
Abstract
Objective:
The aim of this study was to establish if the changes in sympathetic and parasympathetic activity (analyzed through heart-rate variability [HRV]) during ultrasound (US)-guided percutaneous needle electrolysis (PNE) is due to the effect of needle puncture only or of the PNE technique per se where the puncture and galvanic current are combined.
Methods:
This was an experimental, case-control study that took place at the University of Seville. Subjects were 36 male footballers who were randomly allocated to three groups: a control group (CG; 12 players), for whom HRV was recorded for 10 min, both at rest and during an exhaustive US examination of the patellar tendon and adjacent structures; a first experimental group (PNE group; 12 players), for whom HRV was recorded for 10 min, both at rest and during application of US-guided PNE in the patellar tendon; and a second experimental group (needle group; 12 players), for whom HRV was recorded for 10 min, both at rest and during application of US-guided PNE without electrical current in the patellar tendon. The outcome measures were the diameters of the Poincaré plot (SD1, SD2), stress score, and sympathetic/parasympathetic ratio.
Results:
There were no differences between groups in any baseline measurements, nor were there any significant differences between CG measurements (baseline vs. intervention). The PNE group exhibited statistically significant increases in SD1 (p = 0.01) and SD2 (p = 0.004) and statistically significant decreases in SS and S/PS ratio (p = 0.03), indicating increased parasympathetic and decreased sympathetic activity, respectively. The needle group exhibited statistically significant increases in SD2 (p = 0.02) and statistically significant decreases in SS (p = 0.02), indicating decreased sympathetic activity.
Conclusions:
The application of the US-guided PNE technique caused a measurable increase in parasympathetic activity (detected by HRV), which was due to the combination of needle puncture and electric current.
Introduction
U
Techniques involving puncture of the skin are common in physiotherapy. These procedures may use a mechanical stimulus, as in acupuncture or dry needling, 12,13 or apply electrical current, as in electroacupuncture, 14 stimulation of myofascial trigger points, 15 or electrostimulation using galvanic current. 1,2
In these procedures, in which needling is applied, alterations of the autonomous behavior have been observed during the technique application. Heart-rate variability (HRV) has been validated as an accurate tool to assess the status of the autonomic nervous system (both sympathetic and parasympathetic components) under various conditions. 16 –18 In fact, an autonomic imbalance, analyzed through HRV, has been shown in physiotherapy techniques involving puncture. Kitagawa et al. 19 suggested that acupuncture stimulation of trigger points of the tibialis anterior muscle transiently increases parasympathetic nerve activity. Others 20 –22 have shown increased sympathetic activity during acupuncture needling, which is generally followed by increased parasympathetic tone afterwards. De la Cruz et al. 23 showed US-guided PNE in men was associated with an autonomic imbalance characterized by greater parasympathetic activity. Occasionally, vasovagal reactions may occur. These clinical phenomena are mediated by the vagus nerve and characterized by lightheadedness and malaise. Exceptionally, vasovagal reactions may result in brief and reversible loss of consciousness (vasovagal syncope). The relevance of this finding to clinical practice lies in the avoidance of clinically significant vagal reactions (including syncope). Therefore, it is important to advise physiotherapists that this invasive technique should be performed with due care, and one must be fully prepared to attend to any adverse reaction.
For this reason, the aim of this study was to establish whether the changes in sympathetic and parasympathetic activity (analyzed through HRV) during US-guided PNE are due to the effect of needle puncture only or of the PNE technique per se where the needle puncture and galvanic current were combined. In other words, does galvanic current play any role in the autonomous changes observed?
Materials and Methods
Participants
A total of 36 members of an amateur male football club were studied, split randomly into three groups, each comprising 12 players: a control group (CG) and two experimental groups. Exclusion criteria were: (1) pathology in the patellar tendon; (2) a Personal Psychological Apprehension Scale (PPAS) score >37.524; (3) commonly accepted contraindications to PNE, including chronic joint disease, surgery, prosthesis, or osteosynthesis in the area of intervention, cardiac disease, neoplasia, coagulopathy, use of certain drugs (fluoroquinoles, anticoagulants, corticosteroids, or non-steroidal anti-inflammatories) 25 ; (4) any contraindications to needling per se, including unsurmountable fear of needles, history of adverse reaction to needling, immunocompromise, difficulty expressing feelings appropriately, and/or allergy to metals 25 ; and (5) epilepsy.
The local ethics committee approved the study, which complied with all the principles set out in the Declaration of Helsinki. All subjects signed informed written consent to participate in this study.
Procedures
First, all subjects filled in the PPAS, the general aim of which was to measure the psychological apprehension of the subjects during electrophysiotherapeutic treatment. This scale aims to evaluate, by means of the opinion and self-positioning of the subjects, an individual's degree of apprehension to the application of an electrical current. 24 Subsequently, HRV was recorded in the early morning and after fasting overnight. HRV was recorded for the CG for 10 min, both at rest and during an exhaustive US examination of the patellar tendon and adjacent structures using a high-resolution grayscale US machine (Logiq; GE Healthcare, Madison, WI) with a linear probe (12 MHz), according to European Society of Musculoskeletal Radiology guidelines. 26 HRV was recorded for two experimental groups: a first experimental group (PNE-G) for 10 min, both at rest and during application of US-guided PNE in the patellar tendon (Fig. 1); and a second experimental group (Needle-G) for 10 min, both at rest and during application of US-guided PNE in the patellar tendon without application of electric current.

Heart-rate variability recorded during application of ultrasound (US)-guided percutaneous needle electrolysis (PNE) in the patellar tendon. Subjects sat on the bed, leaning back on the recliner at an angle of 75° with a pillow below the knee.
The patellar tendon was selected because patellar tendinopathy is one of the most commonly accepted indications for this technique, 6,7 although all study participants had healthy patellar tendons and did not suffer from any patellar pathology. The US-guided PNE technique was applied using a specifically developed medically certified (Directive 93/42/EEC) device (EPI Advanced Medicine, Barcelona, Spain), which produces galvanic electricity through the negative electrode cathodic flow. This is applied using a modified electrosurgical scalpel that incorporates acupuncture needles (0.3 mm in diameter) of different lengths. The intensity can be adjusted by changing either the duration of stimulation or the output current (mA) of the device. Conversely, the machine's polarity is fixed (i.e., only cathodic flow is usable). During each procedure, all of which were performed by the same experienced operator, volunteers sat on the bed, leaning back on the recliner at an angle of 75° with a pillow below their knees (Fig. 1) in order to minimize the risk of any potential vagal reaction (Fig. 1). Finally, three US-guided precise applications at a fixed intensity of 3 mA for 3 s were performed, according to Valera-Garrido and Minaya-Muñoz's protocol. 27 The applications were in the tendon.
Measurement of HRV
A Firstbeat Bodyguard (Firstbeat Technologies, Jyväskylä, Finland) heart rate (HR) monitor was used to record HR data for 10 min in every session (at rest and during US or US-guided PNE). Data were downloaded from the devices to a computer using the Firstbeat Uploader software (Firstbeat Technologies), and all the RRI series were imported into the Kubios software package (University of Eastern Finland, Kuopio, Finland), which was used to calculate all HRV parameters. To calculate the autonomic balance, the HRV method commonly used for this purpose is based on the Poincaré plot. 28 This method reflects HRV fluctuations. 29 Physiologically, the transverse axis (SD1) is a measurement of the short-term changes in RRIs and is considered an indicator of parasympathetic activity. 30 The physiological meaning of the longitudinal axis (SD2) is not as clear, but it is thought that it reflects the long-term changes in RRIs, and it is considered an inverse indicator of sympathetic activity. 31 Naranjo et al. 32 recently defined two new indexes to facilitate the physiological interpretation of the Poincaré plot: the stress score (SS) and the sympathetic–parasympathetic ratio (S/PS), respectively. The SS is expressed as the inverse of the diameter SD2 multiplied by 1000, and it is considered to be directly proportional to sympathetic activity at the sinus node. The S/PS ratio is expressed as the quotient of SS and SD1, and it is considered to reflect autonomic balance, that is, the relationship between sympathetic and parasympathetic activity.
Statistical analysis
All variables were expressed as the mean and standard deviation, and the normality of the data distribution was evaluated using the Shapiro–Wilk test. Data were first analyzed using a two-factor repeated-measures analysis of variance with three between-group factors (CG vs. PNE-G, CG vs. Needle-G, and PNE-G vs. Needle-G) and one within-group factor (baseline vs. intervention). The Games–Howell post hoc test was used for multiple comparisons. Data were analyzed with IBM SPSS Statistics for Windows v.21 (IBM Corp., Armonk, NY), and statistical significance was set at p < 0.05.
Results
There were no significant baseline differences between the CG, PNE-G, and Needle-G in any demographic variables, including age (22.92 ± 4.32 vs. 24.25 ± 4.05 vs. 25.92 ± 5.35 years), weight (74.33 ± 12.17 vs. 76.08 ± 6.42 vs. 77.33 ± 8.02 kg), height (176.50 ± 6.63 vs. 181.83 ± 3.21 vs. 176.17 ± 5.20 cm), and body mass index (23.77 ± 2.77 vs. 23.29 ± 2.13 vs. 24.92 ± 2.46 kg/m2). On the PPAS scale, the control and two experimental groups scored 23.17 ± 4.51, 22.50 ± 4.87, and 22.17 ± 4.39 (p > 0.05).
Table 1 shows the mean and standard deviation (SD) of the study variables (mean NN interval, mean HR, SD1, SD2, SS, and S/PS ratio) at rest (baseline measurement) and during US examination or application of the US-guided PNE technique or application of the US-guided PNE technique without electric current in the control, PNE, and needle groups, respectively. Table 1 also shows the difference (Δ, in %) between before and after interventions in each group.
Heart-rate variability (HRV) parameters before and during intervention in each group. The mean ± SD for each HRV parameter and group, and the difference (Δ, in %) between before and during interventions in the control, PNE group, and needle group consisted of US examination, US-guided PNE, and US-guided PNE without electric current, respectively.
p < 0.05 baseline versus intervention scores for PNE group and needle group.
p < 0.05 significant difference during intervention between PNE group and needle group.
US, ultrasound; PNE, percutaneous needle electrolysis; NN interval, normal RR interval (RRI); HR, heart rate; bpm, beats per minute; SD1, transverse axis of Poincaré plot; SD2, longitudinal axis of Poincaré plot; SS, stress score (inverse of diameter SD2 × 1000); S/PS ratio, quotient of SS and SD1.
There were no differences between the CG and two experimental groups in the baseline measurements of NN interval (p > 0.05).
There were no significant differences between the CG measurements taken at baseline and during the US examination (p > 0.05). By contrast, compared with baseline values, the PNE-G exhibited statistically significant increases in the following two parameters of HRV during intervention: SD1 (72.93 ± 31.17 vs. 42.22 ± 15.22; p = 0.01) and SD2 (189.15 ± 55.99 vs. 120.08 ± 47.74; p = 0.004). This group also exhibited statistically significant decreases in the following two parameters of HRV during intervention: SS (5.72 ± 1.68 vs. 9.73 ± 4.16; p = 0.03) and S/PS ratio (0.09 ± 0.06 vs. 0.31 ± 0.28; p = 0.03). Compared with baseline values, the Needle-G exhibited statistically significant increases in SD2 (142.06 ± 44.74 vs. 103.14 ± 28.53; p = 0.02) and statistically significant decreases in SS (7.71 ± 2.51 vs. 10.48 ± 3.26; p = 0.02) during intervention.
Figure 2 shows the comparison between the PNE-G and Needle-G during US-guided PNE technique or US-guided PNE technique without electric current, respectively. There were statistically significant differences in SD2 (189.15 ± 55.99 vs. 142.06 ± 44.74; p = 0.03), SS (5.72 ± 1.68 vs. 7.71 ± 2.51; p = 0.03), and ratio S/PS (0.09 ± 0.06 vs. 0.21 ± 0.25; p = 0.04).
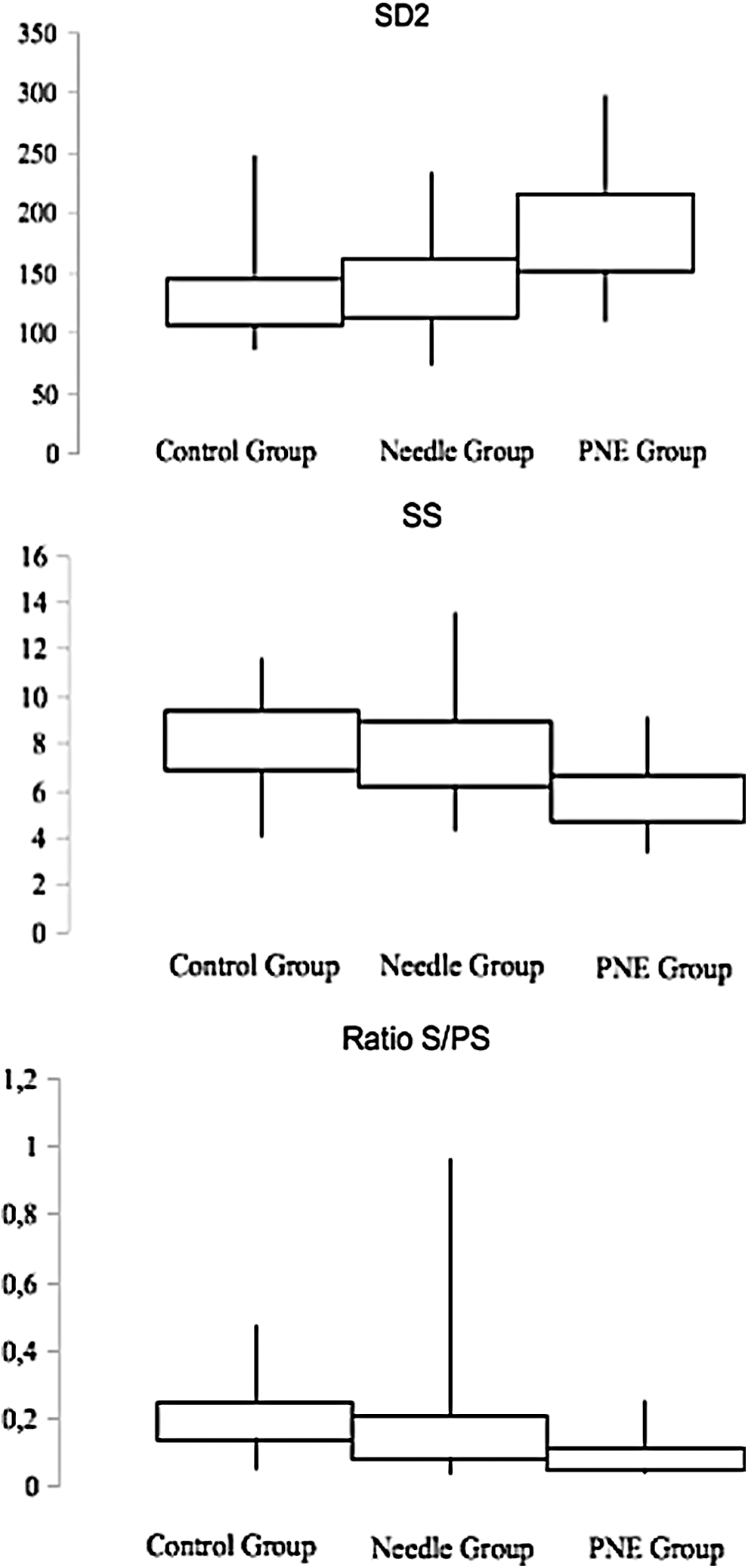
Box-and-whiskers plot of SD2, SS, and ratio S/PS during US examination, US-guided PNE, and US-guided PNE without electric current, in control, PNE, and needle groups, respectively. The box represents the lower and upper quartiles, and the whiskers represent the total range. SD1, transverse axis of Poincaré plot; SD2, longitudinal axis of Poincaré plot; SS, stress score; S/PS, quotient of SS and SD1.
Figure 3 shows the comparison of SD1, SS, and S/PS ratio between the three groups.
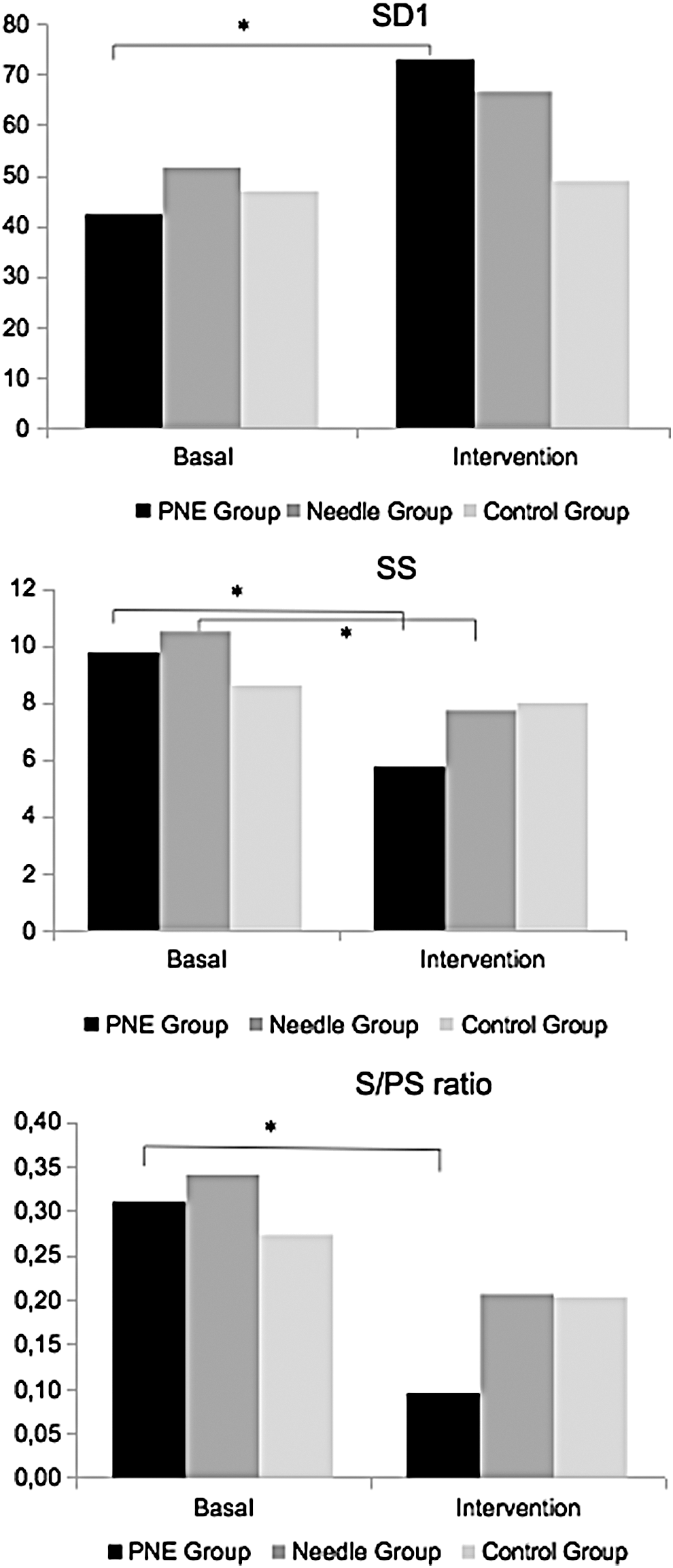
Comparison of SD1, SS, and S/PS ratio between baseline and the intervention for each group. *p < 0.05.
Discussion
The main finding of this study was a significant autonomic imbalance (in keeping with a potential vasovagal reaction) during application of the US-guided PNE technique in healthy patellar tendons of male football players by means of simple HRV measurements. The relevance of this finding to clinical practice lies in the avoidance of clinically significant vasovagal reactions (including syncope). Therefore, it is important to advise physiotherapists that this invasive technique should be performed with due care, and one must be fully prepared to attend to any adverse reaction.
In the PNE-G, a statistically significant increases were observed in the marker of parasympathetic activity, SD1 (p = 0.01). Furthermore, a statistically significant increase was found in SD2 (p = 0.004), which is indicative of decreased sympathetic activity, as well as a statistically significant decrease in SS and S/PS ratio (p = 0.03). Overall, this suggests that the application of the US-guided PNE technique causes an autonomic imbalance with a predominance in parasympathetic activity (Fig. 3). However, in the Needle-G, a statistically significant increase in SD2 (p = 0.02) was demonstrated, which is indicative of decreased sympathetic activity, as well as a statistically significant decrease in SS (p = 0.02). Overall, this suggests that the application of the US-guided PNE technique without application of electrical current causes an autonomic imbalance but not large enough to be a predominance in parasympathetic activity. When the PNE-G and Needle-G were compared during the application of the US-guided PNE technique or application of the US-guided PNE technique without electric current, respectively, there were a statistically significant differences in SD2, SS, and ratio S/PS. Only the PNE-G during intervention showed a decrease in sympathetic activity enough to affect the balance between parasympathetic and sympathetic activity, reflected as ratio S/PS (Fig. 3). This result could be because the difference between before and during the interventions in the PNE-G was higher than in the Needle-G (Table 1). This means that the combination of needling and electric current was a cause of vagal response. However, these results have a positive effect because this technique causes a segmentary response (central nervous system activation) that starts the repair processes. This is known as the response of the organism to a threat (fight–flight response). 33,34
In this particular study, it would appear that this autonomic imbalance was elicited by the needling technique per se, regardless of the participants' attitudes, which were generally positive. In fact, subjects in both control and experimental groups scored an average of 23 points on the PPAS, which is much less than the threshold of 37.5 that is considered to indicate apprehension. 24 Thus, it appears unlikely that any study subject manifested any significant degree of apprehension to the needling or the electrical current that may otherwise have had an impact on the results. Consequently, the HRV changes were attributable to the study's physiotherapy technique, which it is considered important to acknowledge in order to avoid serious vasovagal reactions such as vasovagal syncope.
The analysis of HRV has been applied to several pathological conditions 16 in addition to sports performance. 17,18 In this context, papers on HRV have been identified involving therapeutic massage, 35 –37 craniosacral therapy, 38 acupuncture, 39 –41 and PNE. 23 Some authors have reported an increase in HRV based on increased parasympathetic activity that has been translated into techniques designed to reduce physiological stress. 35,36,38 Other authors have reported increased sympathetic activity during acupuncture needling, which is generally followed by increased parasympathetic tone afterwards. 39 –41 In this study, comparing two experimental groups of homogeneous subjects, a trend toward increased parasympathetic activity and decreased sympathetic activity was observed in both groups, although the changes were only statistically significant in the PNE-G. In light of the fact that US-guided PNE is a needling technique, it is likely that subjects were experiencing an autonomic imbalance, and this should be borne in mind during clinical treatment to avoid potentially serious adverse reactions such as vasovagal syncope.
Limitations and recommendations
The PNE technique causes an autonomic imbalance. Therefore, the technique has a local and a segmental effect. It would be interesting for future studies to clarify the local and segmental therapeutic mechanisms of this technique.
However, HRV changes are different between females and males. 42 –44 Generally, women have a higher prevalence of parasympathetic activity than men do, and therefore women show greater HRV. 42 Also, it would be interesting for future studies to determine the autonomic response to PNE in women.
Conclusion
In conclusion, application of the US-guided PNE technique caused a measurable increase in parasympathetic activity (detected by HRV), which was due to the combination of needle puncture and electric current.
Footnotes
Author Disclosure Statement
There are no financial interests to disclose.