
Abstract
Objectives:
To identify the most common referred pain (ReP) pattern of the infraspinatus myofascial trigger point (MTrP) and compare its coincidence with the original ReP pattern, to verify whether there are any significant differences by sex and types of technique and to determine the observed signs and symptoms evoked by deep dry needling (DDN) and manual palpation (MPal).
Design:
A cohort study of patients randomized to two different examination methods (July and August 2016).
Settings:
Students and staff recruited from Miguel Hernandez University (Southeast Spain).
Patients:
One hundred thirty-three participants (70.7% women) with shoulder complaints were randomly assigned to either an MPal (n = 67) or DDN group (n = 66).
Interventions:
The same physiotherapist carried out the techniques on all participants, and the same protocol was followed for both the DDN and MPal groups. The physiotherapist did not ask participants about their pain features or other relevant issues.
Outcome measures:
Local twitch response (LTR) and ReP assessed through a visual analogue scale and features of ReP of the infraspinatus muscle.
Results:
The areas with the highest percentage of ReP were the front (area 3; 27.1%) and back (area 11; 21.1%) of the arm, anterior (area 4; 36.1%) and posterior (area 12; 42.1%) shoulder, and infraspinatus muscle area. DDN proved to be significantly easier than MPal in evoking an LTR (p ≤ 0.001). There were significant differences between sexes in zone 2 (p = 0.041) and no statistically significant differences were found by technique.
Conclusions:
The ReP pattern of the infraspinatus muscle coincides with the original pattern described by Travell and Simons, although the neck area should be questioned. The study found no significant differences in the ReP pattern by sex and when comparing MPal with DDN of MTrP of the infraspinatus muscle. DDN proved to be significantly easier than MPal in evoking an LTR.
Introduction
S
The patient's pattern referred pain (ReP) and tenderness is often the key to identifying the muscle responsible for the myofascial pain syndrome. The original ReP pattern, as described by Travell and Simons in 1999, 7 is characterized as steady, deep, and aching, rarely as burning, and it is reproducible and predictable. 7 However, in clinical practice, ReP patterns are sometimes unclear in the infraspinatus muscle, as some patients feel pain in their fourth and fifth fingers and not in other areas of the upper body such as the neck.
As previous authors explained, 2,8 myofascial trigger points (MTrPs) may offer a complementary explanation for the pathophysiological mechanisms underlying shoulder pain. When the biomechanics of shoulder is abnormal, MTrPs of this region could suffer and be activated. An active MTrP is defined as a hyperirritable nodule of spot tenderness in a palpable taut band of skeletal muscle. 9 –14 The spot exhibits sensitive tenderness on palpation, and proper stimulation can elicit a local twitch response (LTR) that refers pain to a distance specific to each muscle. It also can cause both distant motor and autonomic effects 7,15 –18 and sympathetic hyperactivity. 19 –21 Strong digital pressure on the active MTrP exacerbates the patient's spontaneous pain complaint and simulates the patient's familiar pain experience. In addition, studies have demonstrated biochemical findings that indicate local and remote inflammation, local acidic milieu, and local sensitization in active MTrPs. 11,12 MTrPs can also be classified as latent, in which case the MTrP is physically present but not associated with any spontaneous pain complaints. 10 A recent study showed that active MTrPs were most prevalent in the infraspinatus (77%) and upper trapezius muscles (58%) in patients with shoulder pain. 8 The thick and triangular infraspinatus muscle occupies the chief part of the infraspinatus fossa and assists in the external rotation of the arm and stabilization of the humeral head during arm movement. When compressed within the patients' level of pain tolerance, active MTrPs in this muscle cause both local and ReP and referred motor phenomena and often sympathetic hyperactivity from the shoulder region down to the frontal and lateral sides of the arms. 7,22 Therefore, it is necessary to verify the characteristics of ReP pattern in the infraspinatus muscle in specific populations.
We also hypothesized that deep dry needling (DDN) of a sensitive locus in the infraspinatus muscle 22 is more likely to elicit LTR and ReP than snapping palpation of the MTrP and we might find differences by sex. Before DDN, we must palpate the muscle tissue to find an MTrP “nodule” and then insert the needle. Dry needling insertion is typically used to treat muscles by eliciting a mechanical stimulation to nociceptors within the MTrP, which can elicit an LTR that provides a strong neural impulse to the MTrP circuit to break the vicious cycle of pain. 23 –26
Hence, the first aim of the study was to identify the most common ReP and compare its coincidence with that described by Travell and Simons. 7 Second, the study aimed to verify whether there were any significant differences by sex and types of technique used regarding the ReP pattern of TrP 2 of the infraspinatus muscle (Fig. 1), around the area described as more sensitive. 22 Finally, the third aim of the study was to determine the observed signs and symptoms evoked by DDN and manual palpation (MPal).
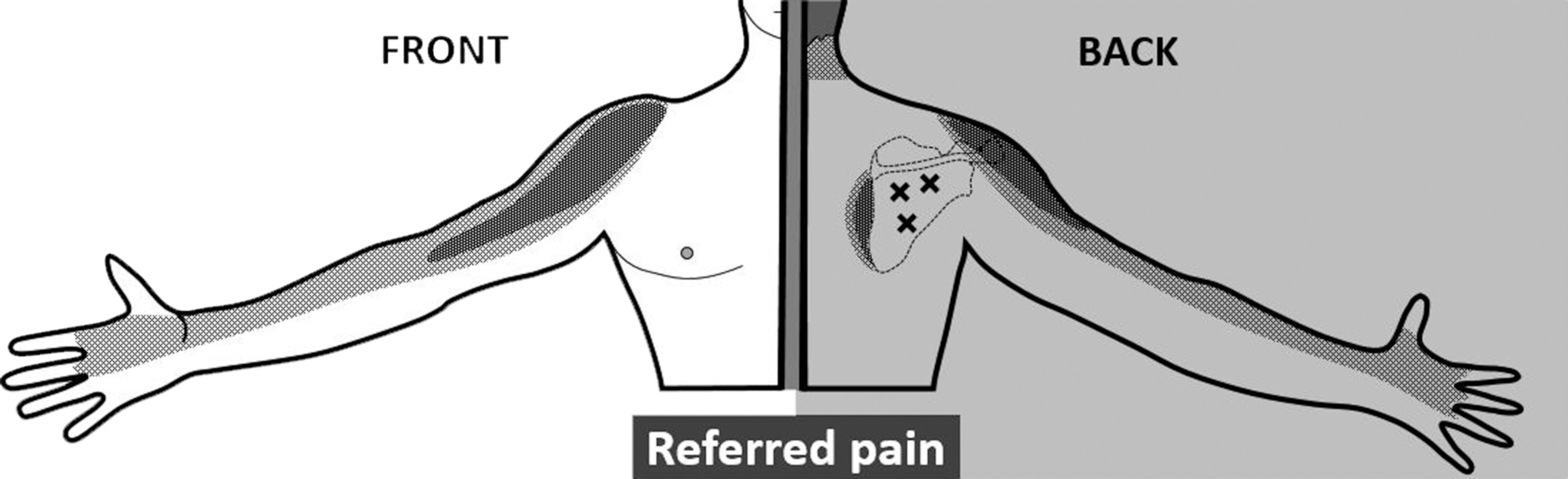
Infraspinatus myofascial trigger points and referred pain.
Materials and Methods
This study is a cohort study of patients randomized to two different examination methods, followed by a comparison of the observed signs and symptoms evoked by these two different methods, DDN versus MPal, on ReP patterns of the infraspinatus muscle in subjects with shoulder pain. The study was guided by the STROBE Statement (Strengthening the Reporting of Observational studies in Epidemiology). 27,28
Participants
One hundred and thirty-three participants (70.7% women), aged 18 to 47 years (mean age ± SD, 22.7 ± 5.9 years) with just shoulder pain (described as pain felt in the shoulder or upper arm) participated in the study. Staff and student population from University Miguel Hernández (Southeast Spain) were invited to participate in the study in July and August 2016.
Selection criteria were as follows: age 18–65 years; four or more hours a day seated in front of data visualization screens (tablets, computers, or smartphones); and individuals diagnosed with just shoulder pain in the last 6 weeks located in the anterior and/or lateral shoulder region (not subacromial pain syndrome, not subacromial impingement). Patients with evidence of serious medical illness, history of shoulder trauma or surgery, cervical radiculopathy, evidence of full-thickness rotator cuff tear, cognitive impairment, psychosocial disorders, bilateral affectation of shoulder pain, or pregnancy were excluded from this study.
The study was carried out in the physical therapy laboratories of University Miguel Hernández of Elche (Alicante). The study protocol was approved by the local Ethics Committee of the University Miguel Hernandez of Elche (DPC-EPP-001-15). Informed consent was developed in accordance with the requirements of the Declaration of Helsinki and was obtained from all subjects before data collection.
Diagnostic procedures
Participants were randomly divided into two groups using an informatic program (Microsoft Excel 2013): DDN group (n = 66; 22 men, 44 women) and MPal group (n = 67; 17 men, 50 women). The same physiotherapist carried out the techniques during 5–7 min in each patient. The same protocol was followed in both the DDN and MPal groups. The physiotherapist did not ask participants about their pain features (except taut band) or other relevant issues that could have influenced the physiotherapist.
For the DDN group, the reference position was a lateral position, lying on the nonaffected shoulder while the affected side was explored. The arm and elbow were flexed 90° resting on a pillow and legs placed with 90° hip and knee flexion to stabilize the body, with the head resting on a pillow to maintain body alignment. The physiotherapist stood in front of the participant and carried out the examination with flat palpation using the thumb to identify soreness taut before making the needle insertion (Fig. 2). Sterile stainless steel needles (length 40 mm/caliber 0.32 with a cylindrical plastic guide; Agu-punt®) were used. Around the infraspinatus area described by Ge et al. 22 was swabbed with 90° alcohol and the MTrP manually located using the thumb. Intramuscular needling was then carried out via DDN (according to the western medical) into the MTrP area without the introduction of any substances. 15,29 –32 The depth of needle insertion varied with thickness of the skin and subcutaneous fatty tissues at the site of the infraspinatus area 22 ; it was usually 2 to 4 cm. The aim was to elicit an LTR on inserting the needle into the MTrP area 29,30 and perform a neurological stimulation 7,33 (by rotating the needle 360°) to more easily evoke ReP, holding for 10 sec and then extracting the needle gently. This LTR must be elicited for successful therapy but it may be painful and post-treatment soreness is frequent. 34 The procedure was followed by 1 min of hemostatic compression. 35,36

Exploration of anatomical position.
The MPal group was explored in the same position as the DDN group. The physiotherapist used a thumb to identify soreness taut band and tried to elicit LTR and ReP in the infraspinatus around or in the area described by Ge et al. 22 First, three attempts were made to elicit an LTR using snapping palpation, if a response was obtained, this feature was considered valid. 7,15,17,37 After LTR, ReP could also be evoked by palpation (Fig. 2). This response depended on the amount of pressure applied and therefore also on subcutaneous thickness; the level of compressive pressure kept constant by applying enough digital pressure to cause the finger nail bed to blanch. When the nail turned pale, the amount of pressure was measured at ∼3–4 kg/cm2 and was maintained for 5–10 sec to evoke ReP. 16,38,39 An MPal-ReP was present if the ReP was far enough for the patient to feel more than just a local pain. The same principle was applied for the assessment of ReP elicited by DDN.
Both groups were examined by a physiotherapist with 15 years of clinical and teaching experience in the management of MTrPs using MPal and DDN techniques at the university. The correct application of the techniques requires experience in palpation and localization of taut muscle bands and MTrPs. 34 Immediately after intervention, data were collected by the same blinded observer in all cases. The participants left the examination room with the observer.
Measures We reported the anatomical regions where they patients reported feeling ReP and the level of pain reported by the patients during the examination procedures (subjective pain intensity).
• Mapping ReP. In the current study, the participants from both groups were asked to report whether ReP had been elicited and to describe the ReP pattern using an anatomical map of the upper half of the human body divided into 18 areas. Nine areas corresponded to the anterior part of the body and the other nine to the posterior part of the body (Fig. 3). The 13th area was not considered part of the ReP palpation or DDN area. In addition, the examiner asked patients whether their pain was superficial or deep and if they felt any paraesthesia.
• Infraspinatus muscle features. The infraspinatus muscle features analyzed were taut band, tender taut band, familiar pain, LTR, ReP, and active MTrP (soreness taut band and familiar pain). These were assigned a numerical value of 0 (yes) or 1 (no) for better statistical handling of the data.
• Subjective pain intensity. Pain intensity was assessed using a visual analogue scale (VAS) after examining the infraspinatus muscle area. 22,40 The VAS for pain measures the amount of pain experienced by a subject from the DDN ReP or MPal ReP group on a continuum from 0 to 10, with 0 being no pain and 10 maximum pain. This method has been proven a reliable, generalizable, and internally consistent measure of clinical and experimental pain. 41
• Other variables. Sex, age, weight, and height were recorded.
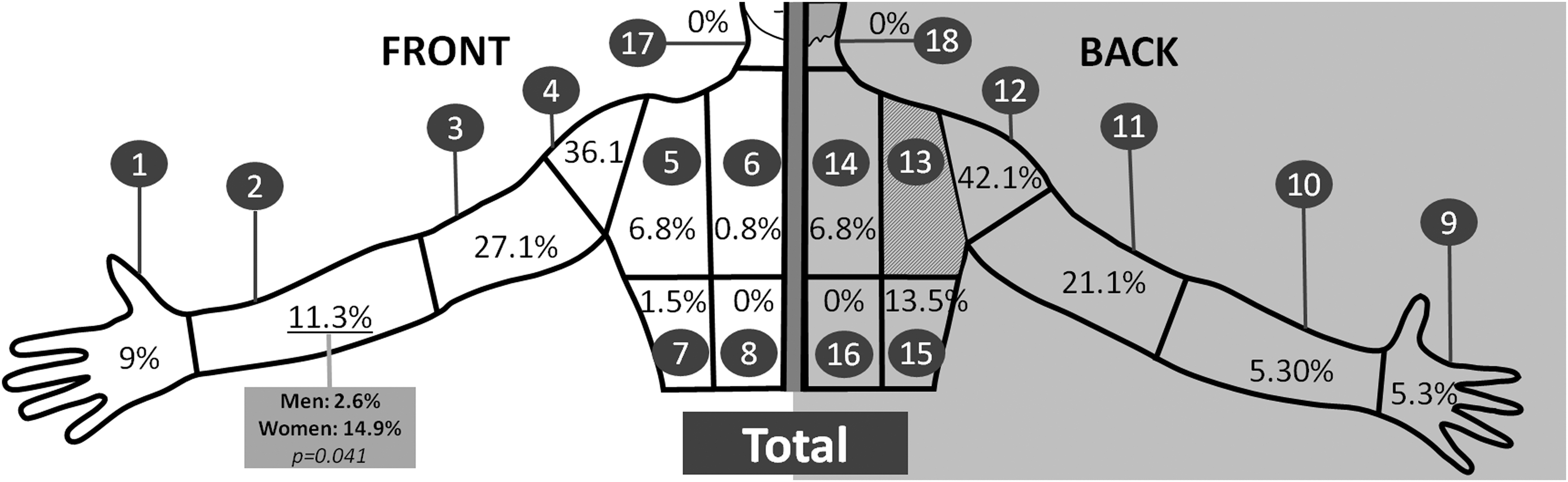
Mapping referred pain (nine areas corresponded to the anterior part of the body and the other nine to the posterior part of the body).
Statistical analysis
We used percentages to describe the variables. We estimated the different features according to DDN and MPal technique using the chi-square test. The 95% confidence intervals (CIs) were calculated for the differences between techniques. All analyses were carried out with the statistical program SPSS IBM (version 23.0).
Results
One hundred thirty-three subjects were selected for the study, with 66 assigned to the DDN group and 67 to the MPal group. There were no significant differences in mean age (95% CI, −1.1 to 3.0), weight (95% CI, −3.1 to 6.0), and height (95% CI, −1.8 to 4.4) between the two technique groups.
ReP pattern
Mapping the ReP of TrP in the infraspinatus muscle indicated that the areas with the highest percentage of ReP (over 20%) were the front (area 3; 27.1%) and back (area 11; 21.1%) of the arm, anterior (area 4; 36.1%) and posterior (area 12; 42.1%) shoulder, and infraspinatus muscle area (Fig. 3). In contrast, nobody had ReP in the front (17) and posterior (18) neck area. ReP areas obtained in the infraspinatus muscle were similar in both men and women and in both technique groups; no statistically significant differences were found (Table 1).
Values are mean ± SD, CI, or as otherwise indicated.
CI, confidence interval; DDN, deep dry needling; MPal, manual palpation; TrP, trigger points.
There were significant differences between sexes in zone 2 (p = 0.041), with 14.9% of women exhibiting ReP in this area compared to only 2.6% of men. The tender spot of the taut band also showed significant differences between men and women (p < 0.001), with it being sensitive in 68.1% of women versus 35.9% of men. Moreover, ReP occurred more easily in women with MPal than DDN (p = 0.071). In contrast, this did not occur with men (p = 0.96) (data not shown).
The prevalence rate of active TrP 2 in the infraspinatus muscle was 25.5% in men and 23.4% in women, with no significant differences between the sexes (p = 0.78).
Local twitch response
According to the technique used to evaluate ReP, no significant differences were found in the mapping of any of the 18 targeted areas. DDN was found to be significantly easily than MPal (p < 0.001) in evoking LTR.
The values obtained using the VAS showed no significant differences (p = 0.89) between palpation (5.2 ± 2.0) and DDN (5.1 ± 2.1) (Table 1).
Discussion
The main purpose of this study was to identify the most common ReP pattern and compare its coincidence with the original ReP pattern described by Travell and Simons. 7 We found that the pattern evoked in the infraspinatus muscle coincided with the original ReP pattern described, although the neck area should be questioned because nobody had pain referred in this area. Moreover, there were no significant differences in ReP pattern by sex and between MPal and DDN techniques when applied to TrP 2 of the infraspinatus muscle. On this issue, we think that the idea of fixed locations of MTrPs is obsolete, because the literature does not provide evidence for the existence of numbering in MTrP location and most people believe that MTrPs can occur in any section of a muscle, not just in certain stereotypical locations.
The patient's ReP pattern and tenderness is often the key to identifying the muscle responsible for the myofascial pain syndrome. 7 We found that ReP patterns in the infraspinatus muscle are not exactly as the original ReP pattern. Some patients feel pain in their fourth and fifth fingers and not in other areas of the upper body such as the neck. Hence, our results and clinical experience suggest that the original ReP pattern should be revised.
In addition, the immediate effects with MPal and DDN observed on ReP patterns show that the most common areas of TrP 2 in the infraspinatus muscle were similar by sex, with the exception of zone 2, with 11.7% of women compared to only 2.6% of men. ReP tends to present as deep pain in both sexes (men: 71.8%; women: 83%), and the incidence of paraesthesia was similar in both techniques (DDN: 30.3%; MPal: 41.8%). However, these significant p-values obtained by sex may be completely spurious findings.
On comparing the two groups according to sex, we found that ReP occurred more easily in women with MPal than DDN (p = 0.071). In contrast, this did not occur with men (p = 0.96). The ReP pattern coincided with Travell and Simons, 7 but there were some areas that were not referred, such as the base of the neck. It is difficult to compare our results to previous studies as no prior research has investigated the most common ReP pattern by sex and compare its coincidence with the original ReP pattern in the infraspinatus muscle. Hong et al. 16 compared the difference between the incidence of ReP elicited by digital compression of MTrPs (before MTrP injection) and that elicited by needling during MTrP injection. It was found that needling could elicit ReP in 87.7%, while palpation only in 53.9%. This difference is certainly possible because in MPal group we explored only the infraspinatus muscle that is easily palpated.
We found that the prevalence rate of active MTrP is 25.5% in men compared to 23.4% in women, with no significant differences between them (p = 0.784). These data support recent research being conducted on shoulder and neck pains suffered by those who remain seated or in front of data visualization screens for extended periods of time. 42 –44
Nonetheless, the prevalence rate of active MTrPs in the infraspinatus muscle in this study is 24.1%, lower than the 77% rate obtained in a different study of people with shoulder pain. 8 One possible explanation for the low prevalence of this study may be due to university students and that the inclusion criteria were individuals with just shoulder pain. Therefore, ReP patterns should be researched by age groups. The external validity of ReP patterns for the general population could be limited although could be considered in young adults. According to the current study, Travell and Simons 7 found that MTrPs were similar between sexes, but other studies have found that musculoskeletal disorders in the neck and shoulders are one of the most frequent disorders found in the working population and that they are more common in women. 45 In addition, this study found that women had more taut band tenderness than men on examining infraspinatus MTrPs.
Otherwise, we obtained statistically significant results showing that DDN is more easily evoked than MPal in generating LTR. Shah et al. 11 studied multiple elicited LTRs, analyzing their concentration during the recovery period, after the LTRs were significantly below baseline concentration. 11,12 In addition, the values obtained with the VAS showed no difference between the two techniques and between the sexes, with both displaying very similar values. This corresponds with the commonly observed decrease in pain and reduction of palpable stiffness after release of an MTrP via needling. 11,12,18,32,46,47 These findings do not coincide with another study that found women exhibited a higher intensity of postneedling soreness than men after dry needling of latent MTrPs in the upper trapezius muscle. 36 Needling very likely provides high-pressure stimulation to the multiple sensitized nociceptors via the descending pain inhibitory pathway, quickly interrupting the vicious “MTrP circuit” cycle to eliminate pain immediately 30 and avoiding the peripheral sensitization process that results in continued central sensitization. 10,48,49 Therefore, the best technique for total immediate inactivation of MTrP is “multiple rapid insertion.” 31
Finally, more research is needed to verify this ReP pattern, revised MTrP pain patterns, and MTrP locations in certain muscles, and to perform topographical mapping of mechanical pain sensitivity in specified muscles. 22,50
Study limitations
One muscle in the shoulder region was assessed. While other muscles may be implicated in shoulder pain, this study focused on ReP patterns of MTrPs in the infraspinatus muscle. The same physiotherapist performed both the dry needling and MPal. This could be a design flaw in the study and could have introduced potential bias. However, we tried to reflect the general clinical practice where the same physiotherapist usually performs MPal and then DDN. The present study had a small sample of men. Moreover, some patients presented with shoulder pain but did not exhibit an active TrP in the infraspinatus muscle; future studies should assess ReP patterns in patients with active MTrPs in the infraspinatus muscle.
Conclusions
The immediate ReP pattern evoked in the infraspinatus muscle coincides with the original ReP pattern described, although the neck area should be questioned. There were no significant differences in ReP pattern between the sexes and between MPal and DDN techniques when applied to TrP 2 of the infraspinatus muscle. In clinical practice, the review of ReP patterns of the infraspinatus muscle must be taken into account to improve in MTrP diagnostic. Future research should analyze the trigger point ReP patterns for each and every muscle in which ReP patterns are an important part of diagnosis to collect up-to-date data.
Footnotes
Acknowledgment
This research has been partially supported by the Ministerio de Economía y Competitividad of Spain, MTM2014-56233-P.
Author Disclosure Statement
No competing financial interests exist.