
Abstract
Objectives:
The aim of this study was to present an overview of the research on the effects of yoga on positive mental health (PMH) among non-clinical adult populations.
Methods:
This was a systematic literature review and meta-analysis, including a risk of bias assessment. The electronic databases PubMed/Medline, Scopus, IndMED, and the Cochrane Library were searched from 1975 to 2015. Randomized controlled trials (RCTs) on the effects of yoga interventions on PMH among a healthy adult population were selected.
Results:
A total of 17 RCTs were included in the meta-analysis. Four indicators of PMH were found: psychological well-being, life satisfaction, social relationships, and mindfulness. A significant increase in psychological well-being in favor of yoga over no active control was found. Overall risk of bias was unclear due to incomplete reporting.
Conclusions:
The current body of research offers weak evidence that the practice of yoga contributes to an increase in PMH among adults from non-clinical populations in general. Yoga was found to contribute to a significant increase in psychological well-being when compared to no intervention but not compared to physical activity. For life satisfaction (emotional well-being), social relationships (social well-being), and mindfulness no significant effects for yoga were found over active or non-active controls. Due to the limited amount of studies, the heterogeneity of the intervention, and perhaps the way PMH is being measured, any definite conclusions on the effects of yoga on PMH cannot be drawn.
Introduction
T
Positive mental health
Positive psychology is a movement that focuses on the scientific study of the conditions and processes contributing to the flourishing or optimal functioning of people, groups, and institutions. 10,11 With the emergence of the positive psychology movement, there has been a shift in the view of the concept of mental health. The traditional approach to mental health regards mental illness and mental well-being as two opposite poles of a continuum. 12 The notion that mental health does not equal the absence of mental illness is gaining territory. Positive mental health (PMH) is defined as a health state characterized by the presence of psychological well-being (positive individual functioning and self-realization), emotional well-being (feelings of happiness and satisfaction), and social well-being (positive social functioning). 13,14 The Dual Factor Model of Mental Health 15 –17 and the Two Continua Model 13,14,18 –20 are two similar models that suggest mental illness and mental well-being are two separate dimensions that correlate.
Positive psychology and yoga
In order to understand and treat mental illnesses, clinical psychology historically has focused on classifying psychological dysfunctions. 11,21 Positive psychology aims at changing this approach and has developed various interventions in the past two decades. These positive psychology interventions consist of techniques and exercises aimed at developing personal strengths and enhancing positive emotions, life satisfaction, personal growth, and meaning. 22 Examples of evidence-based positive psychology exercises are remembering three good things, 23 –25 identifying and using character strengths, 26 –28 performing acts of kindness, 29 counting one's blessings, 30 gratitude exercises, 31 –34 appreciation of beauty exercises, 35 and savoring the moment exercises. 36 Positive psychology has contributed to a shift from a focus on the negative indicators of mental health toward more research on positive indicators of mental health. A wide variety of recently published meta-analyses report on indicators of PMH such as compassion, 37,38 forgiveness, 39,40 gratitude, 41 goal setting, 42 hope, 43 and resilience. 44,45 Many positive psychology interventions have also integrated mindfulness meditation. 46 –50 Positive psychology in general promotes mind–body interventions, but its focus appears to be limited to interventions based on Buddhist principles such as mindfulness-based interventions 51 –54 and acceptance and commitment therapy. 55,56 Besides ongoing research of the effect of mindfulness-based meditation on negative indicators of mental health, such as anxiety, depression, and stress, there is a growing number of studies that investigate the link between mindfulness and specific positive constructs, such as compassion, 57,58 forgiveness, 59 gratitude, 60 happiness, 61 optimism, 62 self-awareness/self-control, 63 and character strengths and virtues. 64 However, while the positive psychology movement seems to have fully embraced mindfulness and the Buddhist philosophy, it appears that it is neglecting the benefits of yoga and ignores the psychological and philosophical knowledge that can be found in yoga philosophy and Hinduism. During the systematic database search that was performed in this study, only a handful of publications were encountered discussing the relation between yoga and positive psychology 65 –67 or indicators of PMH, for example passion. 68 This is odd when positive psychology and yoga share much common ground when it comes to their specific goals; both focus on achieving well-being, increasing meaning in life, and personal growth.
Aim of the study
Although most people believe and expect that yoga will increase their well-being, to the best of the authors' knowledge, no studies have examined the relationship between yoga and (positive) mental well-being among healthy adults. The aim of this meta-analysis was to investigate the effects of yoga on PMH among adults from non-clinical populations in order to establish if there is a possible causal relation. A national survey on the mental and physical benefits of yoga among 4307 practitioners reported that only 1.1% of the practitioners of yoga indicated that they were languishing, that is, experiencing severe mental and/or physical problems, 69 while a bibliometric analyses reported that 73.9% of published randomized controlled trials (RCTs) on yoga focus on non-healthy participants. 2 This study was interested in whether yoga can improve PMH in healthy individuals rather than serving as a therapeutic intervention. Physical conditions clearly influence PMH indicators, mental conditions even more so. So in order to reduce heterogeneity, only trials on healthy individuals (or those from the general population) were included. Only outcomes of RCTs were included because the RCT is widely taken as the golden standard for doing scientific research in the field of medicine and psychology. 70 –72
Methods
The PRISMA guidelines for systematic reviews and meta-analyses 73 and the recommendations of the Cochrane Back Review group 74 were followed in the planning and the implementation of the review.
Inclusion criteria
The inclusion and criteria for this review were: (1) adults belonging to a non-clinical population; (2) studies with outcomes that could be identified as positive indicators of mental health; (3) all structured forms of yoga that offer a postural-based (asanas), breathing-based (pranayama), or meditation-based (dnyana) program or a combination of these three elements; and (4) RCTs. Research indicates that the various yoga styles do not differ in their odds of reaching positive conclusions, 75 so there will be no differentiation of the effects per style.
Literature search
Data were gathered in the following ways. First, for studies prior to 2014, all RCTs were included that were found in a bibliometric analysis that was conducted in 2014 by one of the authors. 2 In this analysis, the electronic databases Medline/PubMed, Scopus, the Cochrane Library, and IndMED were searched, and the tables of content of yoga-specialty journals not listed in the medical databases were also checked. Search terms around the keyword “yoga” were used for the literature search; the complete search strategy for Pubmed/Medline is shown in Table 1, and the search strategy was adapted for the other databases. Second, for studies from 2014 to 2015, the databases PubMed/Medline, Scopus, InMED, and the Cochrane Library were also searched using the aforementioned strategy. In addition, references of several meta-analysis, reviews, and trials were checked. Only studies that were published in articles in peer-reviewed journals were included, and research from grey literature, dissertations, or conference proceedings was not included.
Asterisks (*) represent truncations (PubMed finds all terms that begin with a given text string).
Data extraction
The data extraction was performed by one reviewer (T.H.) and independently checked by a second reviewer (H.C.). The following data were extracted: authors, year of publication, country origin, population, intervention, number of participants who completed the trial, primary and secondary outcomes, and post measurements of mean and standard deviation. Consensus was achieved by discussion.
Risk of bias assessment
Two authors (T.H. and H.C.) independently assessed the risk of bias using the Cochrane risk of bias tool 74 on the following domains: selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (adequate outcome assessor blinding), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting), and free of other bias (such as extreme baseline imbalance, author alliance, and population bias). 76 Consensus was achieved by discussion.
Data analysis
Assessment of overall effect size
Separate meta-analyses were conducted for comparisons of yoga to different control interventions using Review Manager 5 software v5.1 (The Nordic Cochrane Centre, Copenhagen). Meta-analyses were conducted by random effects models if at least two studies assessing this specific outcome were available. Standardized mean differences (SMD) with 95% confidence intervals (CI) were calculated as the difference in means between groups divided by the pooled standard deviation using Hodges's correction for small study samples. 55 Where no standard deviations were available, they were calculated from standard errors, confidence intervals, or t-values, 77 or attempts were made to obtain the missing data from the trial authors by e-mail. A positive SMD (i.e., higher values in the yoga group) was defined as indicating beneficial effects of yoga compared with the control intervention. If necessary, values were inverted. 74 Cohen's categories were used to evaluate the magnitude of the overall effect size with (1) SMD = 0.2–0.5: small; (2) SMD = 0.5–0.8: medium; and (3) SMD >0.8: large effect sizes. 78
Assessment of heterogeneity
Statistical heterogeneity between studies was analyzed using the I 2 statistics, a measure of how much variance between studies can be attributed to differences between studies rather than chance. The magnitude of heterogeneity was categorized as (1) I 2 = 0–24%: low heterogeneity; (2) I 2 = 25–49%: moderate; (3) I 2 = 50–74%: substantial; and (4) I 2 = 75–100%: considerable. 77,79 The chi-square test was used to assess whether differences in results were compatible with chance alone. Given the low power of this test when only few studies or studies with low sample size are included in a meta-analysis, a p-value of ≤0.10 was regarded as indicating significant heterogeneity. 54
Sensitivity analyses
To test the robustness of significant results, sensitivity analyses were conducted for studies with a high versus low risk of selection bias (adequate random sequence generation and allocation concealment). If heterogeneity was present in the respective meta-analysis, sensitivity analyses were also used to explore possible reasons for statistical heterogeneity.
Publication bias across studies
Assessment of publication bias was originally planned by using funnel plots generated using Review Manager software. 80 As fewer than 10 studies were included in each meta-analysis, funnel plots could not be analyzed.
Results
Study selection
A total of 1901 records were identified. A flow chart is presented in Figure 1. After the removal of duplicates, 495 records remained for screening. Of these, 297 articles were excluded because they were related to the clinical population, leaving 202 full-text articles to be assessed for eligibility. Of these, 182 were excluded: 170 studies did not have any outcome that could be classified as a positive outcome, eight studies did have a positive outcome but the population was <18 years of age, one was not a yoga intervention, four used a program where yoga was combined with other invention types, and in one study had its results published in an earlier study, which was already included. In total, 20 studies were included in the systematic review: 17 studies were included in the quantitative meta-analysis; three studies were included in the qualitative analysis due to insufficient raw data (incomplete means and/or standard deviation).
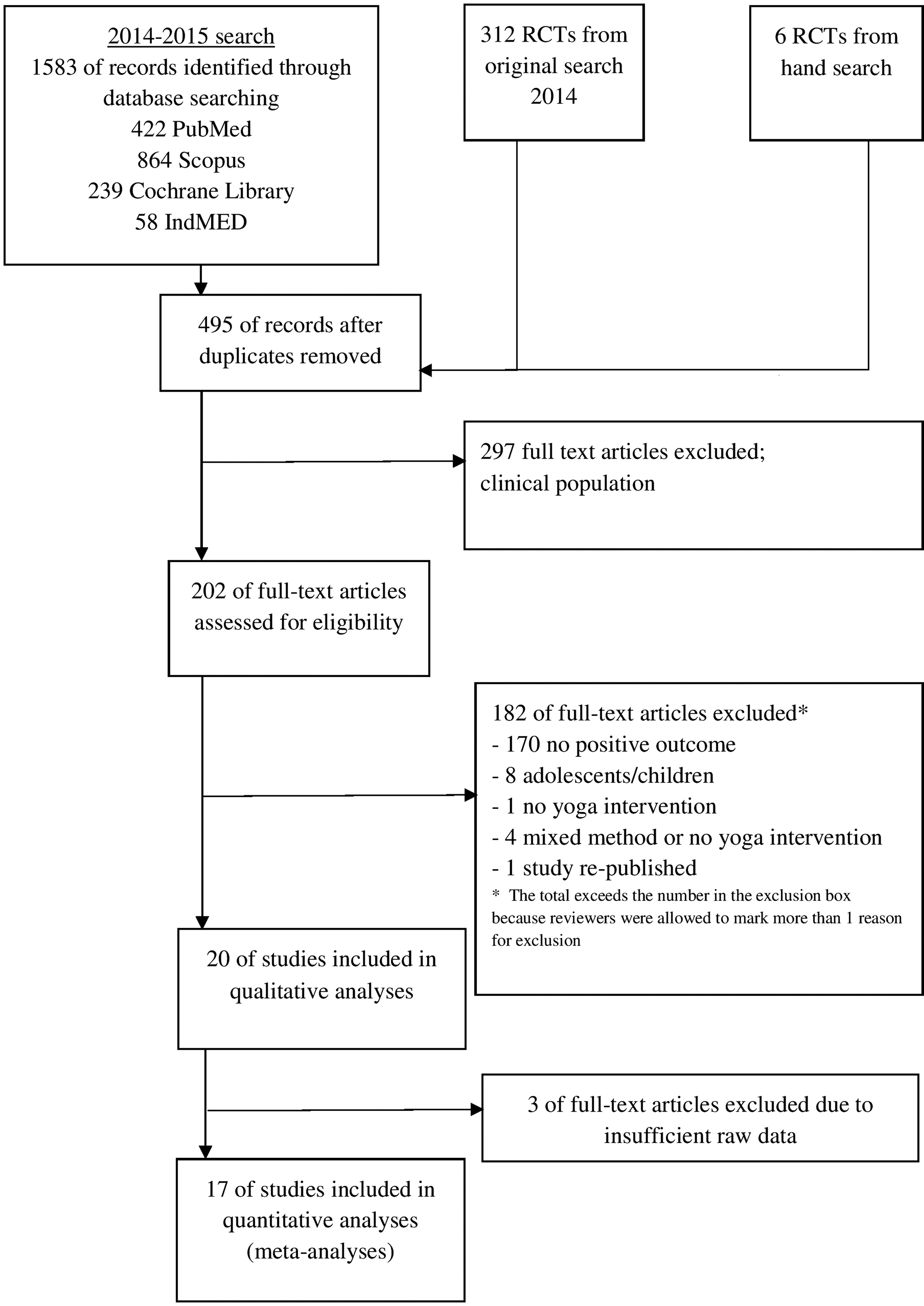
Flowchart of the inclusion of studies.
Study characteristics
Table 2 show the characteristics of the 20 included RCTs. Seven studies originated from India, 81 –87 six from the United States, 88 –92 four from the United Kingdom, 93 –96 one from Australia, 97 one from Japan, 98 and one from Turkey. 99 The studies were published between 1983 and 2015. The total number of participants was 1901, of which 769 received an exclusive yoga intervention. In eight studies, the yoga intervention consisted of a combination of physical postures (asanas), breathing exercises (pranayama), and meditation (dnyana). In eight studies, it consisted of a combination of physical postures and breathing exercises. One study consisted of physical postures and meditation. Three studies consisted of only physical postures. The average intervention period was 9 weeks, with an average of 12 sessions that lasted around 53 min on average. In 10/20 studies, daily practice between 10 and 60 min, with an average of 30 min, was advised. The control conditions used were yoga + physical exercises (100), physical exercises (319), mindfulness (94), progressive muscle relaxation (65), brain wave vibration (29), and non-active control groups (536 participants). The age of the participants ranged from 18 to 77 years, with some studies not reporting (mean) age. The female ratio in total was 61%. (The study by Haber 90 reported the female ratio of two groups at baseline, which was 66% and 60%, but did not report the number of females who completed the trial.)
Y, yoga; PE, physical exercise; BWV, brain wave vibration; M, mindfulness; PMR, progressive muscle relaxation; w, weeks.
Yoga types: A, asanas; P, pranayama; D, dnyana.
Instruments: BS, Bradburn Scale; CAMS-R, Cognitive and Affective Mindfulness Scale-Revised; CDSES, Chronic Disease Self-Efficacy Scales; FMI, Freiburg Mindfulness Inventory; GDS, Geriatric Depression Scale; GSES, General Self-Efficacy Scale; IPPA, Inventory of Positive Psychological Attitudes; LGMS, Lawton's PGC Morale Scale; LOQ, Life's Odyssey Questionnaire; MAAS, Mindfulness Attention Awareness Scale; MCS, Mental Component Summary; PANAS-X, Positive and Negative Affect Scale; PSPP, Physical Self-Perception Profile; PWS, Psychological Well-Being Scale; RSS, Rosenberg Self-Esteem Scale; SRDI, Smith Relaxation Disposition Inventory; SRSI, Smith Relaxation States Inventory; STAI, State–Trait Anxiety Inventory; STAXI, State–Trait Anger Expression Inventory; WEMWBS, Warwick–Edinburgh Mental Well-Being Scale; WHOQOL-100,World Health Organization Quality of Life; WHOQoL-BREF, World Health Organization Quality of Life Scale.
Study measures
In total, 32 types of measures were found that could be classed as indicators of PMH (at ease/peacefulness, attentiveness, aware, awe and wonder, childlike innocence, disengagement, independence, joviality, joy, emotional well-being, environment, life and health attitude, life purpose satisfaction, love and thankfulness, mental quiet, mindfulness, mystery, peacefulness, prayerfulness, quality of life, rested/refreshed, positive affect, psychological well-being, purpose and meaning, self-assured/self-confidence, self-efficacy, self-esteem, serenity, spiritual, social relationships, strengths and awareness, and timeless/boundless). However, a meta-analysis requires a comparison of a similar outcome in a minimum of two studies with a comparable control group (either active or non-active control group). In total, only sufficient data on four indicators of PMH was available to do the meta-analysis. These four indicators were psychological well-being, life satisfaction, social relationships, and mindfulness. The first indicator corresponds with the construct of psychological well-being in the framework of PMH. The second indicator corresponds with emotional well-being, and the third indicator corresponds with social well-being. Mindfulness is a state of focused nonjudgmental attention, with the awareness being in the present moment, 100,101 and it is associated with increased well-being. 102 –104 It could be regarded as a proxy measure of PMH in general.
Risk of bias in individual studies
The risk of bias assessment for each study is shown in Table 3. Selection bias was low in 8/20 studies. In the other studies, the risk could not be determined because the randomization process was not described. Allocation concealment was only described properly in three studies and was therefore classified as having a low risk of bias. Blinding of participants and personnel was described in three studies, leading to the classification of a high risk of bias. Only one study properly described outcome assessor blinding, scoring a low risk of bias. The other studies did not report any information. Risk of attribution bias was low in three studies, high in four studies, and unclear in 13 studies. In 18 studies, all analyzed outcomes were reported, so these studies appear to be free from selective reporting. Finally, three studies were classified as having a general high risk of bias due to author affiliation, not specifying funding, or having high unaccounted dropout rates. Eight studies that clearly addressed funding and absence of conflict of interest were rated as having a low risk of bias. In conclusion, the overall risk of bias could not be determined due to unclear reporting.
Data analysis
Meta-analyses of psychological well-being revealed significant group differences favoring yoga over no intervention (n = 768; SMD = 0.69, 95% CI 0.16, 1.22; p = 0.01; I 2 90%). No such group differences occurred compared to physical activity (n = 552; SMD = 0.00, 95% CI −0.34, 0.35; p = 0.99; I 2 72%; Fig. 2). No effects of yoga compared to no intervention occurred for life satisfaction (n = 140; SMD = 0.39, 95% CI −0.47, 1.25; p = 0.38; I 2 80%; Fig. 3); and social relationships (n = 310; SMD = 0.30, 95% CI −1.21, 1.81; p = 0.69; I 2 95%; Fig. 4). Further meta-analyses on mindfulness revealed no group differences between yoga and no intervention (n = 169; SMD = −0.09, 95% CI −0.47, 0.29; p = 0.65; I 2 27%); and yoga and physical activity (n = 52; SMD = −0.17, 95% CI −0.72, 0.38; p = 0.54; I 2 0%); while group differences favoring mental activity over yoga were found (n = 179; SMD = −0.30, 95% CI −0.60, −0.01; p = 0.05; I 2 0%; Fig. 5).

Effects of yoga on psychological well-being.
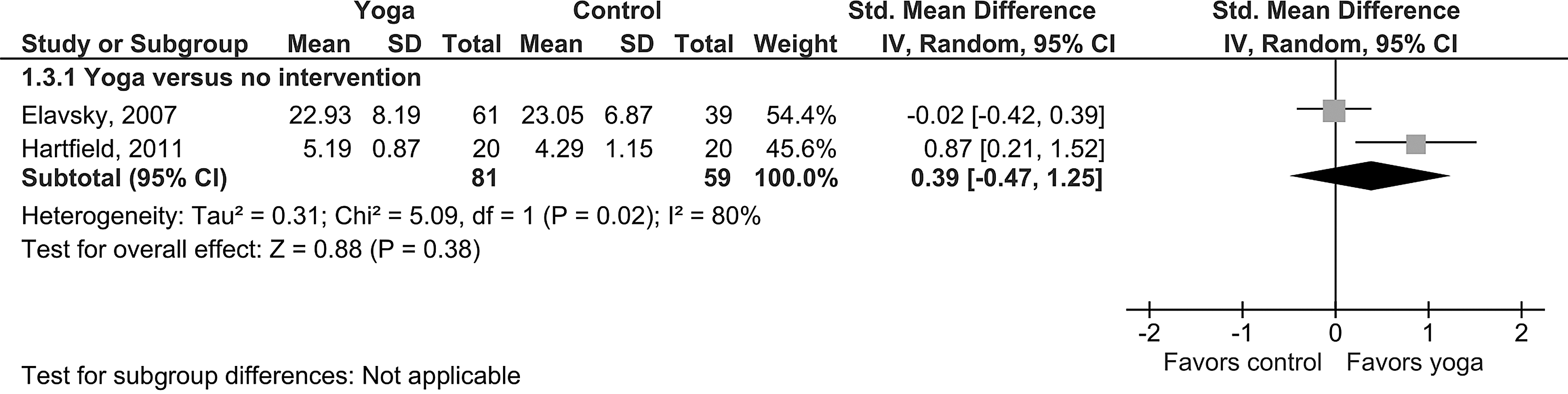
Effects of yoga on life satisfaction.
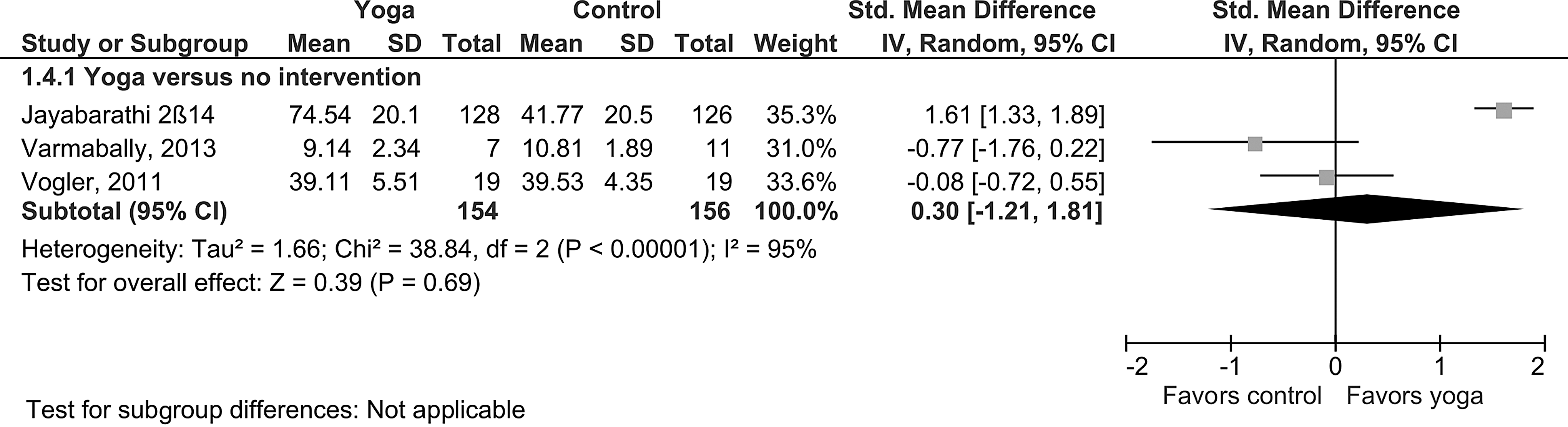
Effects of yoga on social relations.
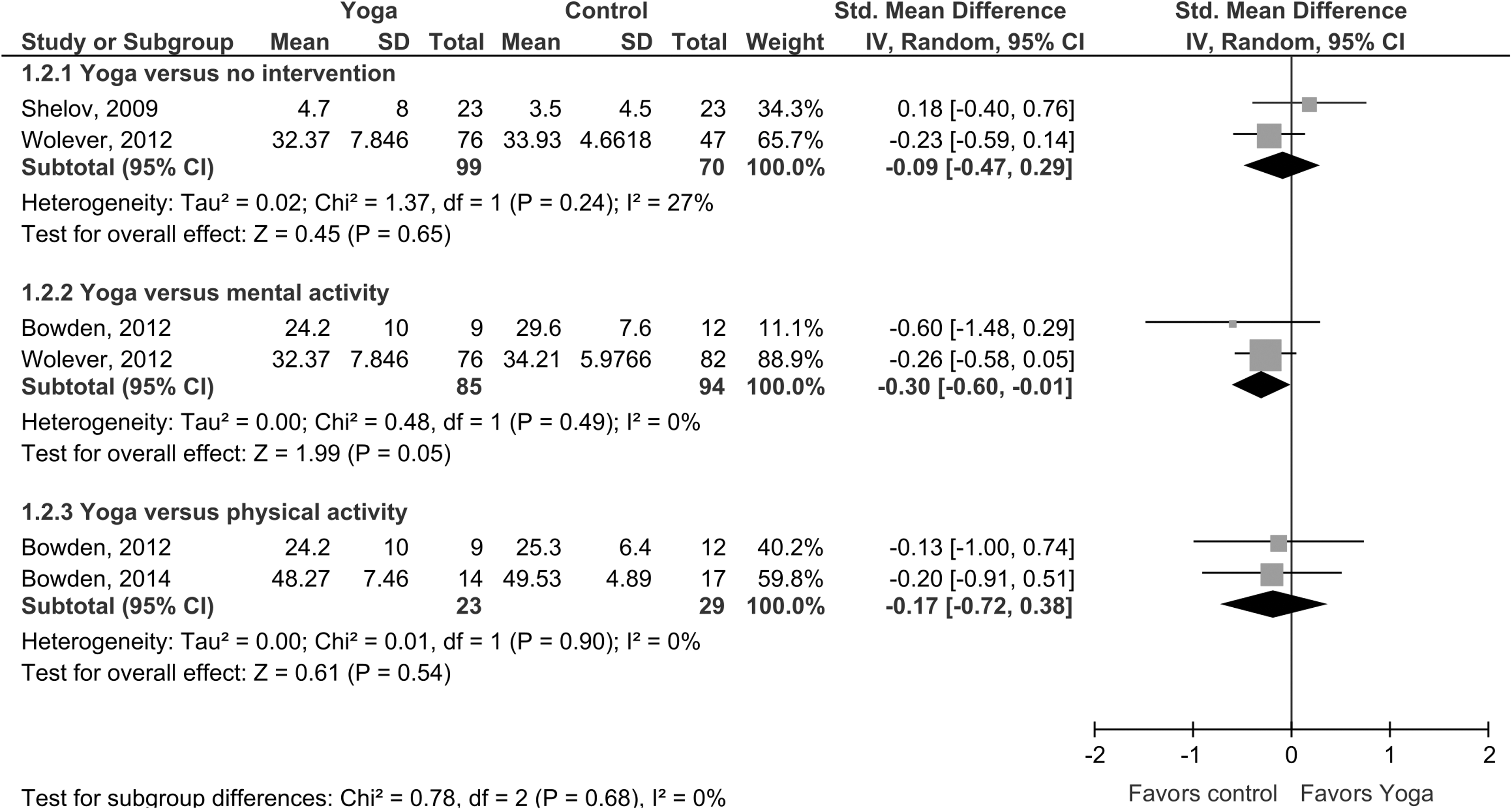
Effects of yoga on mindfulness.
Sensitivity analyses
When only studies with a low risk of selection bias were included, only the effects of yoga compared to no intervention on psychological well-being remained significant, although only one RCT could be included in this analysis (n = 18; SMD = 1.02; 95% CI 0.00–2.04; p = 0.05). The effect on mindfulness favoring mental activity over yoga no longer was significant, although only one RCT could be included in this analysis (n = 18; SMD = −0.60; 95% CI −1.48 to 0.29; p = 0.19).
Discussion
Following a systematic literature search, 17 studies were included in the meta-analysis. Although 32 different indicators of PMH were found, only four of these indicators were present in two or more studies: psychological well-being, social relationships, life satisfaction, and mindfulness. For psychological well-being, yoga was found to have favorable effects over no intervention, but it did not have a favorable effect over mental activity or physical activity. In relation to life satisfaction and social relationships, no significant effects were found for yoga versus no intervention. For mindfulness, yoga interventions had no significant effects on mindfulness in comparison to no intervention, and no significant effect compared to control groups that featured mental and psychical activity. So it appears that yoga is not effective in the development of PMH in general, except maybe for the dimension psychological well-being.
Limitations
There are several limitations in this meta-analysis. First, a very limited number of studies focused on positive outcomes in healthy adults. From almost 500 RCTs, only 20 (4%) studies reported positive outcomes for yoga among healthy adults—a very disproportionate ratio. While 32 different indicators of PMH were identified, only measures for four indicators could be included: psychological well-being, life satisfaction, social relationships, and mindfulness. For psychological well-being, eight studies were found that measured the effect of yoga versus no intervention, and six studies for yoga versus physical activity. For life satisfaction and mindfulness, only two studies were found that measured the effect of yoga versus an active or no intervention. For social relationships, only three studies were found. Based on only two or three studies, definite claims on the presence or absence of certain effects cannot be made. In sum, a firm conclusion can only be drawn on the effects of yoga on psychological well-being—that yoga only improves psychological well-being compared to no intervention. It could be argued that with so such a small number of studies, a meta-analyses is not warranted. However, Davey et al. performed an analysis of 22,453 meta-analyses and found the median number of included studies was three; less than three quarters contained five or fewer studies. 105 Thus, the limited amount of studies in the present meta-analysis is not regarded as an exception.
Second, the findings of this study must be interpreted with caution due to the clinical heterogeneity of the intervention in regard to the various yoga traditions and the differences in duration and frequency of the intervention. In addition to the heterogeneity, most studies displayed poor methodological reporting, making a clear risk of bias assessment practically impossible. Third, there are limitations in the way psychological well-being is being measured. In the majority of the studies, psychological well-being was measured using quality-of-life questionnaires, and these reflect the traditional view of mental health—that mental health is the absence of mental illness. The presence of positive outcomes is more likely to be found when measured by an instrument that reflects the dual factor/two continua model approach to mental health by using questionnaires such as the Mental Health Short Form, 106 the Positive Mental Health instrument, 107 or even the Positive and Negative Affect Scale. 108
Suggestions for future research
First, as only 5% of the current research focuses on positive outcomes, future research in the field of yoga should make a shift from the focus on negative outcomes toward positive outcomes, so there is more of a balance between the two. Second, positive constructs should not be measured by scales that define PMH merely as the absence of mental illness. It is also suggested that PMH is not only measured in a general sense (psychological well-being and quality of life) but more specifically, just as mindfulness research focuses on the relation with specific positive constructs. Third, studies are needed on the effects of yoga intervention that focus primarily on physical postures (asanas). Whereas as relationship between PMH and meditation has been found, there are simply no studies that focus on the sole effects of yoga meditation (dnyana). Future studies should therefore focus more on the effects of yogic meditation. Fourth, since the overall risk of bias could not be assessed due to unclear reporting, future researchers should pay more attention to the quality of methodological reporting, for example by following the CONSORT guidelines for reporting parallel group randomized trials. 109 Fifth, it is questioned whether modern researchers in the field of psychology and yoga are actually measuring what practitioners intend to achieve through yoga. In the present meta-analysis, only one study was found that measured spirituality. A survey among 604 U.S. students reported that 73% considered yoga to be a spiritual activity, 8 and many practitioners expect that yoga will lead to an increased sense of spirituality. 7 However, the spiritual aspects of yoga are rarely addressed in research. 110 In light of this, the field is reminded that the original goal of yoga, as described in the Yoga Sutras, 111 was the removal of fluctuations of the mind. What Patañjali addresses as “fluctuations of the mind” could be associated with modern psychological constructs such as worrying, rumination, or mental activity. However, not a single study was found that measures mental activity in yoga studies. Many studies in the field of mindfulness focus on outcomes that play an important role in Buddhism, such as compassion 112 –114 and non-attachment. 102,115,116 Future research in the field of yoga should focus more not only on positive outcomes, but also on positive psychological constructs that are linked to those that are rooted in yoga philosophy and Hinduism such as moksha (meaning), ananda (bliss, happiness), buddhi (wisdom), or kaivalya (detachment). Using the theoretical frame work of the yoga philosophy could also shed new light on the psychological mechanisms behind yoga interventions and meditation in general.
Conclusions
PMH consists of three dimensions: psychological well-being, emotional well-being, and social well-being. This meta-analysis is the first address the efficacy of yoga in the development of PMH in a non-clinical adult population. The current body of research suggests that yoga is only associated with an increase in psychological well-being in comparison to no treatment. This finding may be counterintuitive; people who practice yoga expect that it will contribute to an increase in their mental health. This study addressed several possible explanations for the findings, including the small number of studies, the heterogeneity of the interventions, and the way mental health is being measured. More rigorous research is needed to draw definite conclusions on the effects of yoga on PMH.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.