
Abstract
Objective:
Adjuvants or alternatives to antibiotics in urinary tract infections (UTIs) during pregnancy seem advisable because of possible fetal stress. The present study assessed the effectiveness of a food supplement containing L-methionine and Hibiscus sabdariffa L. and Boswellia serrata Roxb. extracts as a treatment for symptomatic UTIs in pregnancy.
Design:
Pregnant patients with symptomatic cystitis were screened for UTIs in three different clinical centers. Those unwilling to take antibiotics were offered two alternative treatments: (A) a 1-week treatment with the food supplement or (B) a week in which they were advised to increase their fluid consumption to more than 1.5 L daily. After 1 week, group B patients who still had positive urine cultures (UCs) or had no UC performed took the food supplement for an additional week. UCs were performed on all patients at the first visit (w0) and on most of them at 7 days (w1). Patients who were still positive at w1 or had no UC performed at w1 had UC performed 14 days (w2) thereafter.
Results:
Of 264 pregnant women enrolled, 216 joined group A, while 48 joined group B. At w1, 70.0% of group A patients and 43.2% of those in group B had negative UCs (p = 0.003). The reduction of bacterial load was 42.2% ± 8.0% and 4.5% ± 9.2%, respectively (p < 0.0001). At w1, symptoms disappeared in 135 patients (62.5%) in group A and 22 patients (45.8%) in group B (p = 0.03). At w2, 30 of 32 group B patients who switched to taking the supplement for the second week had negative UCs, including 20 who had been positive at w1. At w2, all group A patients had negative UCs. No side effects were reported.
Conclusions:
The food supplement provided effective treatment and might be an adjuvant or alternative to antibiotic therapy of symptomatic UTI in pregnancy.
Introduction
U
The rapid development of antibiotic resistance is an additional emerging problem as many if not most of Escherichia coli, Klebsiella, and Enterobacteria strains are already resistant to third-generation cephalosporins 14 –16 and carbapenems. 17,18 For these reasons, investigating adjunctive or alternative therapies to antibiotic treatment for UTIs in pregnancy seems advisable.
Among candidates, antimicrobial peptides, estrogen, vitamin D, herbal extracts, and probiotics have been proposed, 19 –21 along with L-methionine, an essential amino acid. Oral intake of L-methionine was shown to have some action in preventing the recurrence of UTIs in acute cystitis follow-up, 22 after renal transplantation, 23 and in patients with neurogenic bladder disorders, 24 significantly alleviating symptoms. It has been suggested that L-methionine may hinder bacterial adhesion by lowering the urine pH. 22 Among herbal extract ingredients, Hibiscus sabdariffa L. contains anthocyanins, flavonoids, polysaccharides, and organic acids with a wide range of potential therapeutic effects. 25 –27 Calyx extract of H. sabdariffa was shown to have a strong bacteriostatic effect against E. coli and Klebsiella pneumoniae strains isolated from the urine of patients affected by recurrent UTIs; it also prevented them from forming biofilms. 28 Other in vitro experiments have shown that H. sabdariffa extracts from calyces had a bactericide or bacteriostatic or antibiofilm effect on many other bacteria species. 29 –34
Another herbal ingredient of some interest for managing UTI symptom management is Boswellia serrata Roxb. Its anti-inflammatory activity 35 may rely on downregulation of TNF-α, IL-1β, and IL-6 messenger RNA (mRNA) expression, inhibition of NO (nitric oxide) production, 36 and reduction of proinflammatory leukotriene release. 37 Gum resin extracts of B. serrata are currently used to manage symptoms of osteoarthritis, 38,39 inflammatory bowel disease, rheumatoid arthritis, and asthma. 40 Recently, a food supplement containing L-methionine, H. sabdariffa L. calyx extracts, and B. serrata gum resin extracts was introduced on the market, with an indication for symptom management of UTIs. The present prospective, multicenter clinical study aimed to investigate the effectiveness of this supplement by monitoring both the symptoms and bacterial counts in two groups of pregnant women suffering from symptomatic UTIs: one undergoing treatment with the supplement (test group) and one simply advised to increase their daily fluid consumption.
Materials and Methods
A prospective multicenter protocol was designed that called for recruiting pregnant women with symptomatic cystitis, including an ongoing UTI infection (>100,000 colony-forming units [CFUs] at urine culture [UC]), and unwilling to undergo antibiotic treatment for their condition over a 12-month period (January to December 2015) at 3-day hospital practices. Other inclusion criteria were pregnancy (any trimester) and complaining about at least one of the following symptoms: dysuria, pollakiuria, suprapubic pain, fever, lumbar pain, or hematuria. The exclusion criteria comprised the presence of acute or chronic kidney disease, ongoing or a past history of renal colic, urolithiasis, renal cysts, renal hypertension, renal cell carcinoma, diabetes insipidus, any known allergy, acute liver failure, and chronic liver disease.
The protocol called for offering the patients two alternatives: (A) treating symptoms with the food supplement under investigation (2 g/day) for 1 week or (B) patients were advised to increase their daily fluid intake for a week to more than 1.5 L. The same advice to consume more than 1.5 L/day of liquids was given also to patients in group A. Table 4 reports the distribution of patients in the two groups according to their fluid consumption in the first week. After 1 week, a second UC was obtained from most patients. The few group B patients, who for some reason did not get one, started taking the supplement along with those whose UC was still positive. Group A patients stopped supplement consumption, even if their bacterial count was still positive. A scheme of the clinical protocol is provided in Figure 1.
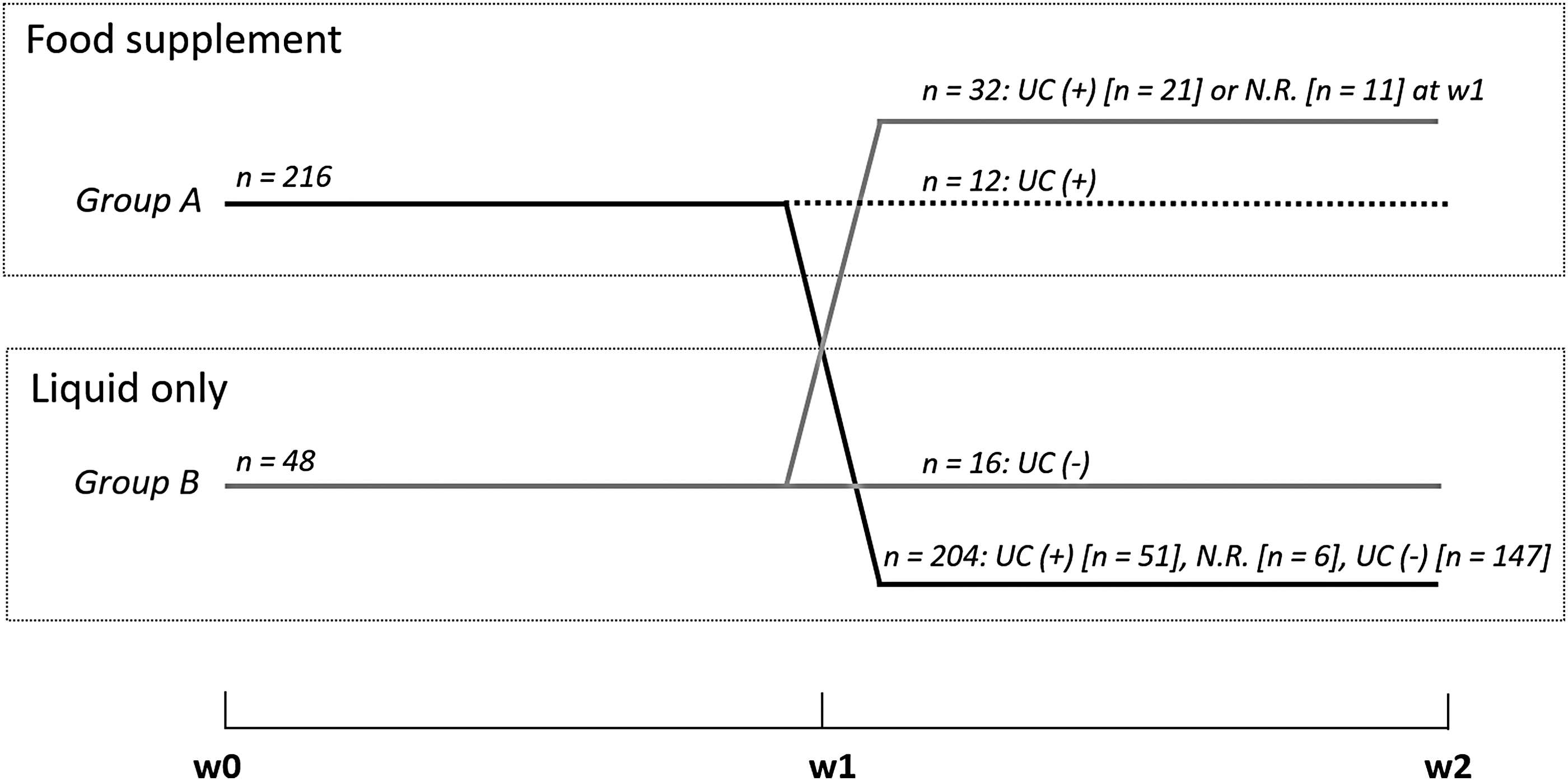
The protocol of the present study. Patients in group A took the food supplement, while patients in group B were advised only to consume more than 1.5 L of liquids daily. At the end of the first week (w1), all patients in group A switched to increased fluid consumption only, with the exception of 12 patients with positive UCs, who took the supplement for 1 additional week. After w1, the patients themselves decided whether to continue the treatment for another week or to only increase fluid consumption. At w1, group B patients who still had positive UCs or whose UC data were not recorded (N.R.) started taking the food supplement for 1 week. The number of patients in each group during w1 and w2 is indicated by “n.” UCs, urine cultures.
The food supplement (Acidif Plus; Biohealth S.r.l, Turin, Italy) was provided as 1-g tablets containing L-methionine (400 mg), H. sabdariffa extract (100 mg), and B. serrata (100 mg), corresponding to 10 mg of acetyl-keto-β-boswellic acid (AKBA). H. sabdariffa dry extract was obtained from the plant calyces using ethanol/water 30% v/v as extraction solvent and the extract ratio was 10:1 to 15:1. For the B. serrata extract, the gum resin part of the plant was used, the extraction solvent was 100% ethyl acetate, and the herb extract ratio was 10:1.
Patients were monitored at the first (recruitment) visit (w0), after 1 week (w1), and after 2 weeks (w2). At w0, patients were asked to provide the following information: age, profession (housewife, clerk, or laborer), the pregnancy trimester, and to subjectively assess their symptoms as mild, moderate, or severe. At all visits, patients were asked whether any of the following symptoms were present: dysuria, pollakiuria, suprapubic pain, fever, lumbar pain, or hematuria. At w1 and w2, patients were also asked to provide information about their daily fluid intake during the previous week (0.5–1.0, 1.0–1.5, >1.5 L) and if any gastric disorder or cutaneous rush developed while they were taking the supplement.
UC was performed on urine samples from all patients at w0. At w1, most patients provided samples, which were cultured. At w2, UCs were performed only on samples of patients that at w1 either were positive or did not provide samples.
UCs were performed according to standard protocols and using standard identification kits. During their first visit, patients who were willing to participate in the study provided their informed consent. The study protocol was approved by an ethics committee.
Statistical analyses
Chi-square tests were used to check for the homogeneity of patients as far as age, profession, trimester of pregnancy, severity of symptoms, symptom distribution, and liquid intake were concerned. As E. coli was the prevalent pathogen found in UC (see Results section), to test homogeneity for bacterial infection, patients were grouped as E. coli-infected and non-E. coli-infected patients and their distribution in the two groups was compared using a chi-square test. Homogeneity of the initial bacterial load in the samples was checked by means of a t-test for unpaired data.
To investigate whether the supplement had a significant effect on the overall bacterial infection, the distribution of patients in the two groups with negative or positive UCs at w1 was compared by means of chi-square tests. Additionally, the residual bacterial load in patients with positive UCs at w1 was averaged for each group, and the averages were compared using a t-test for unpaired data. The bacterial load reduction for each patient in each group was calculated by subtracting the bacterial load at w0 and w1, and the two data sets were compared by means of a t-test for unpaired data. The bacterial load percent reduction for each group was then calculated using the formula ([(average bacterial load [w0] − average bacterial load [w1])/average bacterial load [w0]] × 100).
To investigate whether the supplement provided any significant improvement of symptoms, data concerning the severity and distribution of symptoms at w1 were compared by means of chi-square tests. Distribution of patients in the two groups complaining of each symptom was also compared by means of chi-square tests.
The effect of the amount of liquid intake or the pregnancy trimester on symptoms and bacterial infection was investigated by creating contingency tables. These were analyzed by means of chi-square tests and calculating the percentage deviation using the formula ([[observed − expected]/expected] × 100).
To further investigate the effect of the supplement on subjective overall symptom perception and on each symptom, data collected at w2 were compared as outlined in the previous paragraphs. The effect on the bacterial count was assessed comparing data collected at w2 concerning those patients of the two groups who were positive to UC at w1 or who at w1 had not provided their samples. The significance level of all tests was 0.05. A dedicated software program (Origin 9.0, Microcal) was used for all statistical analyses. All values are presented as mean ± standard deviation.
Results
During the recruitment period, 612 pregnant women were screened; 232 were found to be affected by cystitis, 116 patients chose antibiotic treatment and did not take part in the study, and 264 were enrolled (22–41 years, mean 32 ± 6 years). Of these, 216 began treatment with the food supplement (group A), and 48 followed the advice to only increase their liquid oral intake (group B). The patients themselves chose whether to be included in group A or B after being informed that during pregnancy, increasing fluid intake to ∼1.5 L is sufficient to solve the problem in ∼30% of cases, at least partially. Antibiotic treatment with fosfomycin, considered safe during pregnancy, was not recommended as it was proved inefficient in these patients. The self-reported quantity of fluid intake in the two groups is reported in Table 1. First visit (w0) data are provided in Tables 2 and 3. The two groups were homogeneous as far as age (χ2 = 1.21, p = 0.41), profession (χ2 = 0.80, p = 0.67), pregnancy trimester (χ2 = 0.91, p = 0.63), severity of symptoms (χ2 = 3.53, p = 0.17), distribution of symptoms (χ2 = 2.63, p = 0.76), liquid intake (χ2 = 1.15, p = 0.56), and distribution of uropathogenic bacterial species (E. coli, non-E. coli) (χ2 = 0.99, p = 0.32) were concerned. The two samples were nonhomogeneous as far as the bacterial count was concerned (group A: 360,223 ± 423,791 CFU vs. group B: 243,333 ± 178,711 CFU, p = 0.003).
Patient data at w0: trimester of pregnancy, subjective symptom perception, profession, and bacterial count at UC.
CFU, colony-forming unit; UC, urine culture.
Results at w1
The effectiveness of the treatment was evaluated considering an eventual improvement or disappearance of the symptoms and of the bacterial load. Data at w1 are summarized in Tables 4–5. Table 4 shows UC results. Six patients in group A had no UC performed. Of the remaining 210, 147 (70.0%) had a negative UC. Eleven patients in group B had no UC performed. Of the remaining 37, 16 (43.2%) had a negative UC (Fig. 2A). The difference between the two groups was statistically significant (χ2 = 8.88, p = 0.003). All patients in group A whose UC was positive at w1 (N = 63, 30.0%) had a bacterial count smaller than that at w0. Of the 21 (56.8%) patients of group B whose UC was positive at w1, 17 (81.0%) experienced a reduction of the bacterial load, while the bacterial load increased in 4 (19.0%) of them. At w1, the average bacterial load in urine in patients who tested positive was 208,253 ± 153,709 CFU and 232,381 ± 145,153 CFU in groups A and B, respectively, the two being not statistically different (p = 0.55). The average bacterial reduction in the two groups was, respectively, −297,837 ± 314,660 (−42.2% ± 8.0%) and −124,324 ± 110.265 CFU (−4.5% ± 9.2%), a statistically significant difference (p < 0.0001).
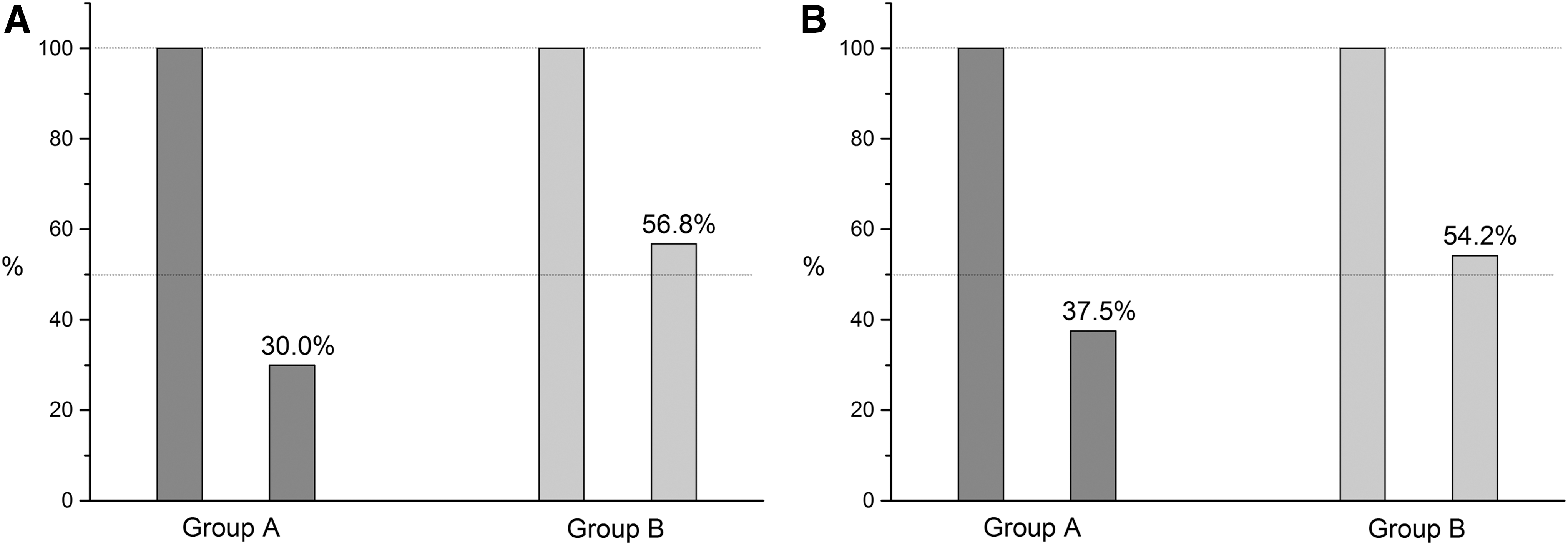
Percentage of patients in the two groups who were
N/A, patients who, for various reasons, did not undergo UC at w1; UC(+), positive; UC(−), negative.
The table also shows the number of patients, for each symptom, who had that symptom at w0 and still perceived it at w1 (NUL), who did not perceive that symptom anymore (NEG), and who were not perceiving the symptom at w0, but were perceiving it at w1 (POS).
Although patients in both groups were advised to consume more than 1.5 L of liquid daily, most of them reported consuming <1.0 L (Table 1).
At w1, 50 patients of the 216 in group A (23.1%) and 7 patients of the 48 in group B (14.6%) stated their symptoms were improved, but no statistically significant difference was observed (p = 0.25). One hundred and thirty-five patients (62.5%) in group A and 22 patients (45.8%) in group B stated that their symptoms had disappeared, the difference being statistically different (p = 0.03) (Figs. 2B and 3).
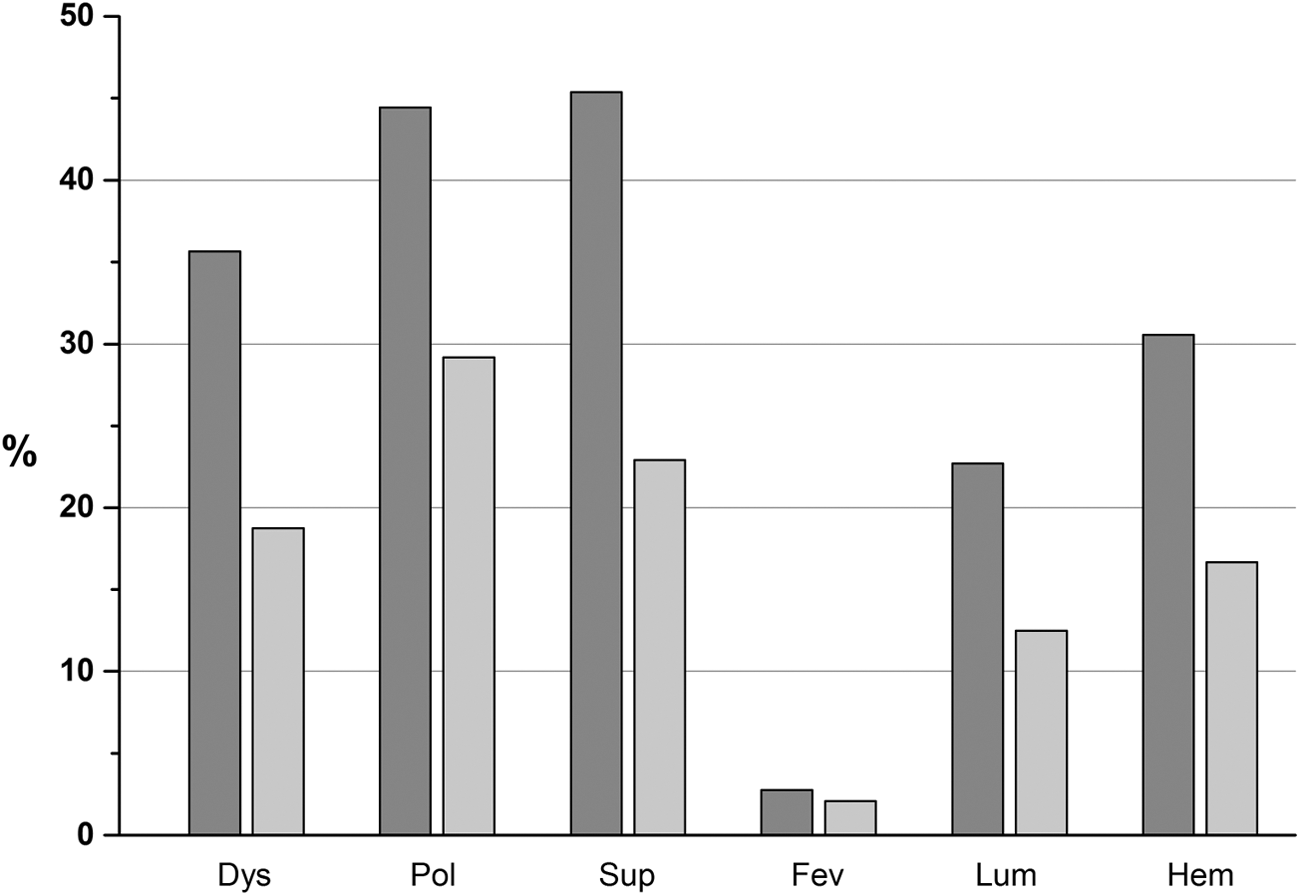
Percentage of patients who at w1 experienced complete disappearance of the following symptoms: Dys, dysuria; Pol, pollakiuria; Sup, suprapubic pain; Fev, fever; Lum, lumbar pain; Hem, hematuria. Dark gray: Group A (food supplement); light gray: Group B (liquid intake only).
Table 5 displays the distribution of symptoms under assessment at w0 and w1 and the effect of the treatment in the intervening period. A significant difference in symptom disappearance at w1 was observed only as far as suprapubic and lumbar pain (p < 0.0001 and p = 0.005, respectively) was concerned (Table 6). Concerning the effect of the amount of liquid on UCs, significant correlations were found for both groups (group A, χ2 = 11.73, p = 0.003; group B, χ2 = 13.1, p = 0.001). Analysis of percentage deviations (Table 7) showed that for group A patients, the more liquid consumed, the smaller the effect on UC reduction, whereas for group B, the greater the liquid intake, the larger the effect on UC reduction.
p, Significance of chi-square tests.
Significant.
UC(+), permanence of bacterial contamination in urine of patients; UC(−), disappearance of bacterial contamination in urine of patients; percentage deviation from values expected on the basis of the null hypothesis (i.e., the two variables are independent).
In group A, subjects who benefited from the treatment were more than expected if they were in their first trimester of pregnancy (χ2 = 8.46, p = 0.01). In contrast, the pregnancy trimester and the disappearance of positive UCs in group B showed no correlation (χ2 = 0.74, p = 0.69). (Table 8). No correlation was found in group A between the trimester of pregnancy and the disappearance of lumbar and suprapubic pain (χ2 = 6.85, p = 0.14; χ2 = 1.84, p = 0.77, respectively).
UC(+), permanence of bacterial contamination in urine of patients; UC(−), disappearance of bacterial contamination in urine of patients; percentage deviation from values expected on the basis of the null hypothesis (i.e., the two variables are independent).
Results at w2
Bacterial load at w2 was measured only for those patients who had positive UCs at w1 (63 patients in group A and 21 patients in group B) or had no UC performed at w1 (6 patients in group A and 11 patients in group B).
As a deviation from the protocol, 12 patients in group A of the 63 who had positive UCs at w1 continued taking the food supplement. At w2, all had negative UCs. The remaining 51 patients who had positive UCs at w1 and switched to the liquid intake only had negative UCs at w2. All six patients who had no UC performed at w1 had negative UCs at w2. In group B, 20 (95.2%) of the 21 patients who had positive UCs at w1 and then switched to taking the food supplement had negative UCs at w2. One patient who had a 400,000 colony-forming unit (CFU) count at w1 still had 100,000 CFU at w2. One of the 11 patients who had no UC performed at w1 had a positive UC (100,000 CFU) at w2. The remaining 10 patients had negative UCs. It is not possible to determine whether there is a correlation between fluid consumption and bacterial load at w2 as most patients, including the two cases with positive UCs at w2, did not report their fluid intake between w1 and w2. At w2, no patient from either group was complaining about any symptoms.
Tolerance and side effects
Both at w1 and w2, no patient taking the supplement complained about either skin rashes or gastric disorders.
Discussion
Standard antibiotic protocol for treating symptomatic lower UTIs calls for administering amoxicillin or cephalexin or choosing among other FDA category B antibiotics based on microbial sensitivity testing. 10 Yet, antibiotic exposure in pregnancy may have short- and long-term effects on infant weight 41 and childhood obesity 42 and might be linked with neurologic and atopic diseases. 43 –45 Scarce information is available about the link between the pregnancy trimester and the associated risk. 46 Antibiotics should therefore be avoided in the first trimester, when risk of teratogenic effects is higher. 47 Given this, investigating adjunctive or alternative therapies for symptomatic UTIs in pregnancy seems advisable. Results of the present study show that the food supplement under investigation is effective at reducing significantly the bacterial load in urine samples of pregnant women suffering from symptomatic UTIs when compared with increasing fluid consumption only. Significantly, 70% of women taking the food supplement had negative UCs after 1 week, and all patients who still tested positive had a significant decrease in the bacterial count. The significant antibacterial action of the food supplement may be ascribable to the effect on urinary pH exerted by L-methionine 23 and to the antimicrobial effect of H. sabdariffa L. 29 –34
The group B patients, who chose only to increase their fluid consumption, had a significantly smaller average bacterial count to begin with than the group that took supplement. Had the initial average bacterial counts in the two groups been more similar, the results of the study may have had an even higher statistical significance. A significant difference between the two groups was also observed regarding the total disappearance of symptoms. With regard to specific symptoms, patients taking the food supplement experienced a significant reduction in lumbar and suprapubic pain, compared with those who only increased their fluid consumption. Again, this may be a result of the combination of the antibacterial effect observed and the anti-inflammatory properties of the B. serrata Roxb. extract. 35 Results of the present study seem to indicate that when taking the food supplement, increased fluid consumption may diminish the antibacterial effects—possibly by reducing the concentration of L-methionine and H. sabdariffa extract active substances in the urine and thus limiting the pH-lowering effect and antimicrobial effects. Conversely, the positive correlation between increase in fluid consumption and disappearance of the infection in group B patients was expected under the rationale that the greater the urine flux and frequency, the higher its washout effect on urinary tract bacteria.
The antibacterial effect of the food supplement was found to be most effective in the first trimester. For the group B patients, no significant correlation between increased fluid consumption effectiveness and trimester status was found. These results suggest that the food supplement under examination may be especially useful in the first trimester of pregnancy, when the fetus is more sensible to exogenous substances. The effectiveness of the food supplement in relieving patients from lumbar and suprapubic pain appeared to be the same at all stages of pregnancy. The treatment can be recognized as effective when considering both the disappearance of these symptoms and the significant reduction of bacterial load.
Results observed at w2 for group B patients who still had positive UCs after 1 week and switched to the food supplement confirm that the food supplement was capable of exerting a significant antibacterial effect as most of the patients (95.2%) had negative UCs 1 week later.
An intriguing question arises when comparing the spontaneous resolution rate of the infection in group B patients (43.2%) with 100% resolution in group A patients who still had positive UCs after 1 week of taking the supplement and then did nothing for the second (supplement-free) week. Whether the higher spontaneous resolution rate of group A patients was due to their lower bacterial loads after 1 week of consuming the supplement or due to some effect of the food supplement persisting after its consumption stopped should be the subject of further investigation. A limitation of the present study was the lack of homogeneity between the two groups studied due to the different self-selection in the groups. Further prospective studies, including more subjects divided in treatment and control groups with similar numerosity, should be carried out, and the investigations should be expanded to include not just symptomatic cystitis but also other kinds of urinary infections.
Conclusions
When used to treat symptomatic UTIs in pregnant women, the food supplement under investigation provided significant symptomatic relief and significant antibacterial effect, with no reported side effects. Further studies should compare its effectiveness with that of common antibiotics prescribed to treat symptomatic UTIs in pregnant women to investigate its validity as an alternative to antibiotic therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.