 53 years; SD = 19.2 years). The majority (77%) of inpatients were admitted to the hospital through the emergency room, whereas 19% were admitted as part of a planned visit. The average length of hospital stay was 6 days (SD = 10.0 days; range 1–86 days).
Demographic data were not available for every patient in all categories. Thus, some categories total <100.
Descriptive statistics were completed using IBM SPSS Statistics for Windows v21 (IBM Corp., Armonk, NY). Inpatients most commonly reported that healthy food (85%), massage therapy (82%), and humor therapy (70%) would be helpful during their hospital stay. Additionally, inpatients indicated they would be most willing to pay for healthy food (71%), massage therapy (70%), and stress management (48%). Figure 1 lists the percentage of inpatients' who stated the complementary and alternative treatments or services would be helpful, and the percentage of inpatients who stated they would be willing to pay for these services.
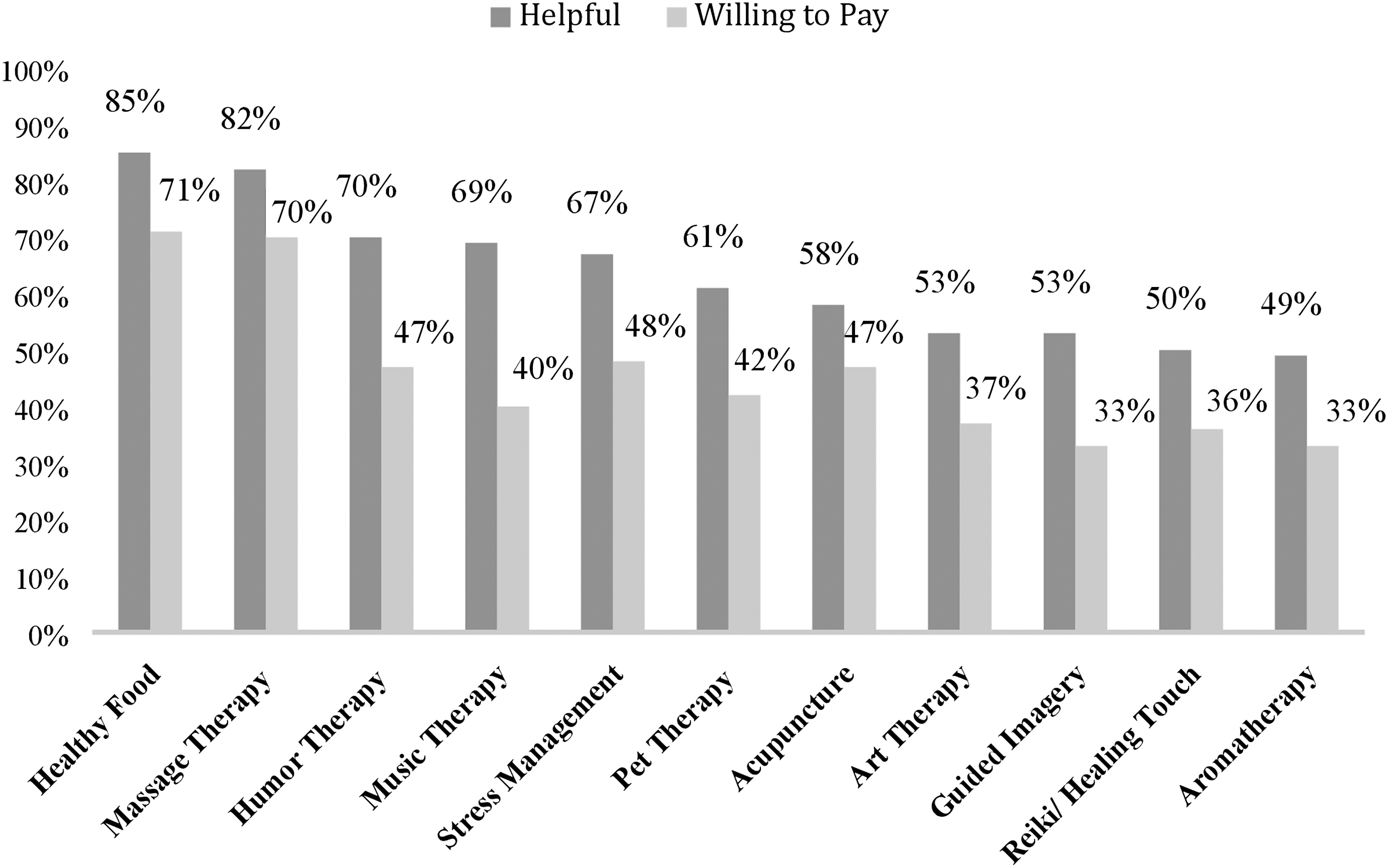
Helpfulness of complementary and alternative medicine services and willingness to pay for services, as reported by inpatients (n = 100).
Figure 2 presents the ways in which inpatients believed CAM services would be of benefit, with the majority of patients indicating that complementary and alternative services could help them relax (88%), increase their well-being (86%), and increase their overall satisfaction with the hospitalization (85%).
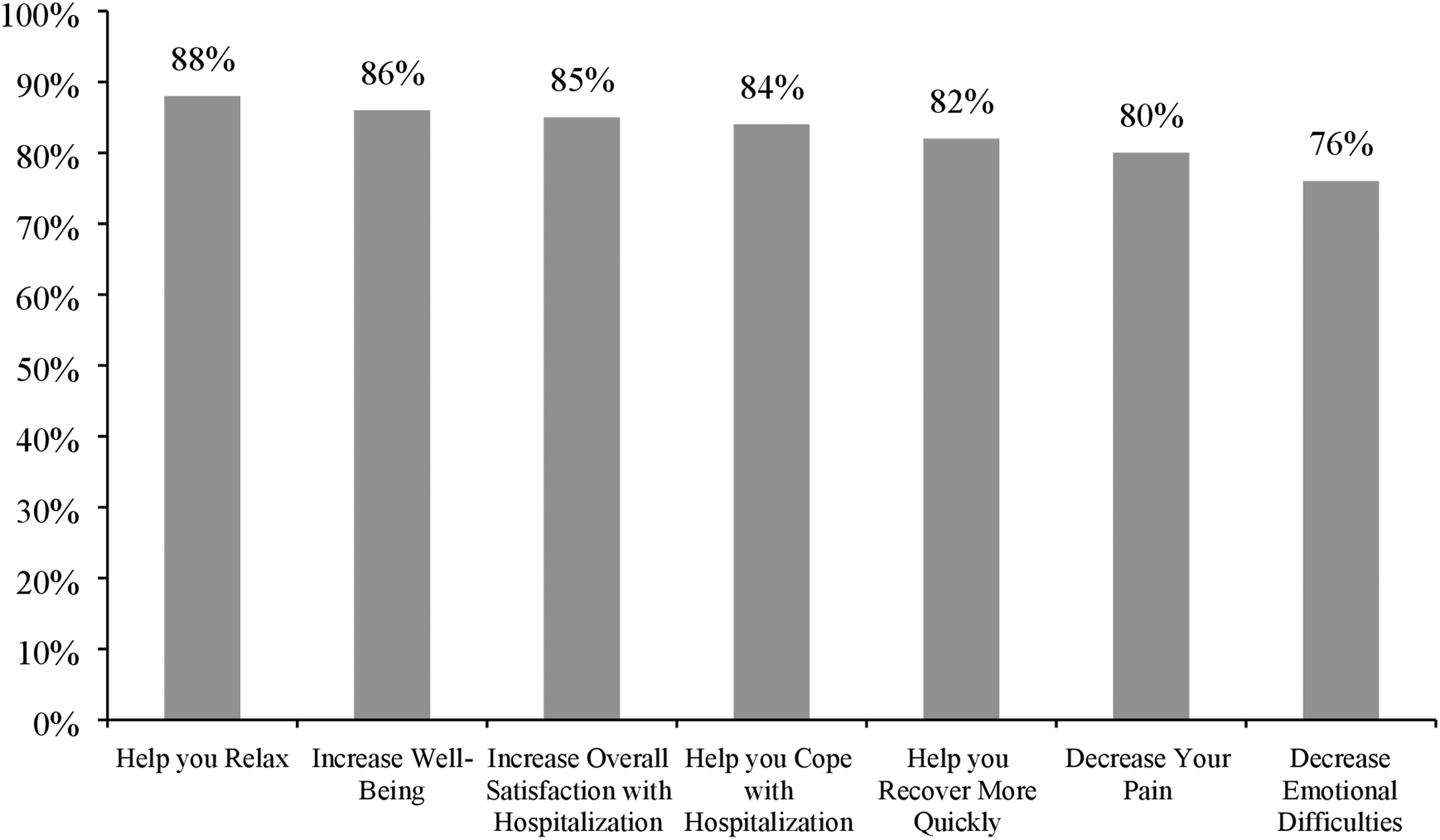
Ways in which inpatients believe complementary and alternative medicine services are beneficial (n = 100).
Discussion
Summary
To the authors' knowledge, this is the only study to date that has examined inpatients' preferences, beliefs, and willingness to pay for CAM services. The findings suggest that inpatients are interested in CAM services as part of their hospital stay and believe these services would be of benefit. Specifically, inpatients reported the highest preferences for the incorporation of healthy foods, massage therapy, and humor therapy. Inpatients most commonly indicated that CAM services could help them relax, increase their well-being, and improve their recovery. Inpatients also viewed CAM services as being able to help them cope with their hospitalization, and felt that they could increase their overall satisfaction with the hospitalization. All of these self-reported inpatient beliefs suggest a strong interest in CAM services being provided within hospitals.
While many of the inpatients in this study indicated an interest in CAM services, health literacy may play an important role when assessing interest or implementation of complementary and alternative services among inpatients. Inadequate health literacy affects 36% of Americans and is more prevalent among minority groups. 13 A recent study examining CAM usage among inpatients found that those with a higher health literacy utilized services more often than those with a lower health literacy. 14 Therefore, in order for CAM services to be of benefit and utilized in hospitals, it is important that inpatients are educated regarding CAM treatments and that the modalities are tailored and designed for those who may have a lower health literacy in order to ensure successful implementation of services.
A significant number of inpatients reported that having a CAM service would increase their overall satisfaction with the hospitalization experience. Given the growing need for hospital systems to improve inpatient satisfaction for a range of reasons, including shorter hospital stays, increased cost savings, fewer potential lawsuits, and enhanced competiveness in the medical system marketplace, this finding merits further study. 15,16
Limitations
Although beneficial to hear about inpatients' preferences and beliefs regarding CAM services, there were several limitations when interpreting the results of this study. First, this study utilized a convenience sample of inpatients in one southern California hospital, and the relevance of these findings in other geographic regions is unclear. Also, although inpatients reported they would be willing to pay for services, the services were not currently being offered in the hospital. Thus, it is unclear if the inpatients would actually submit payment when called upon for services, and whether it would be feasible to charge a separate fee for CAM services while in the hospital. Additionally, it is unclear how much the inpatients would be willing to pay for each service, as a dollar amount regarding the price of the services was not indicated when the services were described to inpatients in the study.
Conclusions
There is a dearth of literature currently available regarding inpatients' preferences for CAM and the successful implementation of those services. While various studies have examined the effects of CAM therapies on specific symptoms such as anxiety, nausea, pain, and relaxation, 6 –9,17 to the authors' knowledge, no studies have examined inpatients' beliefs and preferences for CAM services and their related patient satisfaction. Furthermore, while inpatients in the present study expressed that CAM services may lead to improvement in their overall satisfaction with hospitalization, little to no research has been able to determine a causal relationship between service provision and improved patient satisfaction. 18 The preference ratings for CAM services reported in this study could help guide hospital administrators when deciding how to implement new inpatient programs. Future qualitative studies could examine how CAM services enhance hospital satisfaction and why inpatients may feel more satisfied when hospitals offer these services. Such data could in turn assist advocates when lobbying insurance companies for coverage of these important services.
Furthermore, it is unclear how CAM services may impact inpatients longitudinally. It may be important to develop CAM hospital programs that allow for the maintenance of these services when patients are discharged to their respective outpatient settings, thereby allowing for even greater continuity of care. Nonetheless, the findings from this study may be valuable to those developing and implementing CAM programs within hospital settings, particularly when aiming to provide services that are perceived to be beneficial by patients and those that may enhance the overall patient experience.
Footnotes
Acknowledgments
The authors wish to thank the University of California, San Diego, Center for Integrative Medicine Executive Team, and the inpatients who graciously participated in this study during their hospital admission. We further acknowledge the additional support of Sabina Rea and Tania Cisneros in preparation of this article. The Westreich Foundation provided funding for this study.
Author Disclosure Statement
No disclosures to report.